Anna Belloni-Fortina1, Maria Cristina Montesco2, Stefano Piaserico1, Matteo Bordignon1, Francesco Tona3, Giuseppe Feltrin3 and Mauro Alaibac1
Units of 1Dermatology, 2Pathology, and 3Cardiosurgery, University of Padua, Padua, Italy



Anna Belloni-Fortina1, Maria Cristina Montesco2, Stefano Piaserico1, Matteo Bordignon1, Francesco Tona3, Giuseppe Feltrin3 and Mauro Alaibac1
Units of 1Dermatology, 2Pathology, and 3Cardiosurgery, University of Padua, Padua, Italy
Solid organ transplant recipients are at risk of developing a wide range of viral-associated malignancies, including skin tumours and lymphoproliferative disorders. The risk of a post-transplant lymphoproliferative disorder is 28–49 times the risk of a lymphoproliferative disorder in the normal population. Most cases are of B-cell phenotype and are associated with Epstein-Barr virus infection. Post-transplant lymphoproliferative disorders presenting clinically in the skin are rare and usually of B-cell phenotype. Only rare cases of cutaneous T-cell post-transplant lymphoproliferative disorder have been reported previously, mostly mycosis fungoides type. We describe here a rare primary cutaneous T-cell lymphoma CD30+ arising in a heart transplant patient who had a nodule on the right leg, several years after heart transplantation. The morphology and immunohistochemical findings were consistent with a CD30+ anaplastic large cell lymphoma with a T-cell phenotype. Excisional biopsy and radiotherapy of the affected area were performed. In this patient, the presence of a solitary lesion and the lack of systemic involvement represented the main factors taken into account in choosing the therapy and the patient was therefore treated using a non-aggressive approach, although with systemic immunosuppression. In conclusion, the diagnosis of a CD30+ anaplastic large cell lymphoma in transplant recipients does not imply aggressive clinical behaviour by the lymphoma. Key words: CD30-positive; cutaneous T-cell lymphoma; transplantation; anaplastic large cell lymphoma.
(Accepted May 20, 2008.)
Acta Derm Venereol 2009; 89: 74–77.
Mauro Alaibac, Unit of Dermatology, University of Padua, Via Cesare Battisti 206, IT-35121 Padova, Italy. E-mail: mauro.alaibac@unipd.it
After gastrointestinal localizations, skin is the most involved site for non-Hodgkin’s lymphoma (1). Primary cutaneous lymphomas are defined as cutaneous T-cell lymphomas (CTCLs) and cutaneous B-cell lymphomas (CBCLs) that present in the skin with no evidence of extracutaneous disease at the time of diagnosis (2). Among CTCLs, CD30-positive cutaneous T-cell lymphoma (CD30+CTCL) is the second most common group; it represents approximately 30% of cutaneous primary T-cell lymphoproliferative disorders (3). In the World Health Organization – European Organisation for Research and Treatment of Cancer (WHO-EORTC) classification of cutaneous lymphomas (2), the CD30+CTCL group comprises primary cutaneous anaplastic large cell lymphoma (ALCL) and lymphomatoid papulosis (LP). ALCL presents large cells with an anaplastic, pleiomorphic or immunoblastic cytomorphology with a CD30 antigen expression in more of 75% of neoplastic cells; it usually affects adults, with a male:female ratio of 3:1; clinically, ALCL shows nodules or papules, often ulcerated, in single or multiple lesions; these lesions could have a spontaneous resolution but with possible recurrence; 10% of patients have local node involvement; the 10-year survival rate is greater than 90% for both solitary and multifocal lesions (4).
LP is characterized by papular, papular-necrotic and nodular skin lesions, usually localized in the trunk, arms and legs; the lesions usually undergo spontaneous resolution in 3–12 weeks but often reappear after a variable period of time; 20% of patients with LP may present a more aggressive lymphoproliferative disorder (5).
