


1Department of Dermatology and Allergology, Tampere University Hospital, PO Box 2000, FIN-33521 Tampere, 2University of Tampere and Fimlab Laboratories, and ³Department of Internal Medicine, Tampere University Hospital, Tampere, Finland. E-mail: teija.kimpimaki@elisanet.fi
Accepted Jan 12, 2017; Epub ahead of print Jan 17, 2017
Foot and leg ulcers are a common disorder. It has been estimated that 0.12–1.1% of the population have ulceration of this kind (1). Vasculitic ulcers have been reported to account for 5–15% of all leg ulcers (2–4). The diagnosis of vasculitic ulcer is a challenge, however, as the diagnostic histological features are detectable only in recent skin lesions not older than 48 h (5). Cutaneous small vessel vasculitis generally affects blood vessels in the superficial dermis. Vasculitis of the medium or large vessels occurs deeper in the dermis or even in subcutaneous tissue (6). Thus, a skin biopsy from an adequate depth is crucial for the correct diagnosis of vasculitic ulcer. In addition to a histological assessment of the skin sample, the accurate diagnosis of vasculitic skin ulcer requires the exclusion of systemic vasculitis (5, 7, 8).
Vasculitic ulcers are typically painful and often require a long period of treatment. The ulcer may heal and the patient may recover in a few weeks. However, in the most difficult cases the ulceration may continue for years and several relapses may occur (9, 10). Since there are only limited data on the epidemiology of cutaneous vasculitic ulcers, this study evaluated the incidence of this disease in Pirkanmaa County, Finland, over the period 1980–2010.
This retrospective study was based on a cohort of patients aged at least 17 years who were treated for cutaneous vasculitic ulcers at the Department of Dermatology, Tampere University Hospital, in 1980–2010. They were all living in Pirkanmaa County at the time. The treatment of dermatological patients from the county has been centralized in the University Hospital. Population data for Pirkanmaa County were obtained from the Finnish Population Register Centre. The total population aged at least 17 years in the district served by Tampere University Hospital was 316,505 in 1980 and 395,300 in 2010.
Patient data were retrieved from the Tampere University Hospital patient data system using International Classification of Disease (ICD) codes. The case histories of a total of 1,327 patients were evaluated. Patients with cutaneous symptoms associated with systemic vasculitis were excluded. Data from histological and direct immunofluorescence examinations of the patient’s skin biopsy were recorded, as stated in the dermatopathologist’s report. The results of assays for antineutrophil cytoplasmic antibodies (ANCA), cryoglobulins and phospholipid antibodies were recorded. Ulcer was defined as vasculitic ulcer if the dermatopathologist had stated that histological criteria for cutaneous vasculitic ulcer were fulfilled, or it was stated in the case history that the diagnosis of vasculitic ulcer had been made based on typical clinical findings. Approval from the ethics committee was not considered obligatory, because the study was based on case records, and due permission was obtained for reading these.
The data were analysed statistically using STATA 13.1 and SPSS software (SPSS 19.0 Inc. Chigaco, IL, USA). Annual incidences of vasculitic ulcers were calculated using Poisson regression analysis (11). Incidence rate ratios with 95% confidence intervals (CI) were calculated to assess annual variations in the incidence of vasculitic ulcers.
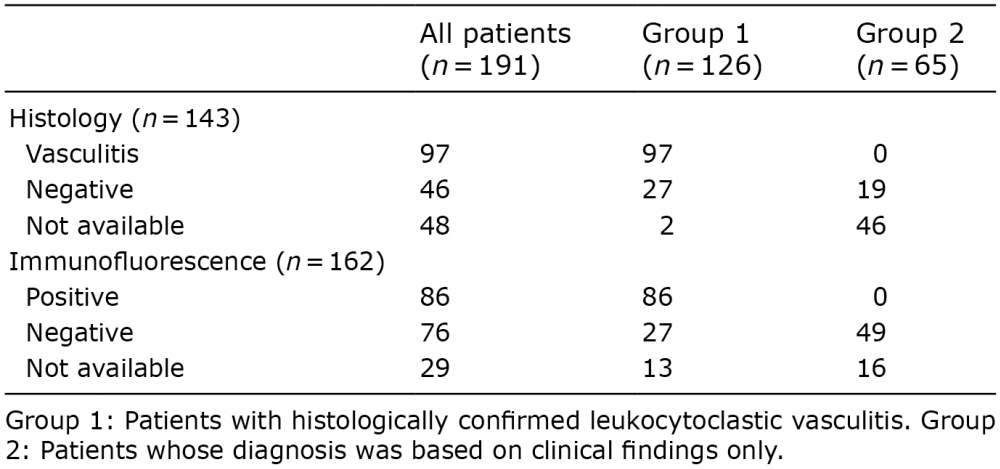
A total of 191 patients (age range 18–95 years, median age 66 (SD 17.1) years, 73 men) presenting for the first time and receiving treatment for cutaneous vasculitic ulcer at the Department of Dermatology from January 1980 to December 2010 were identified. A skin biopsy for histological examination had been obtained from 143 of the 191 patients (74.9%) and from 162 (84.8%) for analysis by direct immunofluorescence assay (DIF). Altogether, 126 patients (66.0%) had histologically confirmed leukocytoclastic vasculitis (Group 1, Table I) and the remaining 65 patients had been diagnosed on clinical findings without histological confirmation (Group 2). DIF was diagnostic in 86 of 191 patients (45.0%). The incidence of vasculitic ulcers in these groups was assessed separately.
