


1Department of Dermato-Allergology and 2Department of Cardiology, Herlev and Gentofte Hospital, University of Copenhagen, DK-2900 Hellerup, 3The Danish Heart Foundation, 4The National Institute of Public Health, University of Southern Denmark, Copenhagen and 5Department of Dermatology, Aarhus University Hospital, Aarhus, Denmark. *E-mail: Kristian.kofoed@regionh.dk
Accepted Aug 16, 2016; Epub ahead of print Aug 18, 2016
Chronic urticaria (CU) is a common condition characterized by daily or almost daily occurrence of wheals, angioedema, or both over a period of more than 6 weeks (1). CU is classified into inducible (CIndU) and spontaneous forms (CSU).
The annual period prevalence of CSU was recently estimated in an Italian cohort as between 0.02% and 0.38%, whereas a German study showed a lifetime prevalence of CU at 1.8% (2, 3). While an association between CU and certain autoimmune diseases is well-established (3), CSU was surprisingly associated with obesity in a recent Italian study (4). Moreover, in a South Korean cohort of 131 patients with CU, metabolic syndrome was present in 30% of patients, and these individuals had particularly poor clinical outcomes and a more severe disease course (5). Finally, a population-based Taiwanese study of 9798 adults with CU recently showed that the condition was significantly associated with having received a prior diagnosis of hyperlipidaemia (6).
Despite the above observations, no study has examined a possible association between CU and cardiovascular (CV) disease. We therefore investigated the risk of myocardial infarction (MI), ischaemic stroke, CV death, and major adverse CV events (MACE; a composite of MI, ischemic stroke, and CV death), in patients with CU and CIndU, respectively, in a nationwide cohort using prospectively collected administrative data.
Study approval ref. 2007-58-0015; approval from an ethics committee is not required for register studies in Denmark. Danish nationwide administrative registers were linked at individual-level, including the Danish Register of Medicinal Products Statistics (records all pharmacy-dispensed prescriptions), the National Patient Registry (contains data on all in- and outpatient hospital contacts, and hospital administered medication), and the National Causes of Death Registry (records causes of deaths). Information on income is recorded by Statistics Denmark.
We identified all patients aged 18 years or older with a first-time diagnosis of CU between 1 January 1997 and 31 December 2012. The index date for cases was the date of first diagnosis, and patients were matched 1:30 with healthy controls. Index date for controls was the index date for the corresponding cases, and the cohort was followed until migration, death from any cause, or the occurrence of an endpoint, whichever came first. A study flow chart is available in Fig. S1. The primary endpoints were a diagnosis of MI, ischemic stroke, CV death, and MACE, respectively.
Baseline treatment up to 6 months before study inclusion was defined for azathioprine, cholesterol lowering drugs, cyclosporine, methotrexate, montelukast, and omalizumab. Baseline comorbidity was assessed up to 5 years prior to study inclusion for alcohol abuse, cardiovascular disease, diabetes, and hypertension. We calculated an index of socioeconomic status (standardized by age) between 0 (lowest) and 4 (highest) based on the average gross annual income during a 5-year period before study inclusion.
We described baseline characteristics with means and standard deviations for continuous variables and frequencies and percentages for categorical variables. Incidence rates were summarized per 1,000 person-years, and Cox regression analyses were performed to estimate crude and fully adjusted (adjusted for age, sex, socio-economic status, medication, and comorbidity) hazard ratios (HRs), respectively. Model assumptions were tested and found to be valid. p < 0.05 was considered significant and results were reported with 95% confidence intervals (CIs) where applicable. All analyses were performed using SAS v9.4 and STATA v13.0. Presentation of data on less than 3 individuals is not permitted, thus results of 1 or 2 events or individuals are shown as < 3.
After excluding patients with incomplete information due to migration, the final study population comprised a total of 2,215 patients with CU, and 66,203 age- and sex-matched controls. Similarly, for CIndU we identified 977 study cases and 28,497 corresponding controls. The baseline characteristics are shown in Table SI, and characteristics were generally similar between cases and controls, albeit with a slightly higher prevalence of hypertension and cardiovascular disease among study cases at baseline.
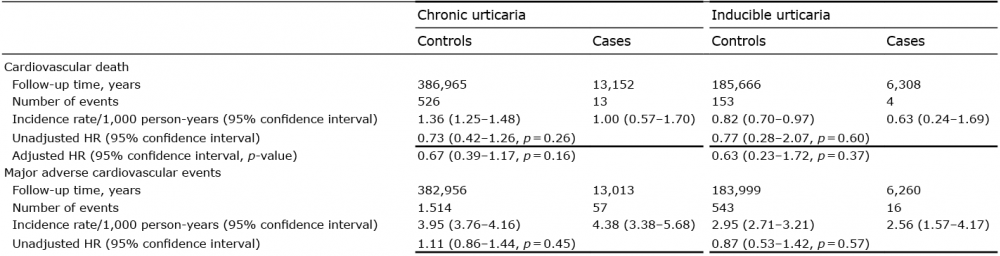
The incidence rates were generally comparable between cases and controls (Table I), and after adjustment for potential confounding factors, there was no significantly increased risk of MI (adjusted HR 1.18 [0.79–1.76]), ischaemic stroke (adjusted HR 1.03 [0.70–1.52]), CV death (adjusted HR 0.67 [0.39–1.17]), or MACE (adjusted HR 1.09 [0.83–1.42]), respectively. Similarly, there was no increased risk in any of the study outcomes in patients with CIndU, as shown in Table I. When analyses were limited to patients with CSU, there were no significant changes to any of the observed results (data not shown).
Table I. Follow-up time, number of events, incidence rates, and hazard ratios (HR) of myocardial infarction, ischaemic stroke, cardiovascular death, and major adverse cardiovascular events, respectively (for complete details see Table SII)
In our nationwide cohort, we found no association between CU and CV disease. The same was the case in analyses of patients CIndU patients only. While alterations in lipid metabolism and obesity could play a role in the aetiopathogenesis of CU, there appears to be no relationship with CV comorbidity. It is possible that the relatively short disease duration in patients with CU is insufficient to generate putative arteriosclerosis from systemic low-grade inflammation. Indeed, other chronic skin conditions that have been associated with CV disease, such as psoriasis (13) and hidradenitis suppurativa (12), are characterized by a more persistent course. Certain limitations and strengths apply to the present study. While our study benefited from the nationwide design, patients were limited to those seen in a hospital setting, which may represent a selected population. Moreover, we lacked information regarding disease severity, and constitutional factors, such as body mass index (BMI), potentially obscuring an association with CU. However, since recent studies have associated CU with obesity, this would arguably have resulted in an overestimation of the true CU-associated risk. Also, we were unable to examine the effect of disease duration on the risk of adverse CV outcomes. In addition, while the maximum follow-up was 31 December 2012, omalizumab was not approved for use in CU at that time, and we are therefore unable to determine the potential effects of omalizumab on the CV risk. Lastly, the Danish population is predominantly Caucasian, which may limit extrapolation to other ethnicities. In conclusion, while we did not observe any increased CV risk in patients with CU or CIndU, further studies are warranted to confirm our findings.
Conflicts of interest: KK has served as an advisory board member for Novartis and received research grants from Novartis. CV has received fees as a speaker from Novartis and is a Novartis advisory board member.


 Click to show fullsize
Click to show fullsize