


1Laboratory for Molecular Dermatology and 2Laboratory of Hemato-Oncology, Felsenstein Medical Research Center, Tel Aviv University, Petach Tikva, 3National Hemophilia Center and Thrombosis Unit, Sheba Medical Center, Tel Hashomer, Ramat Gan, 4Sackler School of Medicine, Tel Aviv University, Tel Aviv, Israel, 5Laboratory of Hematology, 6Thrombosis and Hemostasis Unit, and 7Department of Dermatology, Beilinson Hospital, Rabin Medical Center, Beilinson Hospital, Petach Tikva 4941492, Israel. *E-mail: Aidainbal@hotmail.com
#These authors contributed equally to this work.
Accepted Aug 16, 2016; Epub ahead of print Aug 18, 2016
Fibrinogen-like protein 2 (FGL-2)/fibroleukin (also known as FGL-2 prothrombinase) is a serine protease, similar to activated coagulation factor X (Xa), capable of directly cleaving prothrombin into thrombin, an essential factor in the coagulation cascade (1). FGL-2 is expressed on the surface of monocytes/activated macrophages and endothelial cells and secreted by peripheral blood CD4+ and CD8+ T cells (2, 3).
Studies have reported an increase in FGL-2 protein and mRNA expression in various types of solid tumours (4), suggesting a role of FGL-2 in tumour progression. These findings were supported by our recent study showing increased FGL-2 activity in peripheral blood mononuclear cells (PBMC) of patients with B-cell lymphoma (5). The proposed mechanisms by which FGL-2 affects tumour development are enhancement of tumour cell proliferation, induction of angiogenesis promotion of immune suppression (6), and generation of thrombin leading to thrombin-mediated tumourigenesis (4).
Mycosis fungoides (MF) is the predominant subtype of primary cutaneous T-cell lymphoma (7). “Early MF” is characterized by patches and plaques in the absence of evidence of extracutaneous spread, and “late MF” is characterized by tumours and erythroderma. The majority of affected patients have early MF, and an estimated 20–30% progress to late MF (8). MF often poses a diagnostic challenge, especially in the early patch/plaque stage, owing to its overlapping features with benign dermatoses, such as psoriasis and atopic dermatitis (9). The histopathological diagnosis of early MF is one of the most controversial issues in dermatopathology (10, 11), and there is no non-invasive diagnostic biomarker that may assist clinicians in distinguishing early MF from inflammatory dermatoses.
In the present work we studied FGL-2 activity in PBMC of patients with MF and compared it with controls.
The study group consisted of 20 consecutive patients with MF, 14 early-stage (I–IIA) and 6 late-stage (IIB–IVB) between April 2013 and February 2015. Findings were compared with 2 control groups: 101 healthy volunteers (medical personnel) and 21 patients diagnosed with an inflammatory T-cell-mediated dermatoses (psoriasis vulgaris or atopic dermatitis).
Staging of MF was determined according to the criteria of the International Society for Cutaneous Lymphomas (ISCL)/European Organization for Research and Treatment of Cancer (EORTC) (7, 8, 12).
Blood samples were collected from all participants following written informed consent and approval by the ethics committee of the hospital.
FGL-2 prothrombinase activity was measured in PBMC (isolated as described in reference 5) by thrombin generation (TG) assay (5) with some modifications: PBMC extract containing 6.5 × 105 cells was suspended in a 500 µl reaction buffer (5) and homogenized by sonication for 1 min in a W385 sonicator (Labotal, Jerusalem, Israel). The sample containing approximately 62,000 cells was mixed with purified human prothrombin (Stago, Asnieres, France) to a final concentration of 5 µM. The reaction mixture underwent further incubations and centrifugations (as in (5)) and transferred to a flat-bottomed 96-well plate. A fluorogenic substrate (ZGGR-7-amido-4-methylcoumarin, ZGGR-AMC) (Stago, Asnieres, France) was added to a final concentration of 0.35 nM, and a fluorescent signal was measured by Fluoroskan Ascent® (Thermo Labsystems, Helsinki, Finland) at 400–460 nm. Thrombin generation was calculated as described previously (5). Quantitative RT-PCR analysis of fgl-2 mRNA in PBMC was performed as published before (5).
Analysis of variance (ANOVA) was used to assess differences in FGL-2 activity and mRNA (expressed as mean ± SEM), followed by post hoc analysis. A multivariate linear regression analysis was conducted to adjust for possible confounders. A receiver operating characteristic (ROC) curve was generated to measure performance of the FGL-2 activity assay. Statistical analyses were performed using SPSS ver.21.0 and GraphPad prism v.6. A p-value of < 0.05 was considered statistically significant.
The background characteristics of the 3 groups of participants and the treatment modalities used are shown in Table SI. There were no differences among the groups with regard to age, sex, percent lymphocytes, systemic treatment or phototherapy, although percent monocytes showed a trend for a statistical significance (p = 0.059).
