


Marion Fenot1, Vincent Lassalle2, Hervé Maillard1, Louis-Rémi De Ybarlucea3 and Philippe Celerier1
Departments of 1Dermatology, 2Intensive Care, and 3Anatomopathology, Hospital Center, 194 avenue Rubillard, FR-72000 Le Mans, France. E-mail: mfenot@ch-lemans.fr
Accepted November 5, 2012.
Shock revealing a lymphoma is rare. We report here 2 cases of lymphoma revealed by the association of atypical shocks and skin lesions.
Case reports
Case 1.
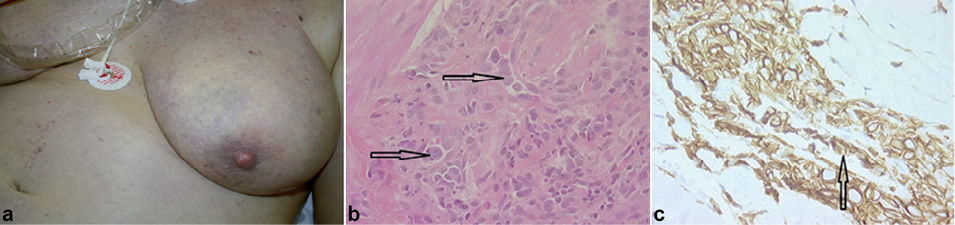
A 56-year-old woman was hospitalized because of febrile dyspnoea. She was not taking any regular medication. A full infectious, immunological and radiological work-up was inconclusive. Despite empirical antibiotic treatment targeted against intracellular bacteria (levofloxacin), haemophagocytic syndrome developed and haemodynamic instability prompted a transfer to the intensive care unit (ICU). Echocardiography revealed an altered cardiac output. Respiratory assistance and haemodynamic support with vasoactive amines were required after fluid challenge and transfusion of packed red blood cells. A broad-spectrum antibiotic was administered. Multiple bacteriological samples, along with a renewed immunological work-up, were inconclusive. A computed tomography (CT) scan was normal. However, the patient presented skin lesions on the breasts (Fig. 1a). These were violaceous, macular, slightly infiltrated plaques. A skin biopsy showed a perivascular lymphocytic infiltrate in the dermis and hypodermis (Fig. 1b). Immunohistology revealed CD20+ (Fig. 1c), CD3–, CD5– and CD10–. The diagnosis was an intravascular lymphoma. The patient died 4 days later with multiple organ failure before any chemotherapy could be initiated.
Fig. 1. (a) Non-infiltrated, purplish plaques on the breast associated with shock, revealing a lymphoma. (b) Histology of a skin biopsy, showing a perivascular lymphocytic infiltrate in the dermis and hypodermis. Near to the tumour, the presence of atypical lymphocytes and red blood cells in the capillaries are visible (arrow). Haematoxylin and eosin (H&E) × 400. The diagnosis is intravascular lymphoma. (c) Immunostaining of a skin biopsy. Antibodies anti-CD20 (× 400). Presence of tumour cells, expressing CD20 (brown), in capillaries (arrow).
Case 2.
A 69-year-old woman was admitted because of shock. During the previous year, the patient had developed 2 haemodynamic collapses with spontaneously favourable outcome. Successive infectious and immunological screenings were negative. A CT scan showed inguinal, iliac and axillary lymphadenopathies. The patient refused a lymphadenopathy biopsy. Three months later, a third febrile shock was complicated by acute respiratory failure, requiring endotracheal intubation and haemodynamic support by vasoactive amines. The haemodynamic monitoring system eliminated cardiogenic shock. The serum lactate dehydrogenase was increased to 524 IU/l. There were infiltrated plaques on the trunk (Fig. 2a). Histological examination showed a lymphomatous proliferation, in the dermis and hypodermis with large cells in a population of small lymphocytes (Fig. 2b), with immunostaining CD3+ (Fig. 2c). Histological analysis of an axillary lymph node biopsy showed a large-cell tumour proliferation, with a nodular and diffuse infiltrate in a microenvironment rich in lymphoid T cells. Clonal analysis performed on the lymph node biopsy showed a majority of monoclonal B population with a dominant monoclonal T contingent. A diagnosis of angio-immunoblastic T-cell lymphoma was made. Combination chemotherapy with rituximab–cyclophosphamide, doxorubicin, vincristine, and prednisone (rituximab-CHOP) was initiated. The patient died 6 months later, despite 2 other lines of chemotherapy.
