


1Department of Dermatology and Venereology, Sahlgrenska Academy, and 2Centre for Health Care Improvement, Chalmers University of Technology, Gothenburg, Sweden
Patients diagnosed with a single primary cutaneous melanoma are at increased risk of developing multiple primary melanomas. The aim of this study is to describe the epidemiology of multiple primary melanomas (invasive and in situ) in Western Sweden. Data from the Swedish Melanoma Registry from 1990 to 2013 revealed that 898 patients (7.4%) developed 2,037 multiple primary lesions and 11,254 patients developed single lesions. The proportion of subsequent lesions that were melanoma in situ was 47%, compared with 26% of first melanomas (p < 0.0001).The median and mean time to diagnosis of a subsequent melanoma was 38 and 58 months (95% confidence interval (CI), 53–62 months). In total, 49% of subsequent melanomas were detected within 3 years. Patients and physicians should be aware of the high proportion of multiple primary melanomas in Western Sweden, especially during the first years of follow-up.
Key words: cutaneous malignant melanoma; multiple primary melanomas; second primary melanoma; synchronous melanomas; subsequent melanomas; time to diagnosis.
Accepted Dec 12, 2016; Epub ahead of print Dec 13, 2016
Acta Derm Venereol 2017; 97: XX–XX.
Corr: Magdalena Claeson, Department of Dermatology and Venereology, Sahlgrenska Academy, SE-413 45 Gothenburg, Sweden. E-mail: magdalena.claeson@vgregion.se
Incidence rates of cutaneous malignant melanoma (melanoma) are increasing worldwide in the fair-skinned population (1). Early detection and increased survival have resulted in a high proportion of melanoma survivors. It is well known that patients diagnosed with a single primary melanoma are at elevated risk of developing multiple primary melanomas during their lifetime. Multiple lesions can be detected synchronously at a single visit or during follow-up (i.e. subsequent melanomas). Important risk factors for developing multiple primary tumours are: age, fair skin type, family history of melanoma and presence of many or large naevi (2, 3). Research has shown that the percentage of patients who develop multiple primaries ranges from 0.2% to 8.6% (4, 5). Subsequent melanomas in patients who attend follow-up have been noted to present with a thinner Breslow thickness than those who do not attend follow-up (6, 7). Previous studies have also calculated the latency of development of subsequent melanomas; they are most common within the first years after initial diagnosis (2, 4, 5, 8, 9).
Sweden is among the countries with the highest incidence of melanoma in the world. The incidence increases annually, by 5.5% for men and 5.2% for women and is currently 19.5 for men and 20.9 for women/100,000 population (World Standard Population year 2000) (10, 11). The increasing incidence makes melanoma a major health issue, being the 6th leading cancer in the country for men and the 5th leading cancer for women. Despite increasing incidence, the national mortality rate has remained low, at 2.8 deaths/100,000 population (World Standard Population year 2000) (10). Thus, Sweden has a high proportion of patients diagnosed with a single primary melanoma at risk of developing multiple primary melanomas. There are a few previous studies investigating different aspects of multiple primary melanomas in Sweden, but none has focused on Western Sweden (12–15). Over the past 20 years this geographical region has shown a higher incidence of melanoma than the national average, and is therefore an important area for melanoma research (16).
The aim of this study was to describe multiple primary melanomas (both invasive and in situ) in Western Sweden from 1990 to 2013, focussing on the number of lesions detected, patient and tumour characteristics, and the time to diagnosis of a subsequent melanoma.
Data were extracted retrospectively from the Swedish Melanoma Registry. The data-set provided information on all invasive and in situ melanoma cases in Western Sweden from January 1, 1990 to December 31, 2013. Western Sweden is a geographical area with approximately 1.6 million inhabitants, corresponding to 17% of the national population (17).
