


1Service de dermatologie-allergologie, 3Service d’anatomie pathologique and 4Service de médecine interne, Hôpital Tenon, AP-HP, 4, rue de la Chine, FR-75020 Paris, and 2Université Paris VI, Paris, France. *E-mail: sarah.guegan.bart@gmail.com
Accepted Oct 6, 2016; Epub ahead of print Oct 10, 2016
Amicrobial pustulosis of the folds (APF) is characterized by relapsing pustular lesions associated with erosive macerated areas and crusts, affecting the cutaneous folds, face and scalp (1). It is usually reported in females in the third decade, mainly in association with systemic and cutaneous lupus erythematosus and, rarely, with connective tissue disease, scleroderma, myasthenia gravis, Hashimoto’s thyroiditis, idiopathic thrombocythemia and coeliac disease (1–4).
APF belongs to the spectrum of neutrophilic dermatoses, diseases all characterized by similar pathological features, namely an intense inflammatory infiltrate composed primarily of neutrophils, in the absence of patent infection. In APF, intraepidermal subcorneal spongiform abscesses are associated with a neutrophilic dermal infiltrate. Diagnostic criteria were established by Marzano et al. in 2008 (Table SI) (2).
We report here a case of refractory APF, which preceded by 11 years the onset of lupus erythematosus tumidus (LET), and by 15 years the onset of Crohn’s disease (CD). Both APF and CD were controlled by ustekinumab, a monoclonal antibody directed against the p40 subunit common to interleukin (IL)12/IL23.
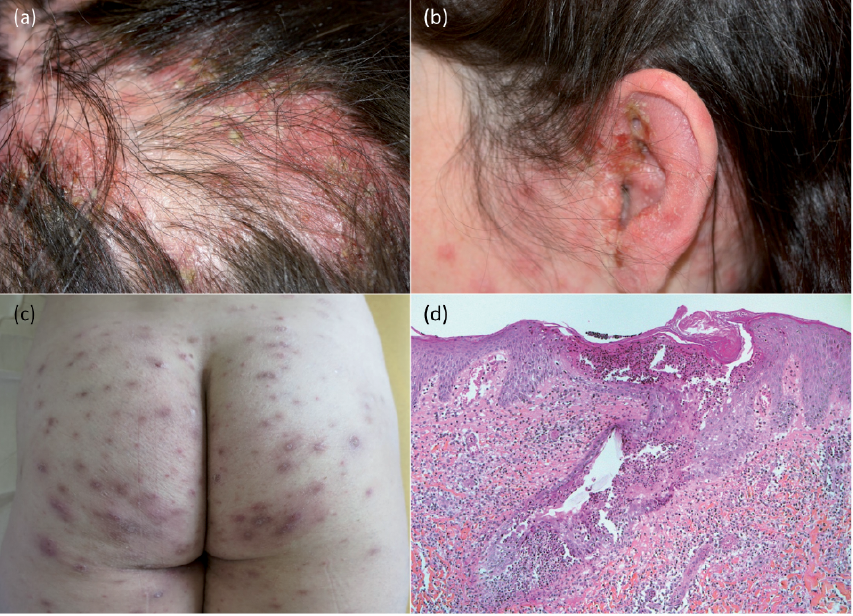
A 26-year-old woman was referred for evaluation of recurrent episodes of pustular skin lesions affecting predominantly her major body folds over the last 10 years. Upon examination, the patient was healthy, afebrile. Axillary, submammary and inguinal folds were involved with multiple symmetrically distributed erythematous pustules. The gluteal folds, perianal area and buttocks were mostly affected (Fig. 1a). Isolated pustules were observed on the arms, back, abdomen and thighs. Nikolsky’s sign was negative. In the course of evolution, similar lesions involved the face and scalp, together with erosive and crusted lesions (Fig. 1b). Pustular lesions affecting the scalp eventually coalesced into larges plaques with hair loss, quickly followed by regrowth. All of these lesions regressed following topical corticosteroid therapy, and relapsed after withdrawal of treatment. Histology of skin biopsy specimens revealed intraepidermal subcorneal spongiform abscesses as well as a dermal inflammatory infiltrate with predominant neutrophils (Fig. 1c). Direct immunofluorescence of lesional skin showed non-specific IgM deposits at the dermoepidermal junction. Micro-biological cultures from recent closed pustules were sterile. A diagnosis of APF was thus established.
Fig. 1. A case of refractory amicrobial pustulosis of the folds. (a–c) Crusted erythematous pustular lesions of the scalp, ear and buttocks, respectively. (d) Haematoxylin-eosin staining showing spongiform subcorneal epidermal and follicular pustule with a mixed neutrophil and mononuclear infiltrate in the upper and middle dermis (original magnification ×200).
