


1Departments of Dermatology, Venereology, Allergology and Immunology and 8Institute for Clinical Chemistry and Microbiology, Dessau Medical Center, Dessau, Germany, 2Humanitas Clinical and Research Center, Milan, Italy, 3Université Paris Descartes, Sorbonne Paris Cité, 4Inserm U1151, équipe 11 “Physiopathologie des infections systémiques”, 5Institut Pasteur, Centre Médical, Service de Pathologie Infectieuse et Tropicale, 6Centre d’Infectiologie Necker-Pasteur, Paris, France, and 7Institute for Health Services Research in Dermatology and Nursing, University Medical Center Hamburg, Hamburg, Germany
#These authors contributed equally to the study.
It is unclear whether bacterial colonization in hidradenitis suppurativa/acne inversa (HS) comprises a primary cause, triggering factor or secondary phenomenon of the disease pathogenesis. Furthermore, the connection between certain bacterial species, the disease severity and its localization is unknown. Bacterial species were isolated from HS lesions to reveal a potential correlation with localization and disease severity. Ninety swab tests were prospectively obtained from 90 HS lesions of 50 consecutive patients. The material was cultured under aerobic and anaerobic conditions. The identified species were statistically correlated with Hurley stage and localization of the lesions. The most prevalent isolates were reported. Hurley stage significantly correlated with disease localization. Particular bacterial species were associated with “extended” disease and Hurley III stage with the detection of both aerobic and anaerobic bacteria and with a higher number of species. The presence of bacterial species is dependent on the local milieu, which correlates with the localization of the disease, its clinical manifestations and its extension.
Key words: hidradenitis suppurativa; acne inversa; bacteria; aerobic; anaerobic; microbial colonization; Hurley stage.
Accepted Nov 23, 2016; Epub ahead of print Nov 24, 2016
Acta Derm Venereol 2017; 97: XX–XX.
Corr: Christos C. Zouboulis, Departments of Dermatology, Venereology, Allergology and Immunology, Dessau Medical Center, Auenweg 38, DE-06847 Dessau, Germany. E-mail: christos.zouboulis@klinikum-dessau.de
Hidradenitis suppurativa/acne inversa (HS) is a chronic, inflammatory, recurrent, debilitating disease of the terminal hair follicles that usually manifests after puberty with painful, deep-seated, inflamed lesions in the apocrine gland-bearing areas of the body, most commonly the axillary, inguinal and anogenital regions (Dessau definition, 1st International Conference on hidradenitis suppurativa, 30 March–1 April 2006, Dessau, Germany) (1). The pathogenesis of the disease is probably multifactorial. Genetic predisposition, cellular and immunological agents, nutrition, adipositas and smoking are among the suspected factors (2).
Bacterial colonization in HS, both aerobic and anaerobic, has only been sporadically investigated in recent years (3, 4). Despite recent analysis of the skin microbiome (5), there is no evidence as to how bacteria could be involved in HS pathogenesis and lesion development (6).
In 1999, Brook & Frazier (7) reported the isolation of aerobic and anaerobic bacteria from lesions of 17 patients with HS, claiming a possible involvement of bacteria in the occurrence of the disease. However, the study included only axillary lesions. Staphylococci and streptococci, peptostreptococci, Prevotella, Fusobacterium and Bacteroides spp. were the majority of the isolated aerobic and anaerobic bacteria (7). In a study performed on skin cysts and abscesses without strict association with HS a strong involvement of staphylococci and streptococci, but also of Peptostreptococcus and Prevotella spp, was identified (8).
Recently, samples of 10 patients with HS before and after treatment with carbon dioxide laser revealed coagulase-negative staphylococci, Corynebacterium spp. and alpha-haemolytic streptococci were detected at various levels among the aerobic bacteria (8), whereas Gram-positive cocci were the most common species in another study (9). From the microbiologist’s point of view, HS was reported as a bacterial biofilm disease, with staphylococci and streptococci being the most prevalent bacteria (10).
In the current study, swab tests were obtained from HS lesions (axillae, inguinofemoral, submammary as well as gluteal region and, in individual cases, from the scalp, head and neck as well as the periumbilical region/lower abdomen) of a consecutive series of 50 patients in a prospective manner. The collected material was cultured under both aerobic and anaerobic conditions and the results show the colonization of aerobic and anaerobic bacteria into HS lesions.