Table I. Histopathological findings in 191 patients with cutaneous vasculitic ulcers
Nineteen patients tested positive for perinuclear anti-neutrophil cytoplasmic antibodies (P-ANCA) and 2 for cytoplasmic anti-neutrophil cytoplasmic antibodies (C-ANCA), all without any specific definition. The titres were low in all the patients who tested positive for cryoglobulins (n = 2) or phospholipid antibodies (n = 8) and the clinical significance of these remained uncertain.
The incidence of leukocytoclastic vasculitic ulcers among all the patients in 2010 was 45.5/106 person years (30.4/106 person years for Group 1 and 39.5/106 person years for Group 2). The incidence of cutaneous vasculitic ulcers increased over the period 1980–2010. The incidence rate ratio (IRR) was 1.07 (95% CI 1.05–1.09, p < 0.001) among all the patients. In Group 1 the IRR was 1.06 (95% CI 1.04–1.09, p < 0.001), and in Group 2 IRR was 1.09 (95% CI 1.06–1.13).
The mean age of the total population had increased from 44.8 years in 1980–1990 to 47.6 years in 2001–2010, but that of the vasculitic ulcer patients was significantly higher (mean 66.1 years; CI 62.8–69.4 years) in 2001–2010 than in either 1980–1990 (mean 50.7 years; CI 42.3–59.2 years) or 1991–2000 (mean 62.3 years; CI 58.7–65.8 years; p < 0.001).
This report shows that the annual incidence of cutaneous leukocytoclastic vasculitic ulcers among the adult population of Pirkanmaa County, Finland, in 2010 was 45.5/106. The IRR was 1.07 over the period 1980–2010, representing a 7% annual increase in the incidence of vasculitic ulcers. The incidence of histologically confirmed leukocytoclastic vasculitis was similarly increased (IRR 1.06) reaching a level of 30.4/106. Our finding of an increase in the incidence of cutaneous vasculitis is supported by the recent observation of a comparable incidence rate for biopsy-proven cutaneous small vessel vasculitis of 21/106 person years in a retrospective population-based study performed in Minnesota, USA (12).
We also found that the mean age of patients diagnosed as having vasculitic ulcers increased more steeply over the interval 1980–2010 than did the mean age of the total population concerned (15.4 years vs. 2.8 years). Ageing of the population may, however, somewhat explain the increased incidence of vasculitic ulcers during the last three decades. There may also be other factors, e.g. medication or infections, that could not be evaluated reliably in this retrospective study.
There are some limitations attached to this work. Certain clinical data may be incomplete, as the material was collected retrospectively. On the other hand, the observation period was quite long, as the data covered the interval from 1980 to 2010. In common with its names and definitions, the diagnostic criteria for vasculitic ulcer have altered over the period 1980–2010, and this may have influenced the incidence rates in the reports covering the period before 1994, particularly those reported before 1994, when cutaneous leukocytoclastic vasculitis was defined as isolated cutaneous leukocytoclastic angiitis without systemic vasculitis or glomerulonephritis (13). Therefore, cases of vasculitic ulcer with systemic disease may have been included in the previous reports concerning the incidence of cutaneous leukocytoclastic vasculitis before 1994, and its actual incidence may have been lower than was reported prior to that date. The operational environment, nevertheless, remained the same between 1980 and 2010, as did the hospital district’s referral policy.
In conclusion, these results indicate that cutaneous vasculitic ulcers are more common in Pirkanmaa County, Finland, nowadays than they were previously. We suggest that ageing of the population is the main reason for this, but prospective studies would be needed in order to examine the aetiology and pathogenesis of this disease systematically, with the ultimate objective of preventing new cases.
The authors are grateful to Heini Huhtala, MA, for her skilful statistical analyses.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize