


1Department of Dermatology, Hôpital Victor Dupouy, Argenteuil, 2Department of Public Health, Centre Hospitalier Universitaire Ambroise Paré, University of Versailles-Saint-Quentin-en-Yvelines, Assistance Publique-Hôpitaux de Paris, Boulogne-Billancourt, 3Department of Dermatology, Hôpital Robert Debré, Reims, 4Department of Dermatology, Hôpital d’Instruction des Armées Bégin, Saint-Mandé, 5Private Office, Martigues, 6Department of Dermatology, Hôpital Sud, Centre Hospitalier Universitaire d’Amiens, Picardie-Jules Verne University, Amiens, 7Department of Dermatology, Hôpital d’Instruction des Armées Percy, Clamart, 8Department of Dermatology, Centre Hospitalier Régional d’Orléans, Orléans, 9Department of Clinical Immunology and Allergy, Centre Hospitalier Lyon-Sud, Lyon, 10Private Office, Paris, 11Department of Dermatology, Centre Hospitalier d’Auxerre, Auxerre, 12Department of Dermatology, Centre Hospitalier de Pontoise, Pontoise, 13Private Office, Vienne, 14Department of Dermatology, Centre Hospitalier du Mans, Le Mans, 15Department of Dermatology, Hôpital d’Instruction des Armées Sainte Anne, Toulon, 16Department of Dermatology, Hôpital François Quesnay, Mantes-La-Jolie, 17Department of Dermatology, Hôpital Brabois, Vandœuvre-Les-Nancy, and 18Department of Dermatology, Hôpital Jacques Monod, Le Havre, France
Psoriasis has major physical, psychological, and social impacts: its management should not be restricted by individual financial considerations in Western countries as these have well-structured health systems and social/insurance coverage. We investigated if the socioeconomic characteristics of patients were associated with severity of psoriasis and access to healthcare. In a cross-sectional study, we included 903 patients with psoriasis that were consulting for the first time. We showed that low educational level was associated with severity of disease in multivariate analyses. Moreover, patients of lower class and lower educational level, with severe psoriasis, had seen fewer physicians and had less frequently received a systemic treatment. Thus, physicians need to be vigilante of patients with a low socioeconomic status. Both low socioeconomic status and less access to dermatologists are associated with clinical severity of psoriasis at a first consultation.
Key words: psoriasis; social inequalities; treatment; epidemiology.
Accepted Jan 25, 2017; Epub ahead of print Jan 27, 2017
Acta Derm Venereol 2017; 97: XX–XX.
Corr: Emmanuel Mahe, Department of Dermatology, Hôpital Victor Dupouy, FR-95100 Argenteuil, France. E-mail: emmanuel.mahe@ch-argenteuil.fr
Psoriasis is a chronic skin and articular disease that affects 2–4% of the population (1, 2). It is known to have major physical, psychological, and social impacts (2–4). Recently physical (i.e., cardiovascular, metabolic) and psychological (i.e., depression) comorbidities have been associated with psoriasis (5–8).
Topical and systemic treatments can improve clinical aspects, quality of life (QoL), and social discomfort. It has been suggested that the use of systemic treatments for severe forms of psoriasis could reduce the cardiovascular risk linked with psoriasis-associated chronic inflammation (9–14). Thus, adequate management and adherence to treatments are important. The management of psoriasis should not be restricted by individual financial considerations in most Western countries, which have well-structured health systems and offer social or insurance coverage.
Socioeconomic and demographic inequalities are major determinants of health status (15, 16). These differ from one country to another, but also within countries. Infectious diseases are probably the diseases most impacted by these inequalities because, for instance, of sanitary factors caused by socioeconomic inequalities. More recently, it has been shown that the stage of cancers is more advanced at diagnosis in populations with a low socioeconomic status (17, 18). This is also true for chronic cardiovascular and metabolic diseases, and for acute events, such as stroke or myocardial infarction (19–21). The consequences can be tremendous for the patient as the prognoses of these diseases depend on their early diagnosis.
Despite the high frequency of psoriasis, few and discordant data are evaluable on its link with socioeconomic and demographic status, on adherence to medication, severity of the disease, or access to treatments (22–25). Thus, we have investigated if the socioeconomic and demographic characteristics of patients consulting for the first time with psoriasis are associated with its severity
The “R-ens” study (“Resopso - Evaluation Nationale du parcours de Soins pour un psoriasis”) was a non-interventional, cross-sectional, multicenter study that included adults with psoriasis. R-ens was designed to evaluate the impact of the socioeconomic and demographic characteristics of the patients with the severity of psoriasis at a first consultation.