All patients identified as having had one or more invasive or in situ melanomas were eligible for analysis. Data on patient characteristics, such as age and sex, were obtained, as well as tumour characteristics, such as invasion depth of the first and any subsequent melanoma. The invasion depth categorized the melanomas depending on their Breslow thickness: Tis (melanoma in situ), T1 (≤ 1.0 mm), T2 (1.01–2.0 mm), T3 (2.01–4.0 mm), T4 (> 4.0 mm), and unknown thickness. In addition, the melanomas were characterized according to their histopathological subtypes: nodular melanoma (NM), superficial spreading melanoma (SSM), lentigo maligna melanoma (LMM), acrolentiginous melanoma (ALM), and other. Time to diagnosis was calculated, defined as the time from diagnosis of a first melanoma to diagnosis of a subsequent melanoma. Some of the multiple primaries in the registry were diagnosed within a relatively short time after the first melanoma, indicating that they were detected within the care pathway of the first melanoma. Thus, synchronous melanomas were defined as 2 or more melanomas diagnosed within 3 months. Recent studies on multiple primary melanomas have used this definition to avoid underestimating the time to diagnosis of a subsequent melanoma (2, 6, 18). When there were synchronous lesions, the thickest melanomas in the first period of 3 months were selected for comparison with the thickest melanomas in the subsequent 3 months.
All data were analysed using R version 3.0.3 (The R Foundation for Statistical Computing, Vienna, Austria). Kaplan-Meier estimates were calculated for the 5-year and 10-year probability of developing a subsequent melanoma. Wilcoxon rank-sum test was used for 2-sample comparisons. Wilcoxon signed-rank test was used for paired tests. The exact binomial test was used as a pairwise sign-test. Fisher’s exact test was used to compare proportions. Univariate Cox proportional hazards tests were performed to test for dependence between the time from the first to the subsequent melanoma vs. sex, age and whether the first melanoma was invasive or in situ. All tests were 2-sided and p < 0.05 was considered statistically significant. The regional ethics board approved the data extraction.
Within the 24 years of the study period, 12,152 patients developed 13,291 melanomas (in situ and invasive) in Western Sweden. Out of all patients, 5,922 (49%) were men and 6,230 (51%) were women. The median Breslow thickness for all invasive melanomas was 0.90 mm (0.93 mm for men and 0.80 mm for women, respectively).
Of all patients in the registry, 11,254 developed only a single primary melanoma, whereas 898 (486 men, 412 women) developed multiple primaries. Hence, 7.4% of the patients in this cohort developed multiple tumours during the study period. There was no significant increase (p = 0.57) in the proportion of patients developing multiple tumours comparing the time periods of 1990 to 1994 (8.2%) and 2000 to 2004 (7.7%). The patients with multiple primaries developed a total of 2,037 melanomas (1,122 for men and 915 for women). This corresponds to a mean of 2.3 melanomas per patient in this cohort. Most patients with multiple tumours (n = 729, 81%) developed only 2 melanomas, but patients with 3 or 4 melanomas were not uncommon, corresponding to 126 (14%) and 30 (3%) patients, respectively. One patient in the registry was diagnosed with a total of 16 separate melanomas within the study period.
The median and mean age of the patients with multiple lesions at diagnosis of the first melanoma was 67 and 66 years for men (95% confidence interval (CI) 65–67) and 64 and 61 years for women (95% CI 60–63) (p < 0.001). Table I describes the tumour characteristics of the multiple primary melanomas. Table II shows 5-year and 10-year estimates for the probability of developing a subsequent melanoma. A univariate Cox proportional hazards model analysis showed men to be at considerably higher risk of developing a subsequent melanoma compared with females, with a hazard ratio (HR) of 1.37 (95% CI 1.15–1.60, p = 0.005). Comparing patients who had a melanoma in situ as their first melanoma with those who had an invasive melanoma as their first melanoma yielded a HR of 1.24 (95% CI 0.96–1.51) for developing a subsequent melanoma, but this was not significant (p = 0.13). The age at which patients with multiple primary melanomas were diagnosed with their first melanoma did not influence the risk of a subsequent melanoma (HR 1.0, 95% CI 0.99–1.01, p = 1).
