


Sara Bassoli, Chiara Ferrari, Stefania Borsari, Francesca Giusti, Cristina Magnoni, Giovanni Pellacani and Stefania Seidenari
Department of Dermatology, University of Modena and Reggio Emilia, Modena, Italy
The dermoscopic descriptor ”negative pigment network” (NPN) has been reported in several types of melanocytic and non-melanocytic lesions, although it has a higher frequency of association with melanoma and Spitz naevus. In a study of 401 consecutive melanomas, excluding facial, acral and mucosal locations, the frequency and variability of NPN were investigated, and the results of NPN correlated with clinical and histopathological data. NPN of any extention was found in 27% of melanomas, most frequently invasive and arising from a naevus on the trunk of young subjects. Seven percent of melanomas in the study population showed presence of NPN in more than half of the lesion area; most of these did not show typical dermoscopic melanoma features. The authors propose a new melanoma subtype, in which extensive NPN should be considered per se as a diagnostic indicator. Key words: multicomponent; negative pigment network; reticular depigmentation; inverse network; dermoscopy; algorithm.
Accepted Dec 17, 2012; Epub ahead of print May 17, 2013
Acta Derm Venereol 2013; 93: XX–XX.
Sara Bassoli, Department of Dermatology, University of Modena and Reggio Emilia, Via del Pozzo 71, IT-41124 Modena, Italy. E-mail: sarabassoli79@gmail.com
Dermoscopy, a method that utilizes pattern analysis and diagnostic algorithms, is currently the preferred diagnostic tool for melanocytic lesions because it has been proven to enhance the accuracy of diagnosis of malignant melanoma (MM) (1–6). Traditional dermoscopic features, however, achieve a maximum sensitivity of only 94%, and are not powerful enough to detect all in situ lesions (2, 7, 8). Since the primary goal of treatment of MM is surgical excision in an early phase, further efforts have been made to improve the diagnostic potential of the dermoscopic examination. Several descriptors characterizing in situ and thin MMs have been proposed by the current study group, such as the dermoscopic island (9), reticular grey-blue regression (10, 11) and peculiar network atypias (12). Moreover, classification into different melanoma subtypes enables the recognition of MM subpopulations that may not be immediately recognizable according to the established main dermoscopic patterns (7, 13).
The dermoscopic parameter “negative pigment network” (NPN), introduced by Menzies et al. in 1996 (14), consists of relatively light areas making up the “cords” of the network, and darker areas filling the holes; it is seen as a negative of the pigmented network and was also named reticular depigmentation (15) or inverse network (13). Its presence has been noticed in MMs, acquired and congenital naevi, Spitz naevi and dermatofibromas (16–18). In a recent review assessing the frequency and characteristics of NPN in a population of melanomas, Spitz naevi and non-melanocytic lesions, Pizzichetta et al. (19) observed that this dermoscopic feature is more frequent than previously described. Under polarized dermoscopy, so called chrysalis structures, have been reported to correspond to changes in the composition and orientation of collagen stroma in melanoma (20). Recently, it has been suggested that chrysalis structures and NPN are manifestations of the same histopathological finding (21).
The current study describes the frequency and variability of NPN in a population of MMs, analysed according to lesion thickness, and clinical and histopathological data.
MATERIALS AND METHODS
The study was approved by the local ethics committee in accordance with ethical standards on human experimentation and with the Declaration of Helsinki. Data were collected according to Protocol Number 1338/C.E.
Dermoscopic images were recorded by means of a digital epiluminescence microscope (FotoFinder, TeachScreen software GmbH, Bad Birnbach, Germany), using 20-fold, 30-fold and a 50-fold magnification. The instrument and the calibration method have been described elsewhere (22). Exclusion criteria included acral, facial and mucosal lesions due to their site-specific dermoscopic aspects. A total of 401 consecutive MMs, including 117 in situ melanomas (MIS) and 284 invasive melanomas (MInv), 183 with a Breslow thickness ≤1 mm (thin MInv) and 101 with a thickness > 1 mm (thick MInv), excised from 2003 to 2009 at a single dermatological department, were selected for retrospective analysis. Images of MIS and MInv were contemporarily reviewed by 3 expert dermoscopists (SS, SB, and CF) to define the main dermoscopic pattern and the presence/absence of NPN in the lesion. According to Pizzichetta et al. (19), NPN was defined as a negative of the pigment network with relatively light areas making up the “cords”, having the same thickness as expected for a pigment network, and brown areas constituting the “holes”. When disagreements occurred, the observers discussed the case in order to reach a common opinion.
