


Ole Martin Rørdam1, Øystein Grimstad1, Olav Spigset2,3* and Kristin Ryggen1
Departments of 1Dermatology and 2Clinical Pharmacology, St Olavs Hospital, Trondheim University Hospital, NO-7006 Trondheim, and 3Department of Laboratory Medicine, Children’s and Women’s Health, Norwegian University of Science and Technology, Trondheim, Norway. *E-mail: olav.spigset@legemidler.no
Accepted September 19, 2012.
Orf, also known as contagious ecthyma or contagious pustular dermatitis, is a viral skin infection caused by a parapoxvirus (1). It typically manifests as a nodule of the hands that heals spontaneously within 3–6 weeks, but other sites such as the head and scalp, are occasionally involved. Orf is common among persons with regular contact with sheep and goats, including farmers, butchers and veterinary surgeons (1). In immunocompromised patients the infection many cause lesions with excessive growth and be long-lasting and difficult to treat. Several cases of orf have been reported in patients using immunosuppressive medications, such as glucocorticoids, cyclosporine, mycophenolate and tacrolimus, after transplantations (2–5), but to our knowledge this is the first report of giant orf in a patient treated with a tumour necrosis factor (TNF) inhibitor.
CASE REPORT
The patient was a 45-year-old man treated for psoriatic arthritis with etanercept (Enbrel) 50 mg per week for 2 years. He had been a sheep farmer for 28 years, but had never been infected with orf before, although he had observed crusts in the oral area of his lambs, which were probably orf infections, for many seasons previously. The lambs were out at grass all summer, and in the autumn they should be given an oral anti-parasitic solution. In relation to this episode he observed that a few of the lambs had crusts around the mouth. While handling the lambs his face was exposed to saliva from 2 different lambs. On that occasion, he already had an abrasion in the temporal area from an unrelated activity.
After this episode the patient developed a rapidly growing tumour in the right temporal area over a period of 3 months and at the same time a more slowly growing tumour on a finger. Clinical examination showed an exophytic, lobulated and raspberry-like structure rising 5–6 cm above the temporal surface, with the largest transverse diameter of 7 cm (Fig. 1). He also had a typical, but far smaller, lesion on the third finger of the left hand. Histological examination confirmed the clinical diagnosis.
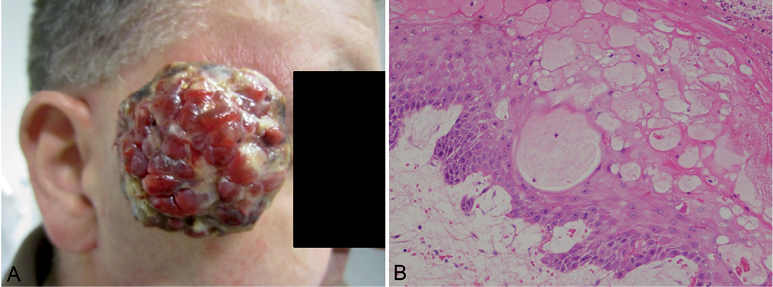
Fig. 1. (A) Initial presentation of the temporal giant orf lesion. (B) Histopathology of the lesion, showing intracellular oedema in the epidermis with enlarged and vacuolated epidermal keratinocytes (ballooning)(Haematoxylin and eosin staining, original magnification x 400).
As only a few cases of giant orf have been reported in immunosuppressed patients, management of this patient category has not been clearly established. In single cases, treatment with topical cidofovir (2) or imiquimod (5) has been successful, and the use of cryotherapy (3) and surgical excision (4) has also been described. Due to the large size of the temporal lesion in our patient, it was considered that topical antiviral therapy would be futile. Therefore, surgical removal was chosen as initial treatment, being fully aware that some degree of scarring could be expected at the site of surgery. The tumour was excised under local anaesthesia (lidocaine 0.1 mg/ml with adrenalin), in a tangential fashion like a shave excision. The base of the tumour was rough and difficult to cut through, and there were several fragile blood vessels in the pedicle. Aluminium chloride 35% and sliver nitrate were used for haemostasis, followed by local compression. The wound was then treated with cryotherapy (liquid nitrogen), with a freezing time of 30 s, applied twice. Etanercept was discontinued.
Control after one week showed no signs of regrowth and healing had proceeded as expected. A part of the tumour was treated with cryotherapy once more. Three weeks after surgery there were signs of progression of the finger lesion, and 6 satellite tumours had appeared in the temporal region. Therefore, cryotherapy was also applied here, and treatment with imiquimod was started on all lesions.

Fig. 2. Appearance of the temporal area 18 weeks after surgical removal of the tumour and 4 weeks after the final cryotherapy treatment.
Cryotherapy was repeated every third to fourth week during the next months, and he used imiquimod on a daily basis. Over this period the lesions gradually diminished, until they finally disappeared 17 weeks after start of therapy, i.e. 30 weeks after the patient had discovered the first tumour. As a safety precaution it was decided to wait a further 3 months before commencement of therapy with etanercept.
DISCUSSION
As an immune evasion strategy, orf virus encodes several immunomodulatory or inflammation-active genes, through which the virus interferes with both innate and adaptive immune responses in the host. Of these, viral homologues of vascular endothelial growth factor-E (VEGF-E) and interleukin-10 (IL-10) are of particular interest (1, 6). The viral VEGF functions in the same way as human VEGFs, causing vascular proliferation and permeability, features observed in the lesion in our patient. IL-10 exhibits immunosuppressive activity by inhibiting the release of human proinflammatory cytokines and chemokines such as TNF, IL-6 and CXCL-8, and it also suppresses the immune response by inhibiting antigen presentation and the production of interferon-γ (1, 7, 8).
It is well known that treatment with TNF inhibitors, such as etanercept, facilitates the risk of viral infections (9, 10). Recently, the evidence has been reviewed for viral hepatitis, varicella-zoster infections, mononucleosis, cytomegalovirus infections, and others (9). However, orf is not discussed (9). In the manufacturer’s product information for Enbrel, the increased risk of severe infections is acknowledged and several viral infections are specified, including hepatitis B and herpes zoster, but not orf (10).
TNF is an important cytokine in host defence against virus, and an enhanced risk of viral infections during treatment with etanercept is reported. This suggests that etanercept both increased the susceptibility of orf and contributed to the excessive growth of the tumour in our patient. Thus, our case illustrates the importance of TNF signalling in the immune response to orf virus infection in the skin. Moreover, this case demonstrates the effect of an integrated treatment consisting of tumour excision, cryotherapy and imiquimod. However, even though intensive therapy was started and the etanercept was swiftly discontinued, the recovery phase was remarkably prolonged.
ACKNOWLEDGEMENT
We thank Harald Aarset for histopathological interpretation.
The authors declare no conflicts of interest.
REFERENCES

