


Gigantic Erythematous Plaques with Violaceous Oedematous Borders: A Quiz
Norma Mechow, Ioana Cosgarea, Edward Ogwang, Ingolf Franke, Harald P. Gollnick and Sven R. Quist*
Department of Dermatology and Venereology, Otto-von-Guericke University, Leipziger Str. 44, DE-39120 Magdeburg, Germany. *E-mail: squist@gmx.de
A 67-year-old female patient presented with multiple erythematous plaques with violaceous oedematous borders. Lesions first appeared on the trunk, then spread to the lower limbs and finally the face within 10 days (Fig. 1). Lesions showed centrifugal expansion and were very itchy. Laboratory tests showed increased eosinophils (0.08%, normal < 0.07%), lactate dehydrogenase (LDH) (4.43 µmol/s/l, normal 2.25–3.35 µmol/s/l), C-reactive protein (CRP) (14.2 mg/l, normal ≤ 5 mg/l), uric acid (389 µmol/l, normal < 340 µmol/l) and carcinoembryonic antigen (CEA) (6.4 ng/ml, normal < 5 ng/ml) as well as total IgE (272 kU/l, normal < 100 kU/l) and eosinophilic cationic protein (31.1 µg/l, normal < 12 µg/l). Tumour markers Cyfra 21-1 and CA 125 II were within normal ranges. There was no history of blistering disease. Any contact with animals or previous insect bites were denied. Due to bronchial asthma with recurring bronchitis the patient was being treated with montelukast ipatropium bromide, salbutamol, femoterol and beclomethasone spray. Medications, unchanged over the last months, included ramipril, amlodipine and torasemide and levothyroxine. Eighteen months previously, a non-small-cell lung cancer at the right lower lobe had been diagnosed and was removed without further radiotherapy or chemotherapy.

Fig. 1. Erythematous plaques on left shoulder (a), lower back (a), right upper leg (a, c) and face (b).
What is your diagnosis? See next page for answer.
doi: 10.2340/00015555-1579
Gigantic Erythematous Plaques with Violaceous Oedematous Borders: Comment
Acta Derm Venereol 2013; 93: XX–XX.
Diagnosis: Wells’ Syndrome
First described by George C. Wells as “recurrent granulomatous dermatitis with eosinophilia” in 1971 (1), and renamed as “eosinophilic cellulitis” and Wells’ syndrome in 1979. The exact pathogenesis is still unknown; however, local hypersensitivity to various triggers, such as arthropod bites and stings, viral and parasitic infections, to drugs and hematologic and non-haematological malignancies have been proposed (2–9). Clinical manifestations include annular reddish plaques with oedema, urticaria or even blisters, vesiculae and hemorrhagic bullae, but also papules, nodules with a recurrent burning or itching sensation, and sometimes with fever and fatigue. The symptoms usually vanish within weeks or months when treated with topical and systemic corticosteroids, but also griseofulvin, antihistaminics and dapsone have been used successfully. Eosinophils play an important role in the typical histology of Wells’ syndrome, showing a dermal infiltrate of eosinophils with an admixture of lymphocytes and histiocytes. Flame figures, collagen fibres with eosinophil granules, are a hallmark of Wells’ syndrome, but can also be associated with other diseases, such as parasitic, viral, fungal or bacterial infections, arthropod bites, mastocytoma, drug reactions, eczema, various malignancies, urticaria, hypereosinophilic syndrome or Churg-Strauss disease (10).
In our patient, computed tomography (CT) scans and chest X-ray 2 months prior to the lesions did not reveal any sign of tumour regrowth. A new CT scan was performed and showed a novel mass formed in the left lower lobe. Subsequent bronchoscopy could not verify or exclude a new malignant process, and this requires further close observation.
Histopathology from biopsies of the elevated erythematous skin borders from the left shoulder (Fig. 2) showed marked dermal oedema, a nodular and diffuse inflammatory infiltrate of the upper and lower dermis associated with connective tissue fibres, which was predominantly eosinophilic, but with few histiocytes lymphocytes. Skin lesions were treated successfully with systemic steroids and topical polidocanol 5% cream. Moreover, treatment with montelukast was paused, but due to severe bronchial obstruction, re-started without exacerbation of Wells’ syndrome.
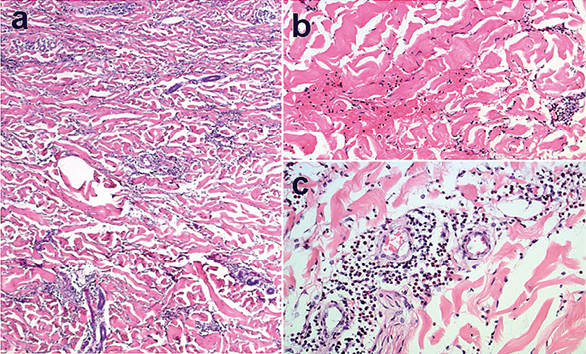
Fig. 2. Histopathology showed (a) a diffuse inflammatory infiltrate of the upper and lower dermis associated with (b) connective tissue fibres, which was predominantly eosinophilic but with (c) a few histiocytes lymphocytes (haematoxylin and eosin; H&E a: × 40, b: ×100, c: × 100).
There have been a few reported cases of Wells’ syndrome associated with non-haematological malignancies, such as one case each of: squamous cell carcinoma of the bronchus (4), adenocarcinoma of the lung (6), adenocarcinoma of the colon (8), and nasopharyngeal carcinoma (7), where skin lesions cleared after successful treatment of the underlying malignancy using either chemotherapy or surgical resection. However, in the case of a 79-year-old woman with squamous cell carcinoma of the bronchus (4), relapse of Wells’ syndrome was noticed when widespread metastases appeared one year after surgery.
This case shows that Wells’ syndrome can present as gigantic erythematous plaques with violaceous oedematous borders, and early sign of malignancy, leading to further clinical investigations and exclusion of a novel malignant progress.
REFERENCES