Demographic and histological data, such as the gender and age of the patient, Breslow thickness, location according to anatomical site and previous naevus, were also considered. The evaluation of NPN distribution (central, peripheral, both) and lesion surface involvement (< 20%, 20–50%, > 50%) was also performed. Moreover, NPN was defined as homogeneous when the width of the “cords” was uniform, and heterogeneous when an increased range of width of the ridges, surrounding globules varying in both shape and size, was noticed (19).
NPN-MMs were also classified according to their main dermoscopic pattern into the following groups: reticular, globular, homogeneous (with structureless pigmentation), reticular–globular, reticular–homogeneous, globular–homogeneous and multicomponent (when reticular, globular, and homogeneous areas were all found within the same lesion) (12, 13). Other patterns observed in our study were the starburst pattern (attributed to lesions with a radial aspect), the reticular grey-blue regression pattern (coarse blue-grey net, with thick grey-blue lines and large holes, corresponding to white or pink regression areas) (10, 11) and the aspecific pattern, when none of the previous main patterns could be identified. When RD covered more than 50% of the lesion area, the main dermoscopic pattern was classified as RD.
The 7-point score (23) and the ABCD TDS (24) were computed for all 401 MMs.
Statistical analysis
Statistical evaluation was carried out using the SPSS statistical package (release 12.0.0, 2003; SPSS Inc., Chicago, IL, USA). The study sample was primarily subdivided into 2 groups; corresponding to the histopathological diagnosis of MIS and MInv. Differences between MIS and MInv and between thin MInv and thick MInv were assessed by means of the χ2 test of independence (Fisher’s exact test was applied if any expected cell value in the 2 × 2 table was < 5). Student’s t-test was performed to compare mean values. A p < 0.05 was considered significant.
RESULTS
A total of 401 MMs were analysed. Clinical aspects (sex, age and anatomical site) and histological features (thickness and presence of a pre-existing naevus) are described in Table I. MMs belonged to 210 men and 191 women; approximately 50% were located on the trunk, 20% on the upper limbs and 30% on the lower limbs. The mean lesion thickness was 0.98 ± 1.76 mm. In all, 27% of MMs had arisen from a naevus.
Table I. Clinical and histological features of 401 melanomas (MMs) with or without negative pigment network (NPN) at dermoscopy. Bold figures and * indicate statistically significant (p< 0.05) differences among lesions of different thickness, with or without NPN
|
Total MMs n = 401 |
MMs with NPN |
MMs without NPN |
|||||||
|
Total n = 107 |
MIS n = 20 |
MInv ≤ 1 mm n = 51 |
MInv > 1 mm n = 36 |
Total n = 294 |
MIS n = 97 |
MInv ≤ 1 mm n = 132 |
MInv >1 mm n = 65 |
||
|
Men, % |
52.4 |
58.9 |
70.0 |
60.8 |
50.0 |
50.0 |
47.4 |
54.5 |
44.6 |
|
Age, years, mean ± SD |
56.4 ± 16.4 |
53 ± 15.5 |
53.4 ± 9.6 |
54 ± 17. 9 |
50.9 ± 14.1* |
57.7 ± 16.7 |
56.8 ± 17.3 |
55.9 ± 15.4 |
62.8 ± 16.6* |
|
Trunk, % |
49.9 |
53.3 |
45.0 |
58.8 |
50.0 |
48.6 |
51.5 |
46.2 |
49.2 |
|
Upper limbs, % |
21.7 |
26.2 |
30.0 |
27.5 |
22.2 |
20.1 |
18.6 |
21.2 |
20.0 |
|
Lower limbs, % |
28.4 |
20.6* |
25.0 |
13.7* |
27.8 |
31.3* |
29.9 |
32.6* |
30.8 |
|
Thickness, mm, mean ± SD |
0.98 ± 1.76 |
1.07 ± 1.75 |
0.0 |
0.6 ± 0.21 |
2.33 ± 2.66 |
0.96 ± 1.76 |
0.0 |
0.53 ± 0.25 |
3.24 ± 2.65 |
|
Ex naevo, % |
26.9 |
37.4* |
40.0 |
29.4 |
33.3 |
23.1* |
28.9 |
20.5 |
20.0 |
MIS: in situ MMs; MInv: invasive MMs; SD: standard deviation.
