Ryoko Shimada, Taku Fujimura*, Yumi Kambayashi, Tomoyuki Ohtani, Mei Nasu, Yukikazu Numata, Takahiro Haga, Akira Hashimoto and Setsuya Aiba
Department of Dermatology, Tohoku University Graduate School of Medicine, Seiryo-machi 1-1, Aoba-ku, Sendai, 980-8574, Japan. *E-mail: tfujimura1@mac.com
Accepted January 18, 2012.
Merkel cell carcinoma (MCC) is an aggressive, cutaneous, neuroendocrine carcinoma (1). The outcomes remain poor for patients with metastatic disease, with a median survival of only 10 months (1). The biology and clinical course of MCC may be immunologically mediated. For instance, spontaneous regression has been reported, and a significant increase in tumour-infiltrating lymphocytes has been observed in biopsy lesions that have subsequently regressed, suggesting a causal anti-tumour immune response (2).
Xanthogranulomas in adults are observed on the skin and are rarely associated with haematological malignancies. The histopathological hallmark of xanthogranuloma is the Touton cell and collections of macrophages that have vacuolated cytoplasm. Guo & Wang (3) have reported that these macrophages are positive for CD68 and CD163, which suggests that these macrophages may be alternative tumour-associated macrophages.
We describe here a case of adult xanthogranuloma developing from irradiated MCC. This observation may suggest a poor prognosis in patients who have undergone radiation therapy for MCC.
CASE REPORT
An 83-year-old Japanese man visited our outpatient clinic with a 3-month history of an asymptomatic, pedunculated nodule approximately 2 cm in diameter on his right cheek. On his initial visit, physical examination revealed a red-coloured, elastic-soft, 20 × 25 mm, well-demarcated nodule on the side of his right cheek (Fig. 1A). In addition, there was an elastic-hard, subcutaneous nodule, 20 mm in diameter, on the right side of his neck. Biopsy specimen from his cheek revealed sheets of small cells with hyperchromatic nuclei extending throughout the dermis (Fig. 2A). Immunohistochemical staining revealed that these tumour cells were mainly positive for CK20 (Fig. 2B), weakly positive for synaptophysin, Neuron-specific enolase (NSE), chromogranin A, and negative for CD20 and Thyroid transcription factor 1 (TTF-1). From the above data, we diagnosed MCC. In addition, we excised the subcutaneous tumour on his neck, which histologically showed lymph node metastasis of MCC. For treatment of the primary tumour, we applied radiation therapy to his right cheek and right neck, 60 Gy in 30 fractions, and the tumour on the right cheek was diminished in 6 weeks after the radiation therapy. We screened for a possible internal malignancy with computed tomography (CT) scan, but found none. Interestingly, after the radiotherapy, a yellowish, elastic, tumour, 2 cm in size, appeared on his cheek (Fig. 1B). The biopsy specimens revealed many histiocytes with foamy cytoplasma and inflammatory cells and Touton type giant cells were infiltrated throughout the dermis. We diagnosed this tumour as xanthogranuloma (Fig. 2C). Immunohistochemical staining revealed that these histiocytes were positive for CD163 (Fig. 2D). Two months after the end of radiation therapy, a subcutaneous nodule suddenly appeared on a left side of the abdomen. We surgically excised this tumour, which appeared to be the metastatic lesion of MCC. After excision, we screened for a possible internal malignancy with positron emission tomography (PET) and found multiple systemic metastases of the tumour, including metastasis to the pancreas and lymph nodes, although we could not detect any internal malignancy before the surgical treatment by CT scan.
Fig. 1. (A) A red-coloured nodule, 20×25 mm in size, on the right cheek and a lymphnode swelling on the neck (marked). (B) A yellowish, elastic, tumour, 2 cm in size, appeared on the patient’s cheek after radiotherapy.
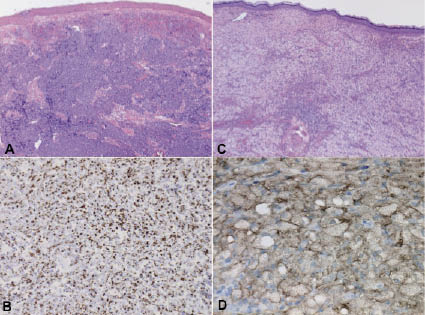
Fig. 2. (A) Sheets of small cells with hyperchromatic nuclei extending through out the dermis. (B) The tumour cells were mainly positive for CK20. (C) Many histiocytes with foamy cytoplasm and inflammatory cells and Touton types giant cells were infiltrated throughout the dermis. (D) The histiocytes were positive for CD163 (original magnification: (A, C) × 100, (B) × 200, (D) × 400).
DISCUSSION
Cotter et al. (2) reported recently the immunomodulatory effect of radiation therapy, namely that localized radiation therapy stimulated lymphocytes to infiltrate the tumour and activated the innate immune system via both toll-like receptors and the NKG2D receptor signal pathway. Indeed, for the treatment of MCC, a recent report also suggested that radiotherapy alone for MCC achieved similar outcomes compared with conventional surgical treatment (4). In the future, more patients with MCC are expected to undergo local radiotherapy for the initial treatment, and, therefore, dermatologists should be able to recognize the possible symptoms developing at radiation ports.
Xanthogranulomas in adults are lesions defined histopathologically as collections of macrophages that have vacuolated cytoplasm. Currently, Cohen & Prieto (5) reviewed benign tumours that developed in radiation ports. In their report, one case of xanthogranuloma arising from a port of radiation therapy for breast cancer is described (5). To the best of our knowledge, their report is the only case describing xanthogranuloma arising from a radiation port, and our case is the second report.
It is still unclear whether xanthogranuloma is the principal sign for tumour-bearing individuals. As described above, xanthogranuloma is defined histopathologically as collections of macrophages. However, we still do not know whether these macrophages are immunogenic or immunosuppressive. Interestingly, a recent report suggested that macrophages in xanthogranuloma are mainly positive for CD163, which suggest that these macrophages might be suppressive tumour-associated macrophages. Moreover, Werchau et al. (6) reported that lymphangiogenesis in MCC was driven by VEGF-C+ CD68+ CD163+ M2 alternative tumour-associated macrophages. In addition, more recently, it was reported that some variants of immature macrophages, which are also known as myeloid-derived suppressor cells (MDSC), are positive for NKG2D and suppress the immune response in local sites of tumours and are associated with a poor prognosis (7). In this respect, xanthogranulomas arising from radiation ports may be related to a poor prognosis of the tumour-bearing host. In fact, in our present case, 2 months after the radiation therapy, we detected distant, multiple metastases of MCC. Further research is required in order to confirm this hypothesis.
REFERENCES