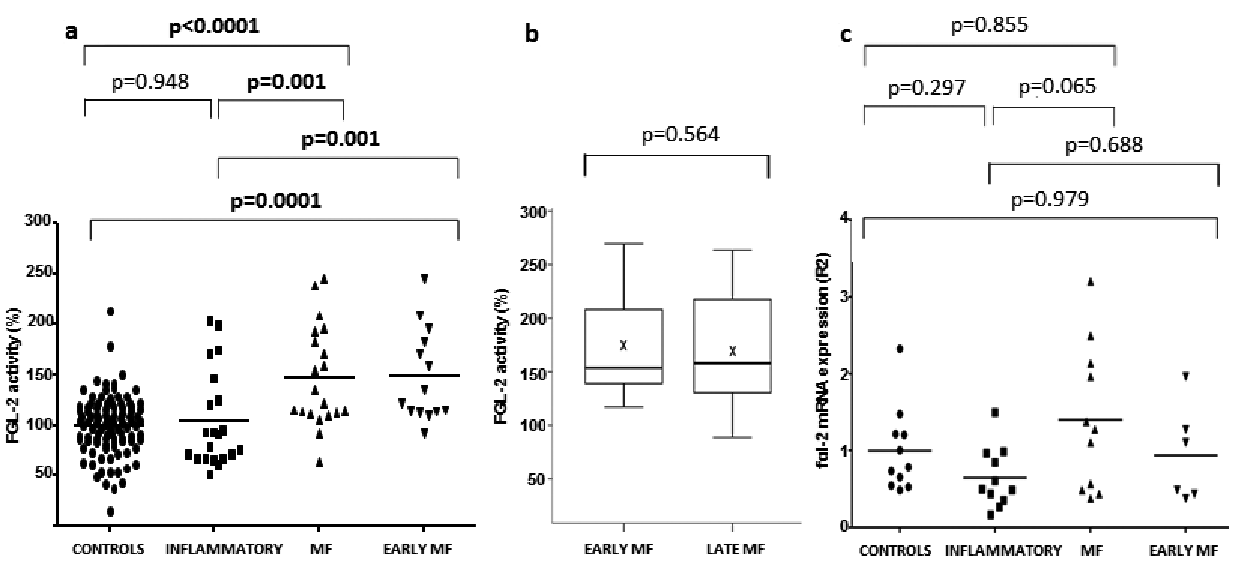
FGL-2 activity was increased almost 1.5-fold in patients with MF compared with normal controls (Fig. 1a; 147 ± 11% vs 100 ± 3%, p < 0.0001) and 1.4-fold compared with patients with inflammatory dermatoses (Fig. 1a; 147 ± 11% vs. 104 ± 10%, p = 0.001). There was no significant difference in FGL-2 activity between patients with early and late MF (Fig. 1b; 148 ± 12% vs. 144 ± 26%, p = 0.564). Separate analysis of PBMC of early MF subgroup showed 1.4-fold higher FGL-2 activity compared with that of patients with inflammatory dermatoses (Fig. 1a; 148 ± 12% vs. 104 ± 10%, p = 0.001). There was no significant difference in FGL-2 activity between healthy controls and patients with inflammatory dermatoses (p = 0.948).
Fig. 1. Fibrinogen-like protein 2 (FGL-2) activity and mRNA in peripheral blood mononuclear cells (PBMC). (a) Scatterplot presentation of FGL-2 activity in PBMC. Horizontal lines represent mean values. (b) Box-plot presentation of FGL-2 activity in PBMC according to mycosis fungoides (MF) subgroups. Horizontal lines represent median and × represents mean. All values are expressed as a percentage of mean FGL-2 activity in PBMC of healthy controls. (c) Scatterplot presentation of relative FGL-2 mRNA expression. Horizontal lines represent mean values. Values are expressed as quantification relative to mean FGL-2 mRNA expression in PBMC of healthy controls.a
Multivariate analysis conducted to study the effect of different variables on FGL-2 activity confirmed that age, sex, percent monocytes and lymphocytes had no effect (p = 0.215, p = 0.793, p = 0.631, p = 0.233, respectively), nor did previous systemic treatment or phototherapy in the MF and inflammatory dermatoses groups (p = 0.455 and 0.393, respectively).
ROC curve analysis yielded a good predictive estimate for the FGL-2 activity assay in discriminating between early MF and inflammatory dermatoses (AUC = 0.77, p = 0.008). At the optimal cut-off value of 103%, FGL-2 activity had a sensitivity of 93%, specificity of 67%, negative predictive value of 93%, and positive predictive value of 65%. Thus, FGL-2 activity successfully distinguished between early MF and inflammatory dermatoses.
Measurement of FGL-2 mRNA in PBMC performed in 11 individuals in each of the 3 groups showed no difference between early MF subgroup, inflammatory dermatoses and healthy controls (Fig. 1c). These results are in line with our previous study of patients with B-cell lymphoma (5), implying that the increase in FGL-2 activity observed in PBMC from patients with MF stems from the post-translational regulation of FGL-2 that governs its final activity. In addition, the presence of mutations or polymorphisms in FGL-2, resulting in alterations in its activity in MF, is a possibility. Indeed, previous study of 1,066 gene products showed that a linear correlation between proteins and corresponding RNA levels was present in only one-third of human genes (13).
The ISCL has created an algorithm to standardize the criteria for the diagnosis of MF (10, 11). At present no non-invasive biomarkers are available to differentiate MF from inflammatory dermatoses and current blood biomarkers are not routinely used (14). Measuring FGL-2 activity in PBMC is simple and rapid, with high reproducibility and accuracy, and therefore, could be included in the diagnostic algorithm of MF.
Multivariate analysis to test whether the increased FGL-2 activity in PBMC of patients with MF reflects monocytosis that is common in T-cell lymphoma (15), showed that FGL-2 activity was not correlated with the proportion of monocytes in the sample (p = 0.631). Similarly, FGL-2 activity was not affected by the proportion of lymphocytes in the sample (p = 0.233).
The drawback of this study is its relatively small cohort. In addition, due to the rarity of MF (12), previously treated or untreated patients were included, although the effect of treatment was excluded by multivariate analysis.


 Click to show fullsize
Click to show fullsize