The primary aim of this study was to elucidate a potential correlation between certain bacterial families or species with the disease localization and its severity. This information can secondarily lead to the discovery of connections between bacteria and HS manifestation patterns, as well the development of more effective thera-peutic strategies.
The Hurley criteria for static/anatomical classification of HS severity were applied to patients with HS, as initially published by Hurley (11) and further defined by Zouboulis & Tsatsou (12). Body mass index (BMI) and smoking status were assessed among the demographic characteristics of the study population.
Ninety swab tests were performed in a prospective manner in 90 skin lesions of 50 consecutive patients (29 men and 21 women) with HS. The tests were performed at the Dessau Medical Center, from December 2010 until June 2011. Swabs from patients who had received antibiotics were obtained after a minimum 3-month wash-out phase. No other exclusion criteria were applied. Ten patients were diagnosed with Hurley stage I (20%), 22 with Hurley stage II (44%) and 18 with Hurley stage III (36%). The characteristics of the study population are shown in Table I. The tests were performed after careful disinfection of the lesions with 1% octenidine HCl/2% phenoxyethanol 3 times, in order to avoid isolation of species of the skin surface that belong to normal skin flora. For the optimal maintenance of microorganism viability, the specimens were collected after gentle pressure and extrusion of the purulent material of the lesions with a special swab (ESwab, Copan Diagnostics, Murrieta USA). The specimens were then immediately transferred into a swab tube, which contained an appropriate medium for the short-term maintenance of aerobic and anaerobic bacteria (modified liquid Amies transport medium). The samples were ideally processed within 2 h after collection or were stored at 4–8°C and processed within 48 h, according to the manufacturer’s protocol. The medium containing the samples was then brought onto Petri dishes containing 5% sheep blood agar (Oxoid, Wesel, Germany) for the culture of aerobic bacteria or Schaedler agar + 5% sheep blood (bioMérieux, Nürtingen, Germany) for the culture of anaerobic bacteria. The minimal incubation time for aerobic bacteria was 24 h and for anaerobic bacteria 48 h at 36°C.
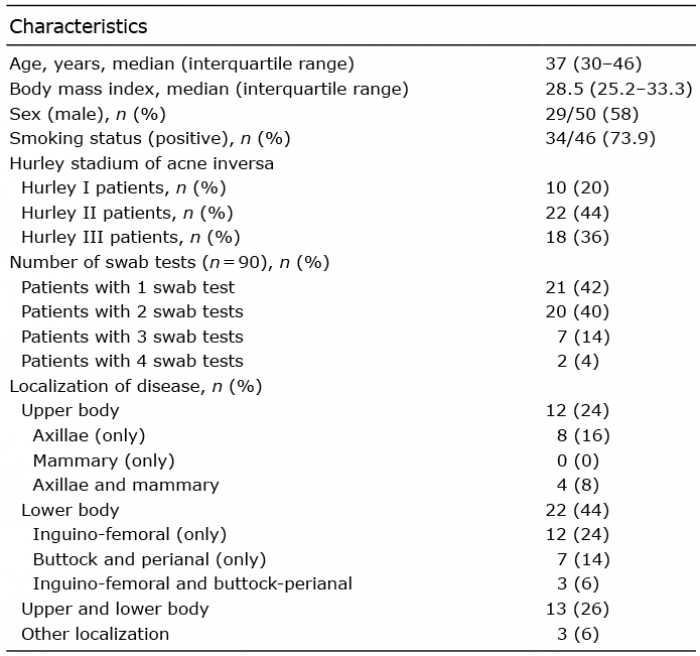
Table I. Demographic characteristics of the study population (n = 50)
Thirty-nine different bacterial species were isolated through this procedure. In case of bacterial growth, bacteria were identified automatically after Gram-staining with advanced colorimetric technology using a VITEK 2 device (bioMérieux).