A total of 107 (26.7%) MM lesions were identified with NPN. Some examples of melanomas with NPN are illustrated in Fig. 1. NPN was present in 20 out of 117 MIS (17.1%) and in 87 out of 284 MInv (30.6%). Patients with MMs showing NPN were younger with respect to the population lacking NPN, considering both the whole population and the 3 thickness subgroups; the difference became statistically significant when comparing patients with thick MInv (50.9 and 62.8 years, respectively).
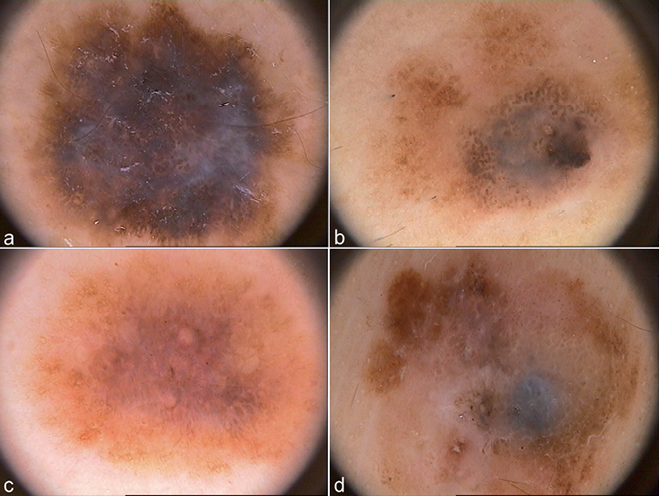
Fig. 1. Dermoscopy (× 20 magnification). Melanomas characterized by the presence of some degree of reticular depigmentation. (a) Female (F), 88 years old, 0.58 mm, upper limbs: negative pigment network (NPN) is centrally and peripherally distributed, heterogeneous and multifocal; (b) Male (M), 40 years old, 0.89 mm, upper limbs): NPN is centrally and peripherally distributed and shows a homogeneous aspect; (c) F, 43 years old, 0.63 mm, trunk: NPN is located in the centre of the lesion, heterogeneous and multifocal; (d) M, 28 years old, 1.15 mm, trunk: NPN is centrally and peripherally distributed, heterogeneous and multifocal.
A higher percentage of MMs without NPN was located on the lower limbs with respect to those with NPN (p = 0.048). In all, 37% of MMs with NPN had arisen on a naevus, compared with 23% of those without NPN (p = 0.007).
Among 107 MMs with NPN, 20 (18.7%) were MIS, 51 (47.6%) were thin MInv and 36 (33.6%) thick MInv. MMs without NPN included 97 MIS (33%), 132 thin MInv (44.9%) and 65 thick ones (22.1%). Thus, MIS were significantly more frequent among lesions without NPN (33.0% vs 18.7%; p = 0.008), whereas MMs thicker than 1 mm more commonly showed NPN (33.6% vs 22.1%; p = 0.027). By contrast, the mean thickness of thick MInv without NPN was higher than that of thick MInv with NPN (3.24 ± 2.65 mm vs. 2.33 ± 2.66mm), although not significantly so.
Features of NPN observed in 107 MMs are described in Table II. A central distribution was observed in 7.4% of cases, a peripheral distribution in 39.2%, while both a central and peripheral presence of NPN was seen in 53.3% of cases. In 41.1% of MMs, NPN covered an area < 20%, in 31.8% an area between 20% and 50%, and in 27.1% an area of > 50%. Homogeneity of NPN was observed in 37.4% of the lesions, the rest (62.6%) were characterized by an increased range of width of the ridges, surrounding pigmented polygonal areas variable in size and shape (i.e. heterogenous).