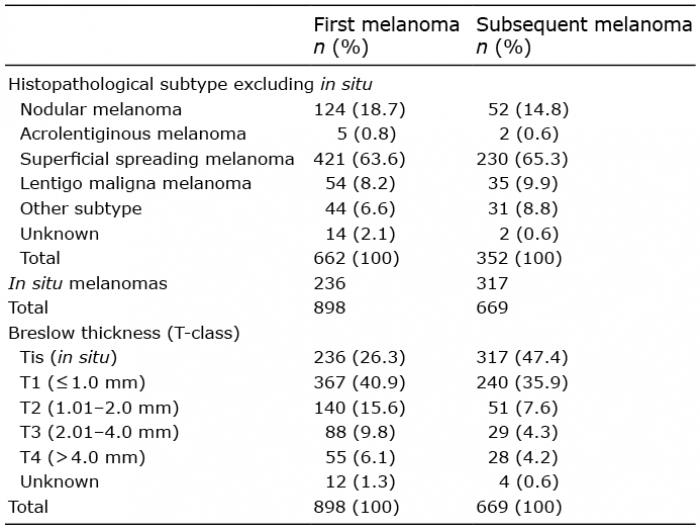
Table I. Tumour characteristics of the multiple primary melanomas in Western Sweden during 1990 to 2013 (excluding synchronous tumours)
Table II. Cumulative probability of a subsequent melanoma among patients diagnosed with their first melanoma during 1990 to 2003 in Western Sweden. (No censoring with respect to death or migration was possible)
Analysis of the distribution of multiple primary melanomas with respect to their Breslow thickness showed that a greater proportion of subsequent lesions were melanoma in situ (47%) compared with first melanomas (26%, p < 0.0001). In the Western Sweden cohort, 656 patients had proper registrations regarding Breslow thickness both for their first and their subsequent melanoma. Out of these patients, 266 developed invasive melanomas in both the first and the subsequent case. Thinner subsequent lesions were registered in 144 patients (54%), whereas thicker subsequent lesions were registered in 115 patients (43%) and 7 patients (3%) had equally thick first and subsequent invasive melanomas. Of the 390 patients with at least one in situ melanoma, 214 (55%) developed an invasive melanoma first followed by a subsequent in situ melanoma, whereas 79 (20%) developed an in situ melanoma first, followed by an invasive melanoma and 97 (25%) developed an in situ melanoma first followed by another in situ melanoma.
The Breslow thicknesses of all the first and subsequent invasive melanomas are shown in Fig. 1. The median Breslow thickness for the first invasive melanoma was 0.90 mm and the mean was 1.58 mm (95% CI 1.43–1.74).
Fig. 1. Breslow thickness (mm) of the first and the subsequent melanomas.
The median Breslow thickness for the subsequent invasive melanoma was 0.70 mm and the mean was 1.63 mm (95% CI 1.29–1.96). The median and mean difference in Breslow thickness between the subsequent and the first invasive melanomas was –0.1 and 0.05 (95% CI –0.32 to 0.42, p = 0.052), respectively.
The time to diagnosis of a subsequent melanoma is plotted in Fig. 2. Of the patients with multiple lesions, 143 (21%), 116 (17%) and 67 (10%) had a subsequent melanoma within the first, second and third year, respectively (excluding synchronous melanomas). Only 3% of the patients with multiple primaries were diagnosed with a subsequent melanoma after > 15 years. Analysis also showed that the median and mean time to diagnosis was 38 and 58 months (95% CI 53–62), respectively. The interquartile range was 14–84 months.
Fig. 2. Time from diagnosis of the first melanoma to the diagnosis of the subsequent melanoma (years).