Because most of the variables exhibited a non-normal distribution, descriptive statistics are presented as medians and interquartile ranges (IQR) or as percentages when appropriate. Non-parametric tests (Pearson’s χ2 test, Fisher’s exact test, two-sample Wilcoxon rank-sum (Mann-Whitney) test; and Kruskal-Wallis (equality-of-populations) rank test) were used for statistical evaluation. In order to gain further insight into the variables that are independently associated with an individual’s likelihood of being classified into a higher Hurley stage, ordered logistic regression analysis was performed. Covariates included in the univariate and the multivariate models were either binomial (smoking status, sex), categorical (localization of disease, type of bacteria isolated) or continuous variables (age, BMI). In univariate analyses, a criterion of p ≤ 0.10 was used to identify candidate predictors. Then, a multivariate model was fitted and a backwards selection procedure was used to eliminate those variables that were not significant in the multivariate framework. A criterion of p ≥ 0.05 was applied for determining which variables to eliminate. The proportional odds ratios (OR) derived from the ordered logistic regression models refer to the odds of being in a higher, rather than lower, Hurley stage of HS, with Hurley III stage been the highest category of severity, and are presented with their 95% confidence intervals (95% CI) and respective p-values. For hypothesis testing, a probability level < 0.05 was considered statistically significant. All statistical tests were 2-sided. Stata software was used for all statistical analyses (Stata Corp., College Station, TX, USA).
Ninety swab tests were performed from 90 lesions of 50 consecutive patients with HS in a prospective manner, from various localizations. In 40 patients at least 2 localizations were actively affected and 2 of them were examined; in 10 patients one anatomical site was affected and examined. The most commonly affected areas were the inguinofemoral region (32%), followed by the axilla (24%), the gluteal/perianal region (17%), and the submammary region (10%) (Fig. S1). The demographic characteristics of the study population, including age, BMI and smoking status, and the percentages of each localization affected by the disease are shown in Table I.
The families and species of the isolated bacteria are summarized in Table II.
Table II. Prevalence of bacterial isolates in hidradenitis suppurativa lesions of the study population (presented as % of patients (some of the patients had multiple isolates))
Staphylococcus aureus, one of the most common species of the human skin flora, was isolated in 26% of patients, as well as the coagulase-negative staphylococci, such as S. epidermidis, S. hominis, S. lugdunensis, S. simulans, S. capitis, S. auricularis and S. haemolyticus, with predominant species the S. epidermidis. B-hemolytic streptococci (Streptococcus agalactiae, Streptococcus dysgalactiae, Streptococcus group G) were identified in 10% of the patients and facultative anaerobic enterococci (e.g. Enterococcus faecalis spp) in 12% (see also Table I). Bacteria of the Enterobacteriaceae family (Proteus mirabilis, Eserichia coli, Klebsiella pneumoniae, Moxarella morganii, Serratia marcescens, Enterodbacter cloacae, Citrobacter koseri) were isolated from 30% of the study population, with P. mirabilis and E. coli being the most prevalent. The family of obligate anaerobic Gram-negative rods (Prevotella bivia, P. disiens, P. intermedia, P. melaninogenica, P. oralis, Bacteroides ovatus, B. fragilis, B. thetaiotaomicron, Fusobacterium varium) was detected in 42% of the patients, with the species P. bivia, P. disiens and B. fragilis being the most frequent. Anaerobic enterococci were isolated in 14% of the patients (Table I, Fig. 1 and Fig. S2).
Fig. 1. Bacterial colonization related to hidradenitis suppurativa disease severity (Hurley).
Our study showed that the Hurley stage was associated with localization of the disease. Most of the patients with HS lesions localized in both the upper and the lower body (n = 9; 69.2%) were classified as Hurley stage III, while most of the patients of the other 2 localization categories (upper body only or lower body only) were classified as Hurley stage II (Table III).
Table III. Evaluation of the association between Hurley stage and localization of the disease
First, we evaluated the association between Hurley stage and the number of species isolated from each patient using the non-parametric Kruskal–Wallis (equality-of-populations) rank test. Hurley stage III was associated with higher number of species isolated (p < 0.05) (Table IV).
Table IV. Association of Hurley stage with number of isolated species and presence of anaerobic and aerobic bacteria, respectively. Hurley stage I was associated with no isolation of clinically relevant bacteria, whilst Hurley stage III mostly correlated with isolation of both aerobic and anaerobic bacteria
Secondly, we evaluated the correlation between the type of bacteria isolated (anaerobic, aerobic, both) from each patient and Hurley stage. The Hurley stage of the disease and the species of bacteria isolated (none, aerobic, anaerobic, or both aerobic and anaerobic) were associated. A correlation of patients with Hurley stage II and the isolation of either aerobic (53.3%) or anaerobic (42.9%) species, but not both, was determined. Moreover, we observed that most patients with isolation of both aerobic and anaerobic bacteria (11 of 16; 68.8%) were classified to Hurley stage III (see Table IV).
