


Department of Skin Oncology/Dermatology, Saitama Medical University International Medical Center, 1397-1 Yamane, Hidaka, Saitama 350-1298 Japan. E-mail: yurilv_vlpqlu_ul@yahoo.co.jp
Accepted Jul 4, 2016; Epub ahead of print Jul 7, 2016
Intravascular papillary endothelial hyperplasia (IPEH) accounts for approximately 2–4% of all vascular tumours of the skin and soft tissue (1). It was originally considered a neoplasm, but is currently recognized as an unusual non-neoplastic, reactive endothelial proliferation associated with an organizing thrombus (2). Histologically, IPEH is characterized by the papillary proliferation of endothelial cells within a vascular lumen (3). Hashimoto et al. (1) have classified IPEH into 3 types: (i) a pure form that occurs within a dilated vascular space, (ii) a mixed form that appears as a focal change, but within another vascular lesion, and (iii) a third form that does not belong to either of the previous types. Although IPEH commonly forms in the soft tissue and usually presents as a solitary lesion, we report here an unusual case of IPEH formed both on the superficial skin and on an intermuscular area on the back.
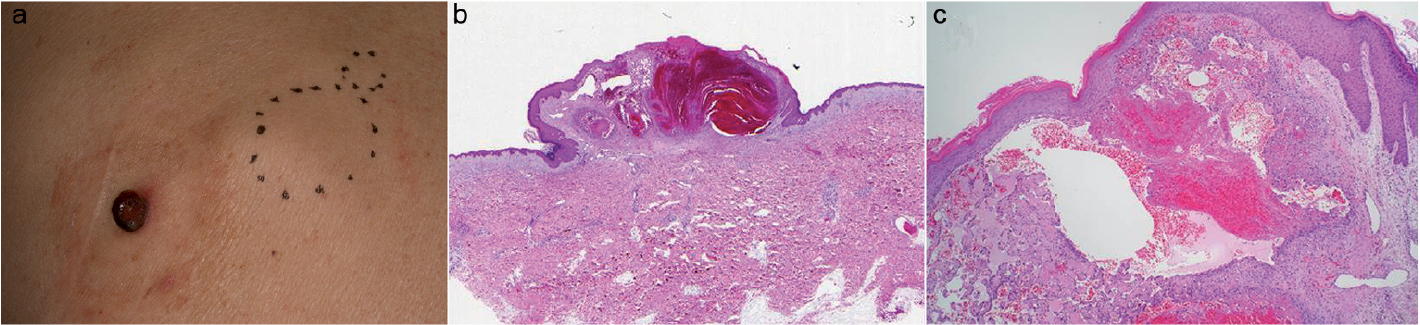
A 70-year-old man presented with a skin nodule and a subcutaneous mass on the left side of his back that had developed and increased in size 2 months earlier. The patient had had Parkinson’s disease for 7 years, managed with regular levodopa. Physical examination revealed a 1.3-cm red-coloured dome-shaped nodule and a 4-cm long elastic soft, well-mobile, restiform subcutaneous tumour (Fig. 1a). The patient had no swollen axillary nodes. These clinical findings were suggestive of amelanotic melanoma that may have metastasized to the subcutaneous tissue. However, an excisional biopsy specimen of skin nodule revealed dilated vascular spaces with haematoma, lined by one or two layers of endothelial cells that form papillary structures (Fig. 1b, c), which led us to speculate that these tumours represent IPEH. Furthermore, ultrasonography revealed another well-defined, restiform, low-echoic, heterogeneous mass of 4.5×3.5cm, just beneath the trapezius muscle. Subsequently, we performed local excision of the intermuscular tumour under general anaesthesia. After confirming the trapezius muscle, it was retracted cranially, exposing the dark-red coloured tumour, which was well encapsulated (Fig. 2a). The tumour was safely enucleated. Histological analysis revealed that the lesion consisted of a segment of dilated blood vessel and thrombus, along with papillary structures lined by a single layer of endothelial cells within the vascular space. These endothelial cells did not invade into the adjacent tissue, and showed few mitotic figures, but no cellular atypia or necrosis (Fig. 2b). On the basis of these clinical, radiological and histological findings, the lesions were diagnosed as IPEHs.
Fig. 1. (a) The clinical appearance shows a red-coloured dome-shaped tumour and 2 subcutaneous tumours on the back (dotted circles). (b) Gross pathology showing dome-shaped nodule, dilated blood vessel and thrombus formation. (c) Vascular spaces lined by one or two layers of endothelial cells that form papillary structures. Haematoxylin and eosin stain, original magnification (b: × 1, c: × 40).
Fig. 2. (a) The mass removed from under the trapezius muscle was dark red in colour and well encapsulated. (b) Papillary structures lined by endothelial cells within vascular space, composed of a single layer of endothelial cells without atypia, and few mitotic figures. Haematoxylin and eosin stain, original magnification × 200).