The data-set in this study provided 13,291 invasive and in situ melanomas over a period of 24 years, which is a large cohort and a respectable length of follow-up, compared with other studies (4, 5). The proportion of patients with multiple primary melanomas in this cohort was 7.4%, a number that is in line with that of other studies, which has ranged from 0.2% to 8.6% (4, 5). Data for comparison with the entire nation of Sweden is available in a report from the Swedish Melanoma Registry for the years 1990 to 2014 (19). The report covers approximately the same period as this study and showed a proportion of multiple primary melanomas of 4.2%. This lower percentage may be explained by the fact that only invasive melanomas were included in the report. Another study by Chen et al. (14), based on data on melanoma cases from 1958 to 2010 from the Swedish Cancer Registry, showed a proportion of multiple primary melanomas of 5.5%. Interestingly, the study included both invasive and in situ melanomas, but still showed a lower proportion of multiple primary melanomas. One possible explanation for the difference could be that Western Sweden had a higher incidence of in situ melanomas, with an age-standardized rate (Swedish population year 2000) of 32 × 10–5 in 2013 compared with 22 × 10–5 in the nation as a whole (19). We believe the inclusion of in situ lesions to be a strength of this study, since they represent a high proportion of the total number of melanomas (32% in the present study).
Another possible explanation for the relatively high proportion of multiple primary melanomas in the present study is the above-mentioned length of follow-up in the registry, since age is a risk factor for developing melanomas. Also, the accuracy and high completion of the Swedish Melanoma Registry could be a further explanation. The Swedish Melanoma Registry has compulsory reporting from both clinicians and pathologists, ensuring that the coverage in the Western Sweden healthcare region is 99% for invasive melanoma and 92% for melanoma in situ (20). One weakness of the study was that we could not control for missing cases of multiple primaries in the registry, depending on patient migration to or from the region. Furthermore, with the data available we could not censor for death or migration in the 5- and 10-year Kaplan–Meier estimates, which may have led to an underestimation of the development of subsequent melanomas.
In this study, SSM, NM and LMM were, in decreasing order, the most common histopathological subtypes among first and subsequent melanomas. One patient in the registry was diagnosed with a total of 16 separate melanomas, which is an extraordinarily high number. However, one case of as many as 48 melanomas in the same patient has been reported in the literature (8).
Most previous studies have shown a reduction in tumour thickness for subsequent invasive melanomas (2, 9, 21). In our study, the median tumour thickness in subsequent melanomas was reduced, but statistical significance was not reached (p = 0.052). However, we did find a significantly increased proportion of melanoma in situ among subsequent melanomas. Similar observations have been confirmed earlier (2, 9). Ferrone et al. (4) reported a proportion of melanoma in situ of 21%, 50%, 55% and 70% for the first, second, third and fourth subsequent melanomas, respectively.
Most countries, including Sweden, base their follow-up routines on observed recurrence rates for patients, depending on prognostic factors such as Breslow thickness, the presence of ulceration, and the presence of mitosis in thin melanomas (T-class) and the N- and M-stage (lymph node involvement and distant metastasis, respectively). However, the risk of subsequent melanomas is usually disregarded. The Swedish national guidelines for melanoma treatment recommend no periodic follow-up for stage 0 and IA melanomas. Three years of follow-up is recommended for stage IB, II and III melanomas (22). In our cohort, the median time to diagnosis for the subsequent melanoma was 38 months (3 years and 2 months). The analysis of time to diagnosis showed that 21%, 49% and 63% of patients developed their subsequent melanomas within 1, 3 and 5 years, respectively. However, the analysis was performed excluding synchronous melanomas. The inclusion of these would have resulted in an even higher percentage of subsequent melanomas during the first years after initial diagnosis. According to the HRs for developing a subsequent melanoma, it does not seem necessary to take age at diagnosis into consideration. Furthermore, the registration of the first tumour as being invasive or in situ does not seem to impact the T-classification of a subsequent tumour. Interestingly, the calculations suggest that men could benefit from closer surveillance, since they have a higher hazard of developing a subsequent tumour. In addition, our results regarding time to diagnosis suggest that only half of the subsequent melanomas in Western Sweden would be detected within the present follow-up programme.