Finally, we evaluated the association of Hurley stage with the isolation of specific bacteria types, one-by-one (Table SI). Isolation of the species of S. aureus (p < 0.05), Streptococci (p < 0.01), Enterobacteriaceae (p < 0.05) and obligate anaerobic Gram-negative rods (p < 0.05) was associated with higher Hurley stage2.
2More analytically
The association between the localization of HS and the number of species isolated from each patient was evaluated using the non-parametric Kruskal–Wallis (equality-of-populations) rank test. The localization of the disease was not associated with the number of species isolated from each patient (p = 0.068) (Table SII). However, when localizations were grouped as “only in the upper body” (n = 12) and “only in the lower body” (n = 22) and compared with the group of patients with localization of lesions in “both upper and lower body” (n = 13), the result was statistically significant (p = 0.028) (Table SII).
We have considered as “extensive disease” the synchronous prevalence of HS lesions in both the upper and lower body and we subsequently evaluated the association of “extended disease” with the detection of the bacterial families, one by one. Isolation of coagulase-positive staphylococci and streptococci was associated with concomitant prevalence of HS in both the upper and lower body (see Table SII)3.
3More analytically
Finally, ordered logistic regression analysis was performed; both univariate analyses and in a multivariate model (Table V). In the univariate analyses, the localization of HS lesions of both the upper and the lower body (p = 0.031) and the isolation of aerobic (p = 0.028) or of both aerobic and anaerobic bacteria (p < 0.001), were found to predict a higher disease severity. However, in the multivariate model, only the isolation of both aerobic and anaerobic bacteria independently predicted a higher severity of the disease (p = 0.004), while the localization of HS lesions to the lower body was only associated with a lower disease severity (p = 0.016).
Table V. Ordered logistic regression analysis’ results, using “Hurley stage” as the outcome variable
Follicular occlusion (13) and activation of the innate immunity (14) may be the initiation factors of HS. Antimicrobial peptides, such as cathelicidin (LL-37), human β-defensin 3 (hBD3), and chemokines, such as interleukin (IL)-8, tumour necrosis factor (TNF-α), α-melanocyte stimulating hormone (α-MSH) and macrophage migration inhibitory factor (MIF) were found to be increased in HS in comparison with apparently normal skin of HS patients (14). Furthermore, HS lesions exhibit a stronger expression of Toll-like receptor 2 within infiltrating macrophages and dendritic cells (15). However, the role of bacterial colonization as a trigger or a simple result of altered innate immune response is unclear. Recently, differences in the microbiota (species and quantity) between HS axillary lesions and healthy controls were reported (16). Several current therapeutic algorithms include combinations of antibiotics, since bacteria were reported to form biofilms in HS lesions (17). Our results induce the question of the clinical significance of bacterial colonization for the progression of HS severity. The most common bacteria isolated were S. aureus, S. epidermidis, E. faecalis, E. coli, P. bivia and P. disiens. These anaerobic bacteria are often associated with common anaerobic infections, such as vaginitis and periodontitis (18, 19). In a recent study of 69 patients with HS, bacterial species were correlated with certain anatomical sites of HS lesions and antimicrobial resistance; staphylococci and E. faecalis were the most commonly isolated species, while Prevotella species were not detected (19).
This study represents one of the largest studies on HS bacteriology to date, which includes and correlates bacterial species with severity of disease and skin localization. Many of the previous studies faced the possibility of biases based on potential contamination of the samples with resident bacteria (8, 9). Sartorius et al. (8) used CO2 laser surgery to gain access to deeper sites of HS lesions and avoid contamination. In our study, the immediate dipping of the swabs in short-term maintenance medium has managed to isolate a high number of both facultative and obligate anaerobic bacteria from patients with both small and extensive lesions. Despite this, swab tests detected no bacterial isolates in 23% of the cases (21 of 90 swab tests). However, previous decontamination of the skin might have affected the viability of certain fragile bacteria during sampling. Moreover, extrusion was used to obtain the purulent material of the lesions and not surgical drainage. This might have underestimated certain bacteria in deeper portions of the HS lesions.
