


1Department of Dermatology and Venereology, 2Institute of Virology, University Medical Centre, Hauptstraße 7, DE-79104 Freiburg, and 3Bundeswehr Institute of Microbiology, Munich, Germany. E-mail: barbara.miernik@uniklinik-freiburg.de
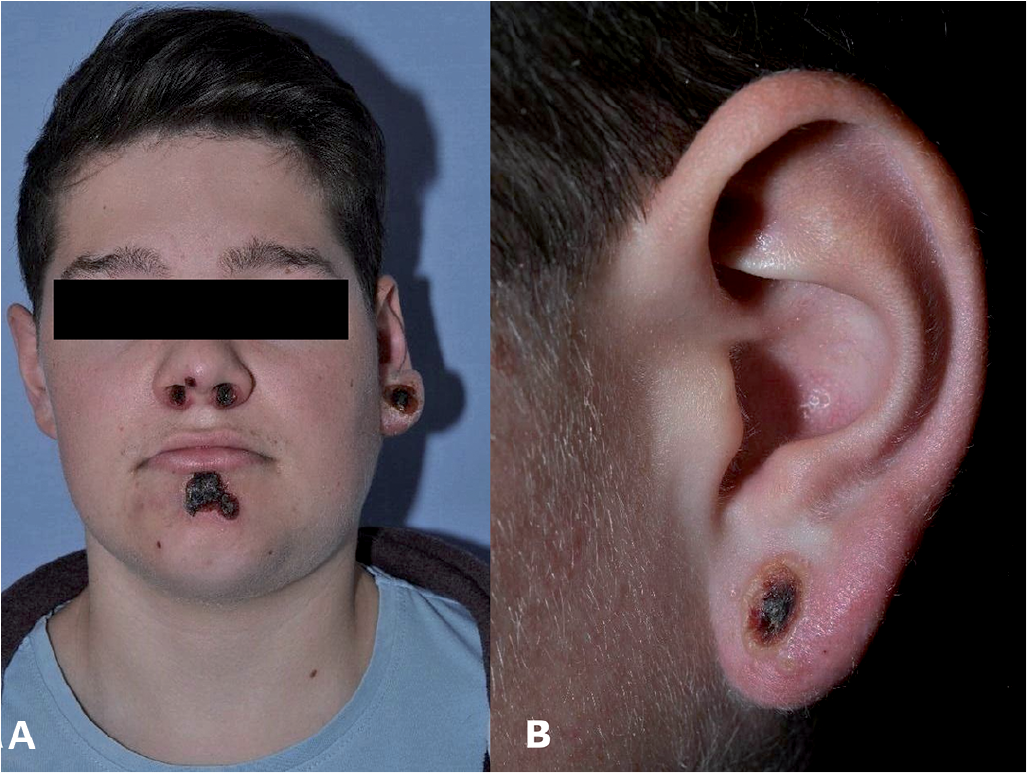
A 16-year-old boy presented with multilocular necrotizing eschar-like facial ulceration, which had first manifested as a solitary red papule, gradually transforming into a blister. Similar lesions had subsequently appeared on his chin and nostrils. A trial of antibiotics (amoxicillin, clavulanic acid, cefuroxime) combined with antiseptic local treatment was administered with no improvement. On examination, the patient showed painless, umbilicated lesions with central necrosis (on the left earlobe, chin, and nostrils) and left-sided painful cervical and submandibular lymphadenopathy (Fig. 1). He reported general, flu-like malaise and a single episode of fever. He had no atopic predisposition and had received all intended childhood vaccinations. The patient lived on the countryside with 2 cats, which were reported to be healthy. Serology work-up was normal (no herpes simplex virus or tuberculosis. Bartonella henselae IgG titre was elevated). A biopsy revealed necrosis with eosinophilic intracytoplasmic inclusion bodies. Computed tomography of the head excluded cartilage involvement. Microbiological examination showed massive colonization of Staphylococcus aureus.
Fig. 1. (A) Multilocular facial ulceration on the left ear lobe, chin and both nostrils, covered with a black eschar and accompanied by extensive left-sided lymphadenopathy. (B) Left ear lobe with umbilicated necrosis (on day of first presentation). The patient has granted permission to publish these photographs.
What is your diagnosis?
The histological presence of eosinophilic intracytoplasmic inclusion bodies is pathognomonic for an infection with orthopoxvirus (OPV) (1, 2) (Fig. 2).
Fig. 2. Biopsy of the chin (haematoxylin and eosin staining). (A) Extensive intercellular and intracellular oedema with necrosis of epidermis (100× magnification) and (B) eosinophilic intracytoplasmic inclusion bodies in necrotic keratinocytes (400× magnification).
The cytopathogenic agent was isolated using cell cultures. Virus culture and biopsy samples were both positive for an OPV by applying 2 polymerase chain reaction (PCR) assays. Amplicon sequencing confirmed a CPXV infection. OPV-specific antibodies (1:80) were found in a plaque-reduction assay and by indirect immunofluorescence. Although the patient’s cat had no visible cutaneous lesions, and a mouth swab from the cat was PCR-negative, detection of OPV antibodies implies that the cat had transmitted the virus. Superinfection with Staphylococcus aureus caused an infra-auricular lymphatic abscess, which was treated surgically and with antibiotics. The boy’s lesions healed approximately 8 weeks later with hypertrophic scarring.