Of note, 11 years after the onset of APF, the patient presented smooth erythematous infiltrated plaques affecting the face. Histology confirmed LET. Antinuclear antibodies (ANA) were positive, with a titre of 1:320 and a nuclear speckled pattern; search for other autoimmune antibodies (anti-dsDNA, anti-SS-A, anti-SS-B, anti-Sm, anti-RNP, ANCA) was negative. Hydroxychloroquine (200 mg twice daily) combined with a short course of topical corticosteroids was quickly effective in treating LET with no further relapse.
Initially, various courses of treatment failed to control APF: topical and systemic corticosteroids (up to 1.5 mg/kg/day), colchicine (2 mg/day), isotretinoin (40 mg/day), hydroxychloroquine, dapsone (100 mg/day), and zinc (30 mg/day). When necessary, bacterial superinfections were treated with empirical antibiotic therapy. The patient responded partially to a 4-year course of cyclosporine (5 mg/kg/day) with gradual tapering. After 4 years of this treatment, as no complete remission was seen, anakinra (100 mg daily subcutaneously) was introduced and continued for 2 years; a significant decrease in the episodes of flare-ups was noted.
Fifteen years after the onset of APF, the patient experienced persistent weight loss and abdominal pains. Upper and lower gastrointestinal endoscopy and biopsies revealed erosive pancolitis with epithelioid cell granuloma, a diagnostic characteristic of CD. In the months following CD diagnosis, several flares of APF occurred. Anakinra was stopped; ustekinumab was introduced at a dose of 90 mg subcutaneously every 8 weeks and has been on-going for the last 2 years. Ustekinumab was well tolerated with no adverse effects and CD symptoms subsided quickly. APF was controlled by the concomitant use of ustekinumab and cyclosporine within 3 months; 6 months after ustekinumab initiation, secondary adjunction of methotrexate (25 mg/week) allowed cyclosporine tapering. Hydroxychloroquine treatment was never discontinued, and prevented LET relapses.
In the case of our patient, obligate criteria for AFP were fulfilled. Two minor criteria were also present: association with 2 autoimmune disorders, LET and CD, and positive ANA with a titre of 1:320. Differential diagnoses that could be considered were a pustular variant of disseminated pyoderma gangrenosum (PG) or the vesiculopustular eruption that may accompany inflammatory bowel diseases (IBD). However, the diffuse prolonged and recurrent evolution of the cutaneous symptoms and their preceding CD by 15 years were not in favour of the latter that is milder and not specifically localized in cutaneous folds or scalp. In the 15 years of evolution of skin manifestations, pustules never progressed clinically toward lesions of ulcerative PG, the most frequent form in patients with IBD (5).
APF has been reported in association with coeliac disease (1), but to our knowledge, this is the first case of APF associated with IBD. IBD may be associated with various neutrophilic dermatoses (ND) (6) such as PG, Sweet’s syndrome, bowel-associated dermatosis-arthritis syndrome, pyostomatitis vegetans, and extracutaneous aseptic abscesses (7).
Immunomodulatory therapies are the mainstay of treat-ment of ND, corticosteroids and cyclosporine being the drugs most commonly used. These treatments have also been given in cases of APF (2). In our patient, cyclosporine incompletely prevented flares of the disease during 4 years.
Anti-IL-1 receptor antagonist anakinra is another alternative in cases of refractory ND, such as Sweet’s syndrome (8, 9) and neutrophilic panniculitis (10). Amazan et al. (11) reported a dramatic response to anakinra with complete remission in a patient with APF, and indeed, expression of IL-1β and its receptors I and II is increased in the skin of these patients (12). In our patient, anakinra partially stabilized APF during 2 years with reduction in flare numbers and intensity. It had to be discontinued following CD diagnosis and new flares of APF.
Case reports and placebo-controlled trials have also underlined the relevance of anti-tumour necrosis factor (TNF)-α therapy as a first-line treatment in the case of PG associated with IBD (13). However, TNF-α inhibitors were not considered as a first-line therapy in our patient because of LET. Ustekinumab is a human monoclonal antibody against IL-12 and 23, approved for the treatment of moderate to severe plaque psoriasis and psoriatic arthritis, and effective in inducing and maintaining remission in patients with CD (14). IL-23 plays a critical role in driving inflammation associated with IL-17 production and especially neutrophil recruitment, and cases of patients with cortico-resistant PG successfully treated with ustekinumab have recently been reported (15, 16). Ustekinumab was used successfully in our patient in association with cyclosporine and, secondarily, metho-trexate, which allowed cyclosporine tapering.
Conflicts of interest: SG was supported by Janssen for international and national conference attendance.


 Click to show fullsize
Click to show fullsize