Hodgkin’s and non-Hodgkin’s lymphomas are a not infrequent complication in transplant organ recipients and they are usually aggressive diseases, with nodal and extranodal localizations, generally B-cell lymphomas, often Epstein-Barr virus (EBV)-related (6, 7). Possible regression after immunosuppressive regimen reduction has been shown (8). Whereas skin is often involved in transplant organ recipient carcinogenesis (e.g. squamocellular carcinoma, basocellular carcinoma, malignant melanoma and Kaposi’s sarcoma), cutaneous lymphomas are extremely rare and their incidence has not been established. Seventy percent of reported cases are CBCL, whereas 30% are CTCL (9).
We describe here a case of cutaneous anaplastic CD30+ T-cell lymphoma in a transplant organ recipient and review the literature concerning CD30+ cutaneous lymphomas in this group of patients.
Case report
In January 2005 a 68-year-old Caucasian man, heart-transplanted in 1994, under immunosuppressive therapy with cyclosporin A (175 mg/day) and azathioprine (100 mg/day) was referred to our unit. Skin examination revealed a reddish oval nodule, about 2 cm in diameter on the lateral side of the left leg (Fig. 1). An excisional biopsy of the lesion was performed and histological analysis showed an atypical, non-epidermotropic cellular infiltrate of the entire dermal compartment; this infiltrate was composed of large anaplastic cells with eosinophilic cytoplasm and numerous and prominent nucleoli (Fig. 2). Atypical mitosis were also identified. The neoplastic cells were CD3+, CD4+ CD30+ (Fig. 3). We observed also a weak positivity for CD5 molecule (expressed in approximately 30% of the lymphoid infiltrate) and a reduced expression of the CD1a molecule in both the dermal and epidermal compartments. The patient was properly staged (serum and instrumental examinations, bone marrow biopsy) and no extracutaneous manifestation of disease was found. On the basis of clinical, histological and immunophenotypical data a diagnosis of primary cutaneous anaplastic CD30+ T-cell lymphoma was made. After surgical removal, local radiotherapy was performed. No variation was made in the immunosuppressive drug regimen. After a 2-year follow-up, complete remission persists.

Fig. 1. Appearance of the lesion: reddish, oval nodule, approximately 2 cm in diameter, not ulcerated.
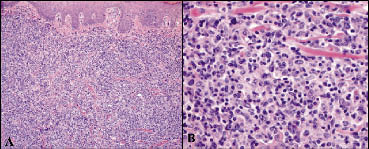
Fig. 2. Histological features of the lesion. (A) Diffuse dermal infiltration without epidermotropism. Large anaplastic cells with eosinophilic cytoplasm and numerous and prominent nucleoli. (B) Atypical mitosis was also observed. Haematoxylin & eosin (H&E); original magnifications: (A) ×10; (B) ×40.
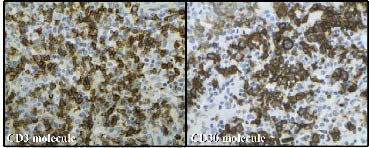
Fig. 3. Immunohistochemical staining of most atypical cells with monoclonal antibodies directed against the CD3 and CD30 molecules. Immunoperoxidase stain for (A) CD3 and (B) CD30. Original magnification ×40.
Discussion
Post-transplant cutaneous lymphoproliferative disorders (PTCLDs) are a rare complication. To date, it has not been demonstrated whether a major incidence of primary cutaneous lymphoma does exist in immunosuppressed patients. Nevertheless, a role of immunosuppressive therapy in the development of PTCLDs could be speculated. Reduction of immune surveillance, chronic antigenic stimulation by the transplanted organ and direct oncogenetic potential of immunosuppressive drugs could be considered risk factors for PTCLDs in transplant recipients. To the best of our knowledge, eight cases of ALCLs have been reported (Table I) (10–17). The clinical behaviour of these cases seems to be more aggressive compared with the non-immunosuppressed population. In most of these cases, multiple lesions were present at the first observation and new nodules were noticed a few months after diagnosis. Systemic chemotherapy and variation of the original immunosuppressive regimen were often necessary, with a very poor prognosis in 50% of cases. The majority of PTCLDs observed were found at least 5 years after solid organ transplantation.