The presence of staphylococci in Hurley stages I and II was rather minimal and sta-phylococci, both coagulase-positive and negative, were isolated in a high percentage of Hurley stage III patients. Our data confirm the findings of Sartorius et al. (8), who did not isolate any S. aureus species from acute inflammatory nodules of HS exacerbations. This may suggest that S. aureus is involved at late stages of the disease, perhaps as a superinfection on an already developed lesion microenvironment from other species of bacteria. The isolation of staphylococcus is also linked to one of the causal factors of HS, namely smoking. The latter is known to promote colonization of S. aureus (13). A retrospective histological study of 27 patients conducted by Jahns et al. (17) failed to detect any staphylococci in any sample. The isolation of S. aureus, streptococci, Enterobacteriaceae and obligate anaerobic Gram-negative rods were all associated with higher Hurley stages of the disease. Moreover, coagulase-negative staphylococci were not detected from Hurley stage I patients. Both staphylococci and streptococci were associated with simultaneous localization from both the upper and lower body regions.
Another observation was that a high percentage of the intestinal flora species, the enterobacteriae, was detected in the gluteal and inguinal regions. From the inguinal regions, Enterobacteriaceae and anaerobic obligate anaerobic Gram-negative rods were mostly isolated. From the obligate anaerobic Gram-negative rods, Prevotella spp. was most prevalent. This corroborates with the results of Guet-Revillet et al. (20), where Prevotella spp. were the most frequently isolated Gram-negative rods. Furthermore, Prevotella spp. were the second most frequently anaerobic bacterial species isolated from HS lesions of the axilla, in another retrospective study (7). Other widely isolated bacteria were E. coli, E. faecalis, P. mirabilis and other species of Prevotella. Anaerobic enterococci and mostly Peptrostreptococcus spp., as well as Prevotella spp. were the most common bacteria from the axillary region in another small retrospective study (7).
In contrast to the recent study of Guet-Revillet et al. (20), we barely detected anaerobic actinomycetes (1 positive swab test) and milleri Group streptococci (only one positive swab test for S. anginosus). A reason for this might be the 48-h minimum incubation time for anaerobic cultures.