CPXV belong to the Poxviridae family, genus Orthopoxvirus, which also includes variola (the causative agent of smallpox), vaccinia and monkeypox virus. Human CPXV infections have been described only in Europe and Western Asia. Rodents, especially voles and wood mice, are considered the primary reservoir (3). Transmission to humans occurs through skin lesions by infected domestic animals (cats, rats, circus animals). The incidence of CPXV infection, e.g. among domestic cats, is high; it is estimated at 2% in Germany (4), 4% in Austria (5), 5% in Denmark (6) and 10.1% in Norway (7). Peak contamination times are between August and October, correlating with large populations and high activities of rodents (1, 8). Lesions are found in correspondence with the area of intense contact with animals, predominantly the arms and shoulders and, rarely, the face. So far, 1 case of infection via the mucosa, resulting in facial cellulitis, has been reported (9). The majority of cases are characterized by a solitary lesion. Multiple efflorescences, as seen in our case, are very rare and occur either via multiple primary inoculation sites, autoinoculation or lymphatic spread with a sporotricoid distribution (10). Transmission by autoinoculation results mainly in ocular lesions, but is rarely documented on the skin, as occurred in our case. Person to person transmission has not been reported.
The clinical hallmark of a CPXV infection is a red papule, evolving through a vesicle, and a haemorrhagic stage into a necrotic ulcer, often accompanied by lymphadenopathy, fever and general malaise (9, 11). PCR, from a vesicle fluid or lesional eschar, is currently considered the method of choice to diagnose a CPVX infection. Electron microscopy also allows rapid diagnosis, but is limited by its availability and cannot distinguish different OPV species (11, 12).
In most cases, CPXV infections are a self-limiting disease, healing spontaneously within 6–12 weeks by scarring. Therefore, a substantial number of human CPXV infections might go undetected or be misdiagnosed. However, generalized and even lethal CPXV courses have been described in immunocompromised patients or individuals with atopic or Darier’s disease (1, 13). No specific treatment is currently available. Supportively, local antiseptics, non-steroidal anti-rheumatic drugs, surgical debridement and antibiotics for preventing superinfection may be considered. Cidofovir, an inhibitor of viral DNA-polymerase approved for treatment of cytomegalovirus-associated retinitis in patients with HIV, has been proven efficient against OPV infections; however, its use is limited by nephrotoxic side-effects (2). Today, the oral drug tecovirimat (previously known as ST-246) might be used as a promising post-exposure therapeutic treatment for OPV disease. Small pox vaccination might have provided cross-immunity against CPXV in the past (13). The abandonment of mandatory vaccination programmes in the late 1970s, and the raising of clinical awareness, might have led to an increasing number of CPXV infections being diagnosed (14).
The primary differential diagnosis in a case of unclear necrotizing lesions should include severe bacterial dermatitis, necrotizing herpes simplex virus (HSV) infection, atypical cutaneous mycobacteriosis (TBC), lymphomatoid papulosis and cutaneous anthrax (1, 8). If the patient has a history of animal contact, diagnosis of cat-scratch disease and CPXV infection should be also considered.
The authors would like to thank Robert Fux (Department of Veterinary Sciences, Ludwig-Maximilians-University of Munich) for providing technical assistance and analysing veterinary samples. The article processing charge was funded by the German Research Foundation (DFG) and the Albert Ludwigs University Freiburg in the funding programme Open Access Publishing.


 Click to show fullsize
Click to show fullsize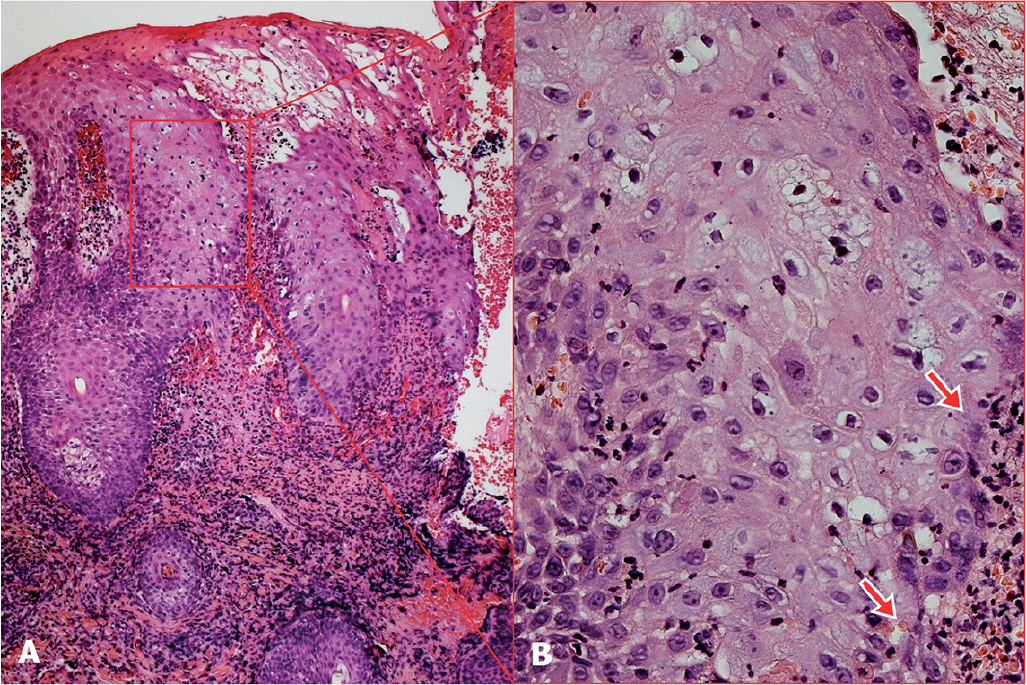 Click to show fullsize
Click to show fullsize