Table I. Summary of cases of primary cutaneous anaplastic CD30+ T-cell lymphoma (CTCL) in organ transplant recipients reported in the literature
| Author, year (Ref) | Sex/age (years) | Transplant | Immunosuppressive drugs | Time* (months) | Skin examination | Therapy and outcome |
| Ward HA, et al. 2001 (10) | F/64 | Kidney | Pred, CyA, Aza | 56 | Erythematous eruption on face and trunk, with papules and hyperpigmented nodules | Deceased after ECP and RT |
| Seckin D, et al. 2001 (11) | F/51 | Kidney | Pred, CyA, Aza | 10 | Reddish and rapidly growing nodule on the left gluteus | Remission after 5 months from RT (cumulative dose 166 Gy) |
| Cooper SM, et al. 2003 (12) | M/60 | Kidney | M. mofetil, Pred, CyA | 66 | Asymptomatic and multiple nodules localized on the left arm | Deceased after local RT and CT |
| Coyne JD, et al. 2004 (13) | F/33 | Kidney | Pred, CyA, Aza | 25 | Cutaneous nodules localized on abdomen, thorax, right upper and lower extremities | Deceased after CyA and Aza reduction and Pred and acyclovir augmentation |
| Kim HK, et al. 2004 (14) | M/56 | Kidney | Pred, CyA, Aza | 192 | Polypoid mass localized on the forehead | CR 10 months after 6 cycles of CT |
| Lucioni M, et al. 2004 (15) | M/63 | Heart | RATG, Aza, CyA, Pred | 111 | Nodules and multiple plaque, some ulcero-necrotic, in the back side of lower extremities | CR 49 months after therapy with IgG, IFN-α and CHOP |
| Salama S, et al. 2005 (16) | M/59 | Kidney | – | 72 | Multiple nodules localized on the left leg | Deceased |
| Denisi MC, et al. 2005 (17) | M/49 | Heart | M. mofetil, tacrolimus, Pred | 60 | Brownish, indolent, not ulcerated nodule localized on the left cheek | CR, after surgical removal and RT |
| Present case 2007 | M/68 | Heart | CyA, Aza | 121 | Reddish, indolent, not ulcerated nodule localized on the left lower extremity | CR, after surgical removal and RT |
*Time between transplant and CTCL.
CyA: cyclosporin A; Pred: prednisolone; Aza: azathioprine; CT: chemotherapy; RT: radiotherapy; CR: complete remission; ECP: extracorporeal photopheresis; CHOP: cyclophosphamide, hydroxydaunorubicin, oncovin, predrisolone; RATG: rabbit anti-thymocyte globulins.
The clinical behaviour, histological and immunophenotypical features of our case were not different from ALCLs of immunocompetent patients. The disease was not aggressive and complete remission still persists after 2 years. The presence of a solitary lesion at the time of diagnosis has represented the main prognostic factor in our case, and for this reason we treated the patient by means of a non-aggressive approach (surgical excision and local radiotherapy) without the necessity for systemic chemotherapy or variation of the immunosuppressive regimen.
In conclusion, we present here a case of ALCL in a heart transplant patient. This particular type of PTCLD showed a not aggressive clinical behaviour that was similar to other published cases with a solitary lesion at the time of diagnosis. We conclude that the diagnosis of ALCL in transplant recipients does not imply aggressive clinical behaviour by the lymphoma and consequently the therapeutic approach should be modulated according to clinical presentation.
References
1. Groves FD, Linet MS, Travis LB, Devesa SS. Cancer surveillance series: non-Hodgkin’s lymphoma incidence by histologic subtype in the United States from 1978 through 1995. J Natl Cancer Inst 2000; 92: 1240–1251.