In fact, our study showed that patients with higher Hurley stages were positive for a more polymicrobial flora compared with the patients with lower stages. It also showed that isolation of particular species was associated with “extended” disease and that Hurley stage III was associated with isolation of both aerobic and anaerobic bacteria and with higher number of species. Taking into account that HS is not a classical infectious disease (no healing after antibiogram-oriented antibiotic treatment) and that it belongs to the group of hyperergic disorders (1), bacteria may, indeed, trigger an enhanced innate immune reaction, which can worsen the disease. On the other hand, bacterial colonization may be a neutral bystander, following the new milieu that it is associated with the localization, the clinical manifestations and the extension of the disease. The extent is, however, less possible, since antibiotic treatment induces some improvement to the magnitude of inflammation.
Therefore, it is possible that in the initial HS stages follicular plugging facilitates development – colonization with anaerobic bacterial species. Progression of the disease from inflammatory nodules and abscesses into fistules leads to subsequent colonization with facultative anaerobic and aerobic bacteria, which contributes to the development of extended disease characterized by lesions of both the upper and lower body predilection areas (Fig. 2).
The authors declare no conflicts of interest.
Fig. 2. Proposed hypothesis on bacteriology of hidradenitis suppurativa.


 Click to show fullsize
Click to show fullsize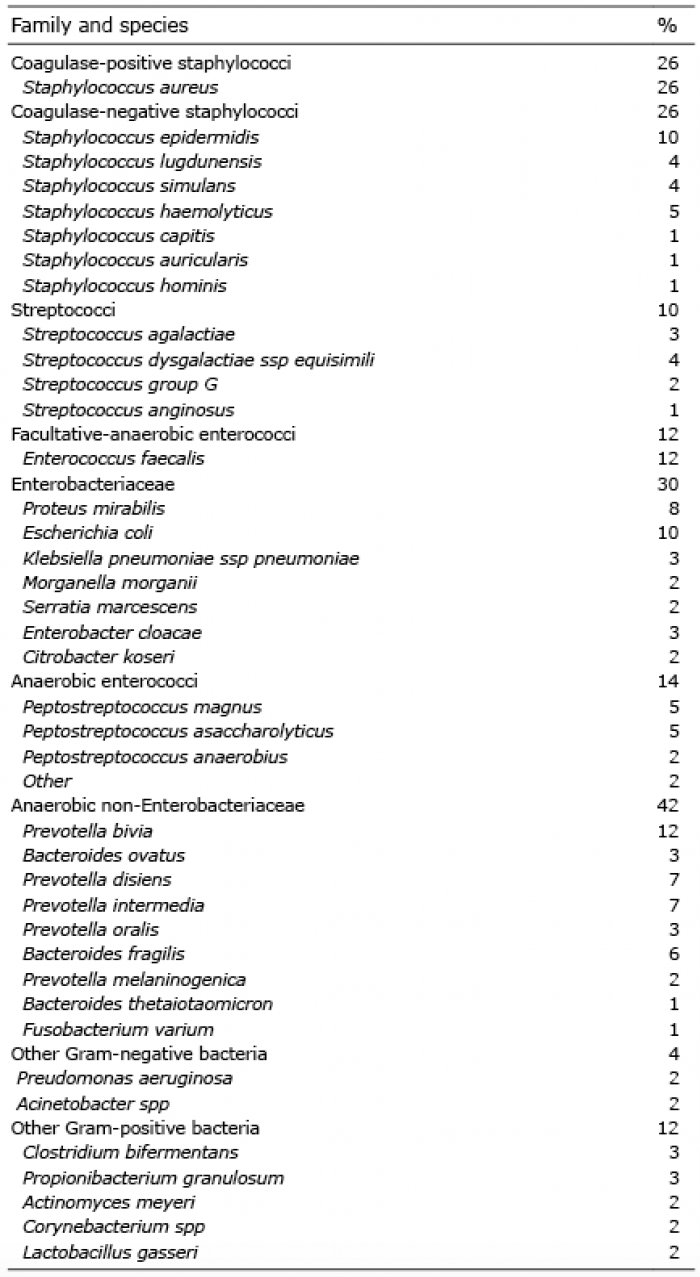 Click to show fullsize
Click to show fullsize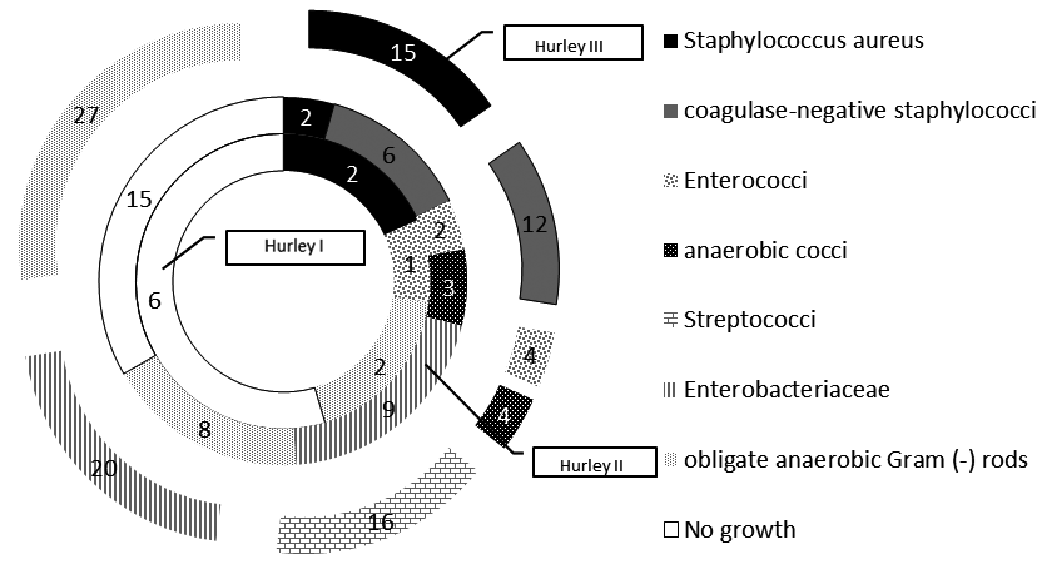 Click to show fullsize
Click to show fullsize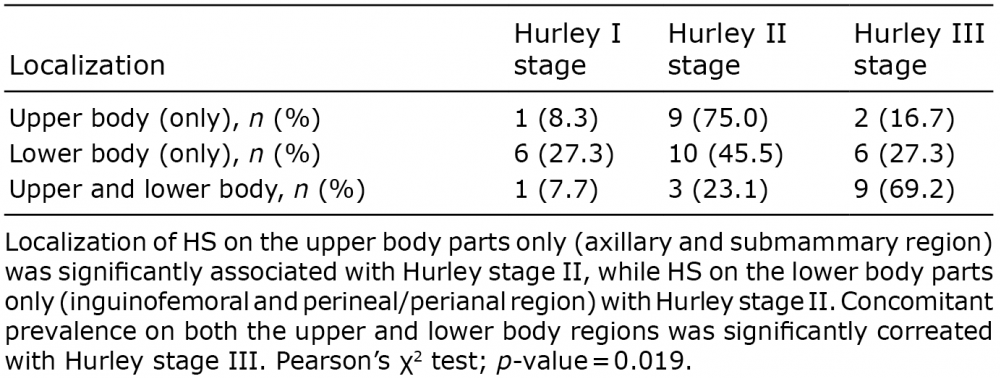 Click to show fullsize
Click to show fullsize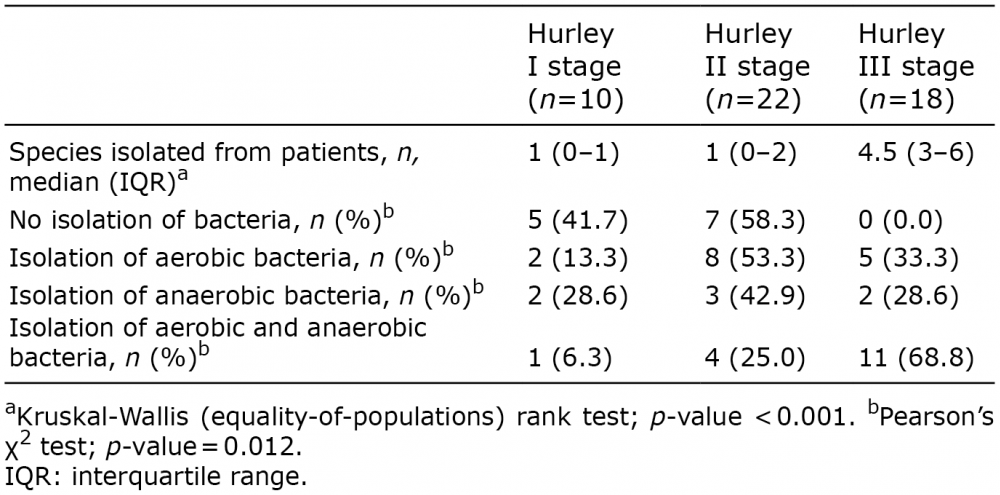 Click to show fullsize
Click to show fullsize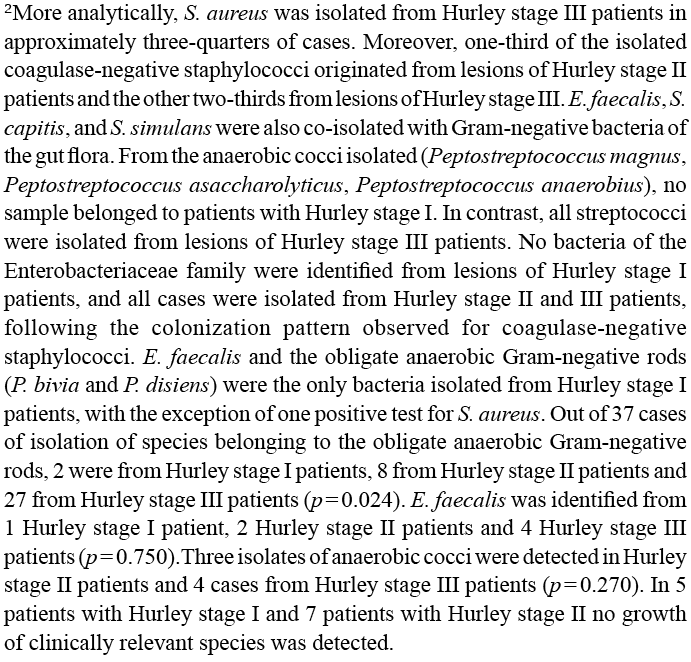 Click to show fullsize
Click to show fullsize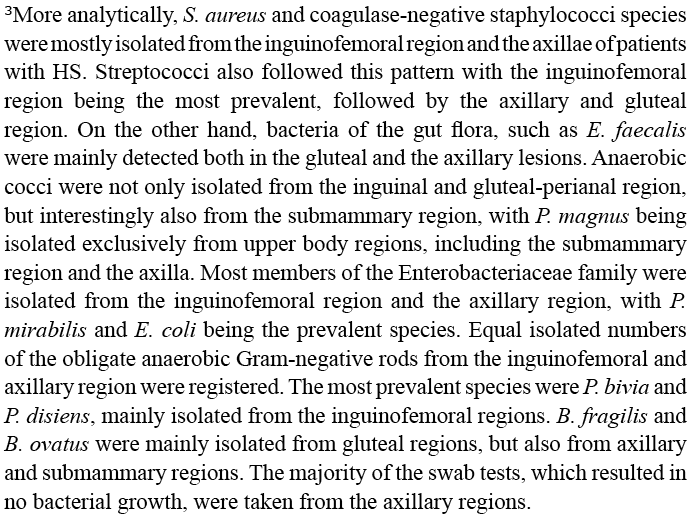 Click to show fullsize
Click to show fullsize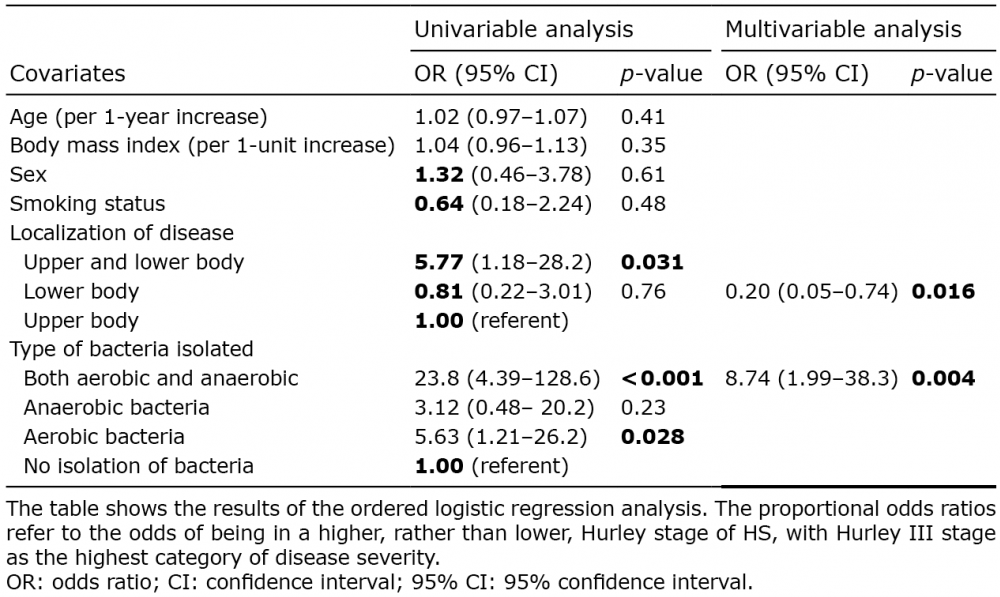 Click to show fullsize
Click to show fullsize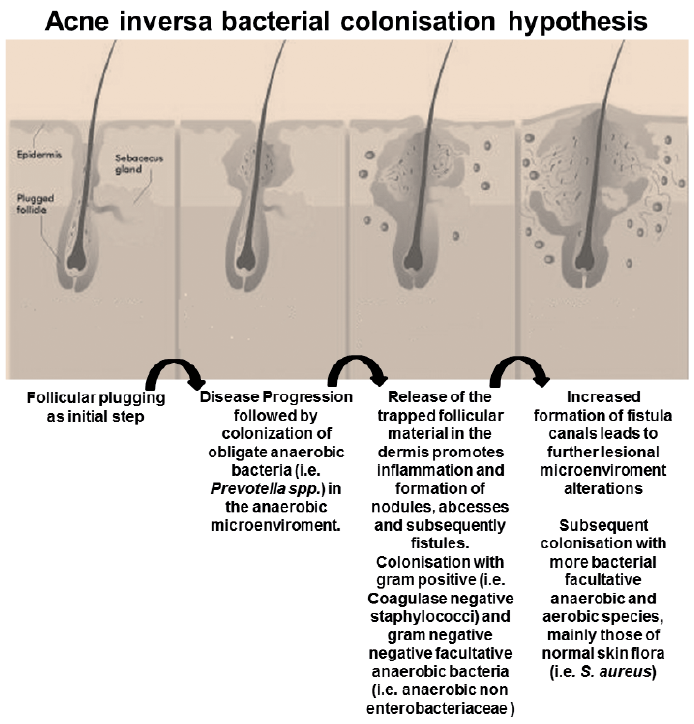 Click to show fullsize
Click to show fullsize