Table II. Features of negative pigment network present in 107 melanomas (MMs) comprising in situ MMs (MIS) and invasive MMs (MInv) (statistically significant marked in bold and *)
|
Total MMs n = 107 % |
MIS n = 20 % |
Total MInv n = 87 % |
MInv ≤ 1 mm n = 51 % |
MInv > 1 mm n = 36 % |
|
|
Central distribution |
7.4 |
15.0 |
5.7 |
7.8 |
2.8 |
|
Peripheral distribution |
39.2 |
25.0 |
42.5 |
35.3 |
52.8 |
|
Central + peripheral |
53.3 |
60.0 |
51.7 |
56.9 |
44.4 |
|
Extension < 20% |
41.1 |
70.0* |
37.9* |
33.3 |
44.4 |
|
Extension 20–50% |
31.8 |
0.0* |
35.6* |
41.2 |
27.8 |
|
Extension > 50% |
27.1 |
30.0 |
26.4 |
25.5 |
27.8 |
|
Homogeneous pattern |
37.4 |
65.0* |
31.0* |
33.3 |
27.8 |
|
Heterogeneous pattern |
62.6 |
35.0* |
69.0* |
66.7 |
72.2 |
|
Multifocal pattern |
66.4 |
60.0 |
67.8 |
64.7 |
72.2 |
In 66.4% of cases, disconnected multifocal areas of NPN were observed.
The distribution and extension of NPN in the 107 NPN-MMs were also evaluated according to MM thickness. No significant differences were observed in the distribution of NPN among MIS and MInv. In MIS the lesion area covered by NPN was smaller compared with MInv: in 70% of MIS an area of involvement of less than 20% was observed, whereas 35.6% of MInv showed NPN in 20–50% of the lesion area. A homogeneous aspect of NPN was significantly more often seen in MIS (65% vs. 31.0%, p = 0.01), while a heterogeneous one was more frequent in MInv (69% vs. 35%, p = 0.01). Among MInv, the subgroups of thin and thick MInv did not vary significantly in terms of extension and distribution of NPN.
Table III describes the main dermoscopic pattern of all 107 NPN-MMs. A multicomponent pattern was observed in 43.9%. NPN as the main dermoscopic pattern was seen in 27.1% (Fig. 2). Other main patterns were seen in 29% of cases.
Table III. Main dermoscopic pattern in 107 melanomas (MMs) with negative pigment network (NPN), comprising invasive melanomas (MInv) (n = 87) and in situ melanomas (MIS) (n = 20)
|
Main pattern |
Total MMs % |
MIS % |
MInv % |
|
Multicomponent |
43.9 |
35.0 |
46.0 |
|
NPN |
27.1 |
30.0 |
26.4 |
|
Aspecific/others |
7.8 |
– |
9.2 |
|
SP |
5.6 |
5.0 |
5.7 |
|
Reticular SP |
5.6 |
15.0 |
3.4 |
|
Reticular grey-blue regression |
5.6 |
15.0 |
3.4 |
|
Globular SP |
4.7 |
– |
5.7 |
SP: structureless pigmentation.
Fig. 2. Dermoscopy (× 20 magnification) of melanomas characterized by negative pigment network (NPN) as a main pattern. In these melanomas, NPN covers more than 50% of the lesion area and it represents the main characteristic of the lesions, not showing other typical dermoscopic features highly suggestive of malignancy. (a) Male (M), 47 years old, 0.4 mm, trunk; (b) Female (F), 54 years old, 0.6 mm, trunk; (c) F, 72 years, 0.39 mm, trunk (× 30 magnification); (d) F, 41 years old, 0.22 mm, lower limbs; (e) M, 37 years old, 0.29 mm, upper limbs; (f) M, 55 years old, 1.07 mm, trunk.