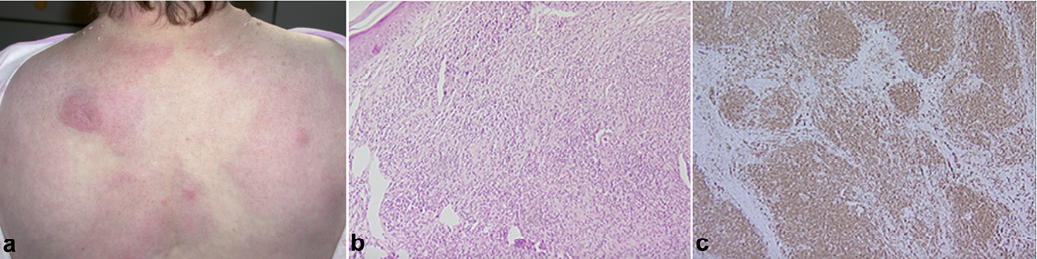
Fig. 2. (a) Infiltrated erythematosus plaques on the back associated with shock, revealing a lymphoma. (b) Histology of a skin biopsy. The infiltrate of lymphoid cells is important in the dermis, without epidermotropism. Haematoxylin and eosin (H&E) × 100. The diagnosis is angio-immunoblastic T cell lymphoma. (c) Immunostaining of a skin biopsy. Antibodies anti-CD3 (× 100). Diffuse expression of CD3 (brown) by lymphoid tumour population.
DISCUSSION
These cases are unusual because of the atypical presentation of shocks and the discretion of the skin lesions, which led to a diagnosis of lymphoma. In the first case, we report an intravascular B-cell lymphoma, and in the second case, an angio-immunoblastic T-cell lymphoma.
Intravascular lymphomas are very rare. They are classified as cutaneous lymphomas in the World Health Organization–European Organisation for Research and Treatment of Cancer (WHO-EORTC) classification (1). They are characterized by multifocal proliferation of lymphocytic cells in the lumina of blood vessels (2). Cutaneous lesions are evocative and reveal a disseminated lymphoma in 75% of cases. Ferreri et al. (2)reported 38 cases of intravascular lymphomas; 39% of whom had skin disorders with heterogeneous lesions. Fewer than 150 cases of intravascular lymphomas have been reported in the literature, with a more or less typical presentation. Indeed, some cases of intravascular lymphomas were reported associated with systemic inflammatory response syndrome (SIRS), as in the observation by Yalamanchili et al. (3) or with acute respiratory failure.
Angio-immunoblastic T-cell lymphoma is a rare type of lymphoma, which affects adults with a median age of 64 years. It is characterized by the association of constitutional symptoms and a tumoural syndrome with hepatosplenomegaly and polyadenopathy. In 40% of cases, angio-immunoblastic T-cell lymphoma is accompanied by non-specific dermatological manifestations (4). A lymph node biopsy shows a partially effaced node structure with a polymorphous infiltrate associated with a proliferation and arborization of high endothelial venules.
The association of SIRS and skin lesions is not rare and has been described recently (5). Shock revealing a lymphoma is rare. Lymphoma can cause SIRS due to a primary release of cytokines by the tumour cells or a secondary release of cytokines after vascular occlusion by the tumour cells (3). There is little data concerning this manifestation. Thus, it is important to request a dermatological consultation in cases of atypical shock.
REFERENCES