It is well known that early detection of single primary melanomas is essential for the prognosis. Similarly, patients with multiple lesions would probably benefit from early diagnosis of subsequent melanomas. Moreover, new treatments for metastasized melanoma disease have been developed during the last years (23). This will possibly lead to an updated emphasis on early detection of metastases in the follow-up programmes for patients with melanomas. Evidence encouraging regular follow-up, from studies by McGuire et al. (24) and Garbe et al. (25), reported that physicians rather than patients detected subsequent melanomas, as opposed to single primary melanomas. On the other hand, the regular full-body skin examination during follow-up may lead to a surveillance bias of the physician, resulting in a higher frequency of melanoma detection. Correspondingly, one may speculate that the pathologist could be biased to overdiagnosis in patients with melanoma in the medical history. The economic impact on health resources from extensive follow-up routines also has to be considered. Turner et al. (26), used computer modelling to investigate the effects of a less intensive monitoring schedule. Their results showed only a small difference in diagnosis delay using a follow-up routine with fewer visits. Recently, the Swedish national guidelines for melanoma treatment have changed, moving towards a considerably lower number of follow-up visits (27, 28). More research is needed in the area of follow-up for melanoma patients.
We conclude that as many as 7.4% of the melanoma patients in Western Sweden developed subsequent melanomas during 1990 to 2013. Subsequent melanomas presented with a higher proportion of melanoma in situ. After initial diagnosis, approximately half of the subsequent melanomas were detected during the first 3 years. Patients, as well as physicians, should be aware of the high proportion of multiple primary melanomas in Western Sweden, especially during the first years of follow-up.
The authors thank Leyla Núñez, and Erik Bülow, statisticians at the Regional Cancer Centre Western Sweden, for extraction of the data from the Swedish Melanoma Registry. The federal government supported this study under the ALF-agreement.


 Click to show fullsize
Click to show fullsize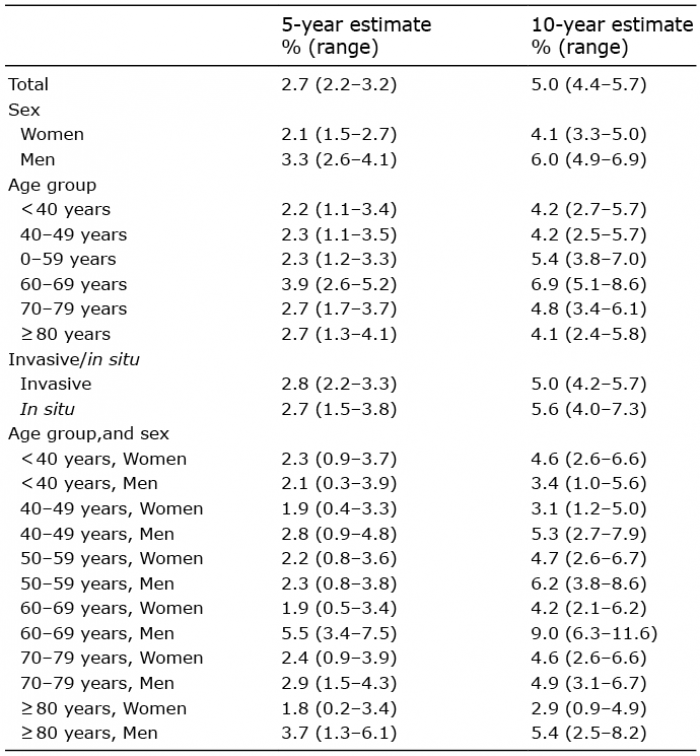 Click to show fullsize
Click to show fullsize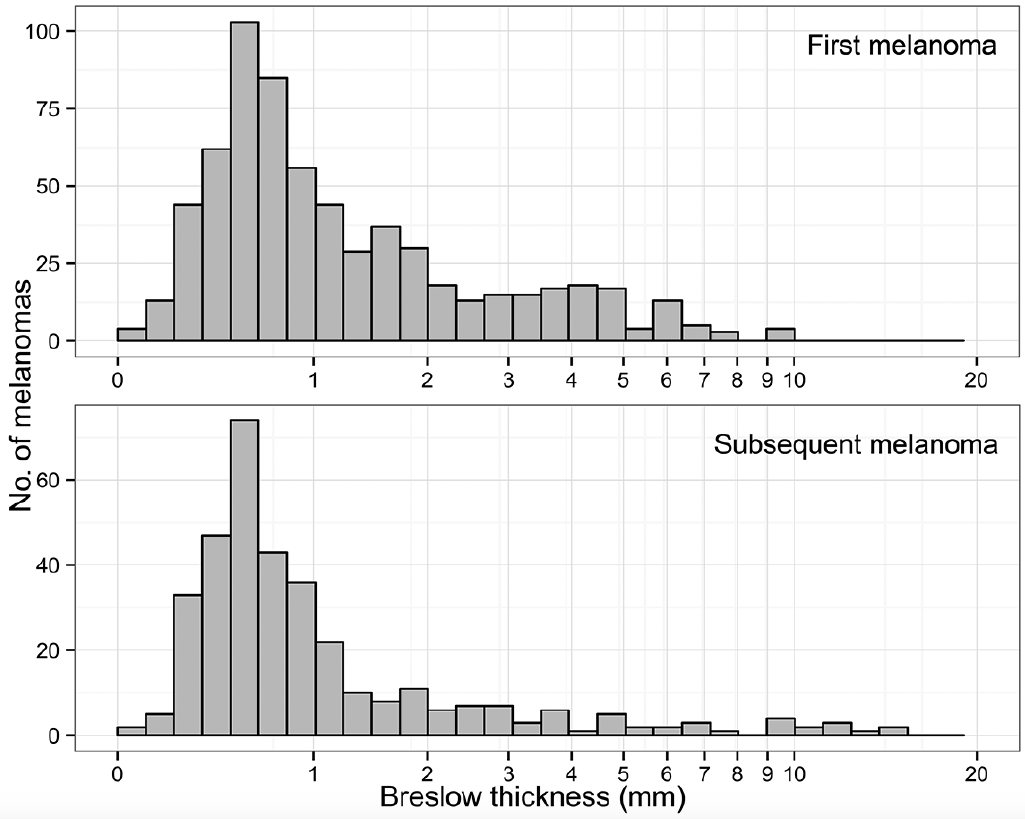 Click to show fullsize
Click to show fullsize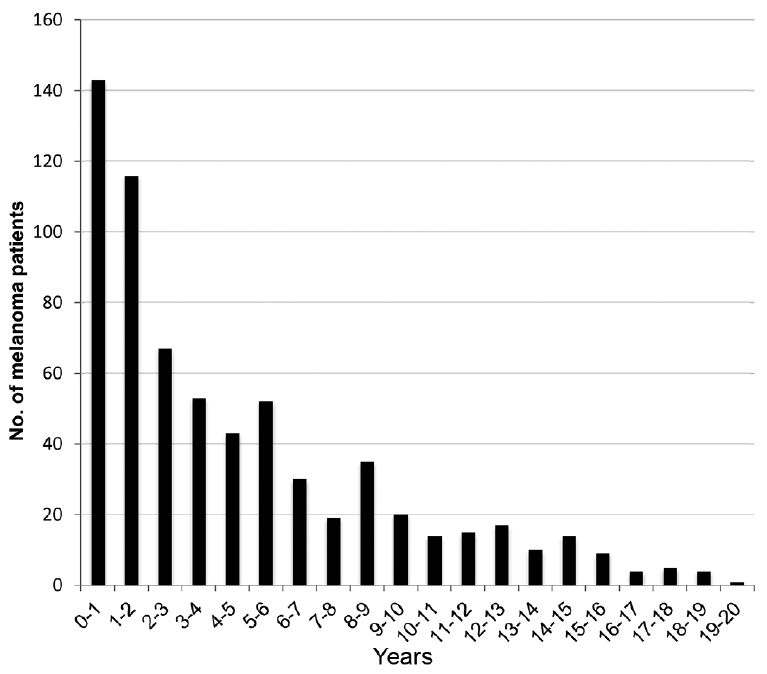 Click to show fullsize
Click to show fullsize