In 1923, Masson described, for the first time, an atypical papillary endothelial proliferation similar to angiosarcoma. Such regions were designated as “intravascular papillary endothelial hyperplasia” by Clearkin & Enzinger in 1976 (4). The most common clinical symptom is a slowly-growing nodule, with bluish or reddish discoloration of the overlying skin (2, 5). IPEH may occur in any blood vessel of the body, but is more prevalent on the fingers, head, and the neck region. Most IPEHs are solitary and are located in the subcutis, measuring less than 2 cm in diameter (1, 3). However, in the case reported here, IPEHs occurred both on the superficial skin and in the intermuscular area, which initially led to the incorrect diagnosis of amelanotic melanoma and its subcutaneous metastases. Co-existence of multiple IPEHs occurring both on the superficial skin and in the soft tissue is rare, with only one case, reported by Higashi et al. in 2009 (3). This report described a 75-year-old man, who presented with multiple recurrent black-coloured skin papules in association with a radiolucent lesion on his tibia (3).
Although there are several reports regarding multiple IPEHs, its pathogenesis is still unclear. However, formation of thrombosis due to systemic disease or a drug may be correlated with its onset (3, 6, 7). The case reported by Higashi et al. (3), as described above, had a history of hepatitis C and subsequent hepatoma. In another study, Petry et al. (6) described a 47-year-old man with multiple IPEHs in the spinal column, who had a history of Wegener granulomatosis. The authors suggested the possibility of underlying thrombosis of the basivertebral venous plexus (6). Gordon et al. (7) reported a 62-year-old woman with multiple IPEHs on the forearms, receiving oral prednisone therapy for advanced sarcoidosis.
In addition, previous reports have shown that multiple IPEHs often occurred on the fingers or arms, suggestive of the sites that vulnerable to traumas. Sung et al. (8) reported that, in their study of 19 patients with finger IPEHs, one patient had 2 lesions extending into the interdigital web space. In a similar study, Stewart & Smoller (9) reported an 80-year-old woman with multiple IPEHs distributed on the upper arms in addition to the face and neck. Likewise, Gordon et al. (7) reported a case of a 62-year-old woman with 2 nodules of IPEHs on the forearm. Another basic research study suggests that pathogenesis of IPEH involves an autocrine loop of endothelial basic fibroblast growth factor (bFGF) secretion, which stimulates proliferation of endothelial cells (10). Thus, it is possible that the onset of IPEH could be triggered by secretion of bFGF from macrophages at the site of trauma (11).
On the basis of these previous reports, we speculate that the patient’s involuntary movement due to Parkinson’s disease may have caused frequent trauma to his back, leading to the development of multiple IPEHs nearby.
This work was partially supported by the National Cancer Center Research and Development Fund (26-A-4).


 Click to show fullsize
Click to show fullsize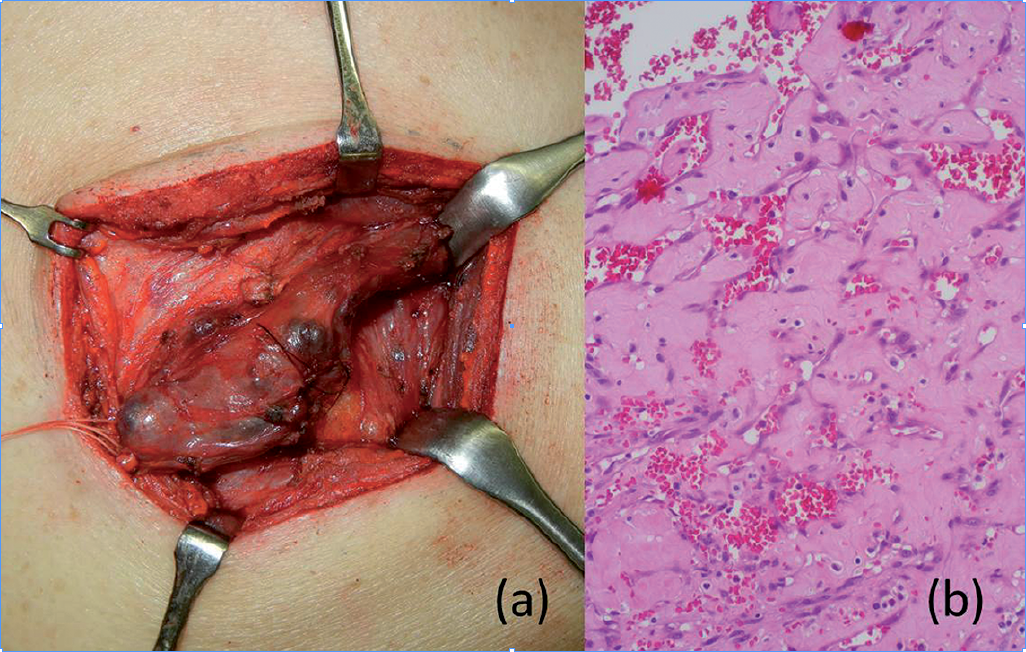 Click to show fullsize
Click to show fullsize