2. Willemze R, Jaffe ES, Burg G, Cerroni L, Berti E, Swerdlow SH, et al. WHO-EORTC classification for cutaneous lymphomas. Blood 2005; 105: 3768–3785.
3. Willemze R, Beljaards RC. Spectrum of primary cutaneous CD30 (Ki-1)-positive lymphoproliferative disorders. A proposal for classification and guidelines for management and treatment. J Am Acad Dermatol 1993; 28: 973–980.
4. Bekkenk MW, Geelen FA, van Voorst Vader PC, Heule F, Geerts ML, van Vloten WA, et al. Primary and secondary cutaneous CD30(+) lymphoproliferative disorders: a report from the Dutch Cutaneous Lymphoma Group on the long-term follow-up data of 219 patients and guidelines for diagnosis and treatment. Blood 2000; 95: 3653–3661.
5. Liu HL, Hoppe RT, Kohler S, Harvell JD, Reddy S, Kim YH. CD30+ cutaneous lymphoproliferative disorders: the Stanford experience in lymphomatoid papulosis and primary cutaneous anaplastic large cell lymphoma. J Am Acad Dermatol 2003; 49: 1049–1058.
6. Penn I. Cancers complication in organ transplantation. N Engl J Med 1990; 323: 1767–1769.
7. Caillard S, Lachat V, Moulin B. Posttransplant lymphoproliferative disorders in renal allograft recipients: report of 53 cases of a French multicenter study. PTLD French Working Group. Transpl Int 2000; 13: S388–S393.
8. Knowles DM, Cesarman E, Chadburn A, Frizzera G, Chen J, Rose EA, Michler RE. Correlative morphologic and molecular genetic analysis demonstrates three distinct categories of posttransplantation lymphoproliferative disorders. Blood 1995; 85: 552–565.
9. Euvrard S, Kanitakis J, Claudy A. Skin cancers after organ transplantation. N Engl J Med 2003; 348: 1681–1691.
10. Ward HA, Russo GG, McBurney E, Millikan LE, Boh EE. Posttransplant primary cutaneous T-cell lymphoma. J Am Acad Dermatol 2001; 44: 675–680.
11. Seckin D, Demirhan B, Oguz Gulec T, Arikan U, Haberal M. Posttransplantation primary cutaneous CD30 (Ki-1)-positive large-cell lymphoma. J Am Acad Dermatol 2001; 45; S197–S199.
12. Cooper SM, Turner GD, Hollowood K, Gatter K, Hatton C, Gray D, et al. Primary cutaneous large cell CD30+ lymphoma in a renal transplant recipient. Br J Dermatol 2003; 149: 426–428.
13. Coyne JD, Banerjee SS, Bromley M, Mills S, Diss TC, Harris M. Post-transplant T-cell lymphoproliferative disorder/T-cell lymphoma: a report of three cases of T-anaplastic large-cell lymphoma with cutaneous presentation and a review of the literature. Histopathology 2004; 44: 387–393.
14. Kim HK, Jin SY, Lee NS, Won JH, Park HS, Yang WI. Posttransplant primary cutaneous Ki-1 (CD30)+/CD56+ anaplastic large cell lymphoma. Arch Pathol Lab Med 2004; 128: 96–99.
15. Lucioni M, Ippoliti G, Campana C, Cavallini D, Incardona P, Viglio A, et al. EBV positive primary cutaneous CD30+ large T-cell lymphoma in a heart transplanted patient: case report. Am J Transplant 2004; 4: 1915–1920.
16. Salama S. Primary “cutaneous” T-cell anaplastic large cell lymphoma, CD30+, neutrophil-rich variant with subcutaneous panniculitic lesions, in a post-renal transplant patient: report of unusual case and literature review. Am J Dermatopathol 2005; 27; 217–223.
17. De Nisi MC, D’Amuri A, Lalinga AV, Occhini R, Biagioli M, Miracco C. Posttransplant primary cutaneous CD30 (Ki-1)-positive anaplastic large T-cell lymphoma. A case report. Br J Dermatol 2005; 152: 1068–1070.