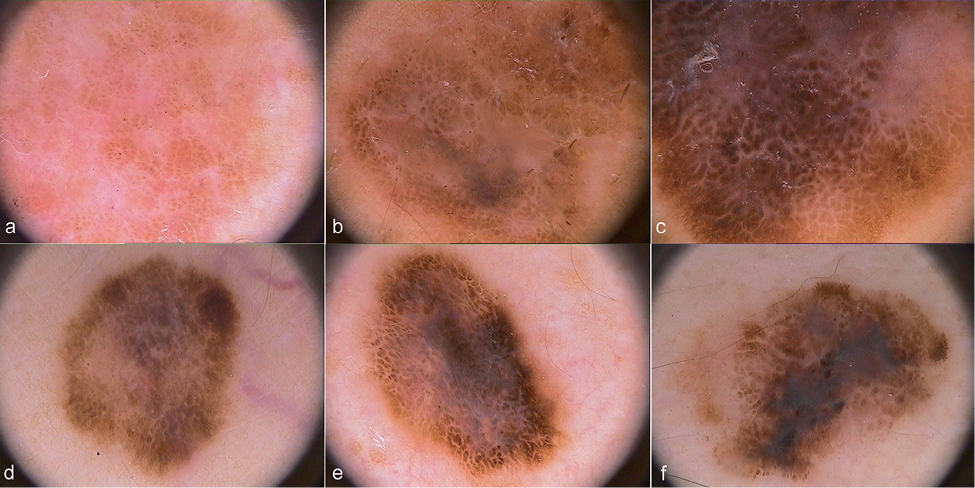
Table IV describes the clinical and histological features of 29 MMs with NPN as main pattern compared with the 372 MMs with other main patterns. The mean age of the patients was lower in NPN pattern MMs compared with non-NPN pattern MMs (46.5 ± 15.3 vs. 56.8 ± 16.2 years, p < 0.05); a significant difference was also observed when the population of NPN pattern MInv was compared with non-NPN pattern MInv, particularly in the thick MInv subgroup (41.9 ± 13.2 vs. 60.1 ± 16.3 years, p = 0.000). No statistically significant differences regarding gender, anatomical location, mean thickness and presence of a pre-existing naevus were observed between the two main pattern groups. However, in the thick MInv subgroup, mean lesion thickness of NPN pattern MMs was lower (1.63 ± 1.05 mm), compared with non-NPN pattern MMs (3.11 ± 2.76). Moreover, a higher frequency of ex naevo onset in NPN pattern MMs was observed with respect to non-NPN pattern MMs (40.7% vs. 28.5%). In particular, NPN pattern MIS arose from a naevus in 66.7% of cases, compared with 32.4% in non-NPN pattern MIS.
Table IV. Main clinical and histological features of melanomas (MMs) with negative pigment network (NPN) as main pattern (covering >50% of the surface) compared with MMs with a different main dermoscopic pattern (statistically significant marked in bold and *)
|
MMs with NPN as main pattern |
MMs with a different main dermoscopic pattern |
||||||||||
|
Total n = 29 |
MIS n = 6 |
Total MInv n = 23 |
MInv ≤ 1 n = 13 |
MInv > 1 n = 10 |
Total n = 372 |
MIS n = 111 |
Total MInv n = 261 |
MInv ≤ 1 n = 170 |
MInv > 1 n = 91 |
||
|
Men, % |
66.7 |
66.7 |
69.6 |
69.2 |
70.0 |
51.4 |
49.5 |
51.0 |
53.5 |
46.2 |
|
|
Age, years, mean ± SD |
46.5 ± 15.3* |
50.3 ± 12.0 |
45.4 ± 16.2* |
48 ± 18.2 |
41.9 ± 13.2* |
|
56.8 ± 16.2* |
56.4 ± 16.5 |
57.1 ± 16.1* |
55.5 ± 15.8 |
60.1 ± 16.4* |
|
Trunk, % |
55.6 |
33.3 |
61.9 |
53.8 |
70 |
48.7 |
51.4 |
47.5 |
47.64 |
47.3 |
|
|
Upper limbs, % |
18.5 |
16.7 |
19.0 |
30.8 |
10 |
21.2 |
19.8 |
21.8 |
21.76 |
22.0 |
|
|
Lower limbs, % |
33.3 |
50 |
28.6 |
23.1 |
30 |
27.7 |
27.9 |
27.6 |
27.64 |
27.5 |
|
|
Thickness, mean ± SD |
0.80 ± 0.89 |
0.0 |
0.88 ± 0.47 |
0.54 ± 0.24 |
1.63 ± 1.05 |
1.00 ± 1.82 |
0.0 |
1.43 ± 2.04 |
0.54 ± 0.22 |
3.11 ± 2.76 |
|
|
Ex naevo, % |
40.7 |
66.7 |
33.3 |
46.2 |
20.0 |
28.5 |
32.4 |
26.8 |
32.94 |
15.4 |
|
|
7-point score, mean ± SD |
4.48 ± 2.29* |
2.16 ± 1.60* |
5.14 ± 2.03 |
4.16 ± 1.26* |
6.44 ± 2.18 |
|
5.38 ± 2.18* |
4.02 ± 2.07* |
5.97 ± 1.96* |
5.75 ± 1.97* |
6.38 ± 1.88 |
|
ABCD score, mean ± SD |
5.7 ± 1.2 |
4.78 ± 1.23 |
5.98 ± 1.11 |
5.86 ± 0.99 |
6.14 ± 1.30 |
6.05 ± 1.19 |
5.67 ± 1.11 |
6.21 ± 1.19 |
6.2 ± 1.04 |
6.24 ± 1.44 |
|
MIS: in situ MMs; MInv: invasive MMs; SD: standard deviation.
Finally, 7-point scores were significantly lower in NPN pattern MMs with respect to non-NPN pattern MMs (see Table IV). ABCD scores were also lower in non-NPN pattern MMs, although this difference was not significant (5.7 ± 1.23 vs. 6.05 ± 1.19). Fig. 2 shows 6 examples of NPN pattern MMs.
DISCUSSION
Huge efforts have been made to define new descriptors, enabling a refinement of the diagnostic procedure in pigmented skin lesions (7–9, 25, 26).
NPN has been described as a dermoscopic feature related to several cutaneous entities, such as dermatofibromas (19), Spitz naevi (27), dysplastic naevi and melanoma, mainly in its invasive subtype (14). Although in a recent study by Argenziano et al. (26), NPN was not considered predictive for the final diagnosis of benign or malignant lesion and Menzies et al. (14) and Skvara et al. (7) reported a low sensitivity of NPN in MM diagnosis, the importance of NPN as a diagnostic clue for MM has been affirmed by others (19, 28).
From a histopathological point of view, NPN represents elongated hypomelanotic rete ridges and large nests of pigmented cells located at the dermal papillae (19). On the other hand, Botella-Estrada et al. (21) state that in Spitz naevi NPN is characterized by the same histopathological substrate as the chrysalis structure, featured by an extensive fibrosis and dermal remodelling causing the bi-refractivity under polarized dermoscopy. Pizzichetta et al. (19) recently reported an extensive analysis, which aimed at characterizing NPN and differentiating its dermoscopic aspects in melanoma and control lesions. The study included dermatofibromas, benign naevi and Spitz/Reed naevi. NPN was defined as a negative mesh consisting of relatively light areas making up the “cords” of the network, with darker areas filling the holes. The lighter grid lines tend to be serpiginous, and they surround the irregularly shaped pigmented structures that resemble elongated and curvilinear globules (15). Two types of false NPN must be distinguished: the first is present in globular or cobblestone naevi and shows a greater range of hypopigmented cord width and/or much larger “holes” filled by large or cobblestone like globules. The second type, corresponding to a white network or chrysalis structures seen in dermatofibroma, can be differentiated from true NPN based on a greater width of short, bright-white, linear lines, which are often orthogonally oriented (19).
Pizzichetta’s multicentre study included 205 MMs and 461 benign lesions and revealed a higher frequency of NPN in MMs compared with benign lesions, particularly when irregularly distributed and located on the periphery. Furthermore, NPN was identified as being more common in MInv than in MIS (36.8 % vs. 28.0%), in line with the data presented in this study (30.6% vs. 17.1%). The multicomponent dermoscopic pattern was found to be significantly correlated with MM diagnosis; the overall specificity for the presence of NPN was high (80.4%), along with a low sensitivity (34.6%) (19).
The present study represents the most extensive monocentric investigation on a population of 401 MMs. Our aim was not to calculate specificity figures of this dermoscopic feature, which were extensively assessed in the paper by Pizzichetta et al. (19), but to evaluate its sensitivity and to characterize NPN in terms of both features and extension, in relation to dermoscopic, histological and clinical aspects. Among the study population described in this paper, 26.7% of MMs showed some degree of NPN, and 7.23% showed NPN involving more than 50% of the lesion area.
According to the presence and extension of NPN, two different subpopulations of NPN-MMs (MMs showing any extension of NPN and MMs with NPN as the main pattern) were identified and were compared with MMs where NPN was not observable. Also in this study, NPN was found to be more frequently associated with MInv compared with MIS, especially when considering thick MInv.
In the current study population, MMs with any extension of NPN were more frequently invasive, more often arising from a naevus and located on the trunk of younger subjects. In most cases, NPN covered an area smaller than 20% of the surface. Contrary to Pizzichetta’s observations of a prevalent peripheral location, NPN was observed both centrally and peripherally, with a multifocal distribution. In MIS, NPN extension was circumscribed to less than 20% of the lesion area in 70% of cases, whereas MInv were characterized by a 20–50% area involvement in 35% of cases.
The concept of main pattern has been introduced in dermoscopy to describe with a single term the main characteristics of a lesion. This enables a classification of benign and malignant lesions to be used for clinical correlations, such as follow-up studies, etc.
Two main pattern populations prevailed among NPN-MMs. Forty-four percent of NPN-MMs showed the contemporary presence of globules, network and structureless pigmentation and were classified as multicomponent MMs. The multicomponent pattern was already shown to frequently be associated with MM diagnosis (28), especially in the presence of a naevus-associated MM (12). In a study performed on 114 MIS, an associated naevus was found in 67% of MIS with dermoscopic island, in 48% of lesions with a multicomponent pattern, in 43% of MIS with inverse network. Those dermoscopic features were reported to represent frequentinitial patterns of a MIS arising on a naevus were reported to represent frequent initial patterns of a MIS arising on a naevus (12). Thus, based on the data presented in this study, NPN on the background of a multicomponent lesion could represent the expression of fibrotic regression as a reaction of a benign lesion against the malignant evolution.
When NPN covers more than 50% of the area, the lesion acquires a typical uniform and symmetrical aspect, which does not match traditional dermoscopic MM criteria. This data confirm that NPN-MM may mimick a benign nevus or a Spitz naevus. Paradoxically, in favour of a diagnosis of benignity stands also the clinical aspect referring to the age of the patients, since NPN-MMs arise in younger patients. Other characteristics of NPN-MMs were a higher prevalence in male subjects and the ex naevo appearance of the malignancy (41% of NPN-MMs arose on a naevus, 13% more than MMs with a different main pattern).
To the best of our knowledge, this is the first time that MMs with extensive NPN have been described and classified according to NPN as the main lesion pattern. In this study, 7% of the population of 401 MMs were classified accordingly, representing a considerable portion of MMs encountered in clinical practice.
The description of MM patterns is important both for the recognition of new subgroups and early diagnosis and for the identification of MM subtypes that may be correlated with different biological behaviours (29). New evidence suggests that MM comprises a family of tumours that vary in growth activity (30, 31). Rapidly growing (32) and slow-growing (8, 32) MMs show different dermoscopic characteristics, which can thus provide clues as to the biological potential of these lesions. Several intermediate types of MM may exist, varying in their tendency to grow and metastasize, possibly corresponding to different dermoscopic aspects. This study introduces a new dermoscopic subtype of MM, the NPN pattern MM, which is commonly associated with young male subjects and has an ex naevo origin.
The authors declare no conflicts of interest.
REFERENCES