R-ens was performed in 40 French dermatology centers, which were all members of the GEM Resopso between January and November 2014. GEM Resospo (http://resopso.fr/le-gem) is a French association of dermatologists involved in the care and research of patients with psoriasis (26). The 40 centers were within universities (n = 9), general practice (n = 5), military hospitals (n = 3), and private practitioners (n = 13).
We consecutively included all adults aged ≥ 18 years who consulted for plaque psoriasis. Because we did not want to modify the ongoing management of patients, we only included patients that were visiting the investigative center for the first time. A protocol for evaluation was implemented that included collecting information on age, sex, age at onset of psoriasis, its clinical characteristics, family history (including first-degree relatives only), severity of psoriasis [Psoriasis Area Severity Index (PASI), Body Surface Area (BSA), Dermatology Life Quality Index (DLQI)], psoriasis arthritis, previous treatments for psoriasis, previous consultation to a general practitioner (GPs) and/or dermatologist, associated cardiovascular and metabolic comorbidities, hypertension, current smoking status, body-mass index (BMI), presence of diabetes and/or dyslipidemia, alcohol consumption, and any history of depression.
Severity of plaque psoriasis was graded as mild, moderate, or severe. We used 3 definitions for severity: (i) The concept of the “Rule of Tens”: mild disease was defined as body-surface area (BSA) ≤ 10, PASI ≤ 10, and DLQI ≤ 10; moderate-to-severe psoriasis was defined as BSA > 10, and/or PASI > 10, and/or DLQI >10 (27). (ii) Clinical severity focused on the PASI definition of severity: moderate-to-severe psoriasis was defined as PASI >10. (iii) Severity of psoriasis according to QoL, which focused on the DLQI definition of severity where moderate-to-severe psoriasis was defined as DLQI > 10.
Definitions of cardiovascular and metabolic comorbidities have been reported in a previous publication (26). Smokers were defined as smoking at least one cigarette per day; alcohol consumption was defined as people who drank at least one glass of alcohol per day. Depression was defined as patients that said they were consulting for depression or were receiving anti-depressive drugs.
Socioeconomic and demographic parameters were evaluated as the living environment, impact of living in a rural area, life as a couple and/or with children, occupational activity, contact with the public through an occupation, sporting activities, education level, and household income.
To identify households with low and high incomes, the cut-off value used was the French median household income, i.e., 2,300 € per month (28).
In France, dermatologists are not established in rural areas because they consider them as “medical deserts” for specialists. Thus, it was difficult to evaluate kilometric distance to a dermatological center; consequently, to represent the difficulty in receiving access to health-care, we use data on the size of towns to evaluate ease-of-access to healthcare. The French definition for a population density of a rural town is <3,000 people.
We first analyzed patients according to having or not having an occupational activity. We then separated the working activities as being “lower-” or “upper”-class activities (29). In France, lower-class activities are considered to be manual work, farmers, and employees; and upper-class activities as artisans, teachers, nurses …, heads of companies, executives, and intellectual occupations. Finally, we asked patients if they had “contact with the public” during there working activities. We also compared patients that had a working occupation with those that were unemployed, retired, or were students.
We planned to include 800 patients with plaque psoriasis, to include a representative sample of younger and older people, and to include at least 150 patients from private office. According to previous studies, performed by the GEM Resopso group, we needed a 1-year period for inclusions. Our objective was reached within 11 months and so the study was stopped at this time.
Quantitative data are expressed as means ± standard deviations (SD), qualitative data as n (%). Continuous variables were compared using Student’s t-test and proportions with the χ2 test. We evaluated 3 severity outcomes: PASI >10, DLQI >10, and moderate-to-severe psoriasis according to the “rule of tens” (27). We conducted univariate analyses on each of these. Multiple regression analyses were then conducted to evaluate the relationship between severity of psoriasis and medical and socioeconomic status. Included in the latter were variables that achieved a statistical value of p < 0.05 in the univariate analyses, for at least one of the 3 severity criteria.
Assessment of socioeconomic status showed that occupational activity, income, and educational level were linked. Thus, in the multivariate analyses, we only included educational level because income takes into account that of the household and not only that of the patient, and occupational activity was only correlated with severity of PASI. A p-value of < 0.05 was considered as being statistically significant. Statistical analyses were computed using SAS software v 9·3 (SAS Institute Inc., Cary, NC, USA).
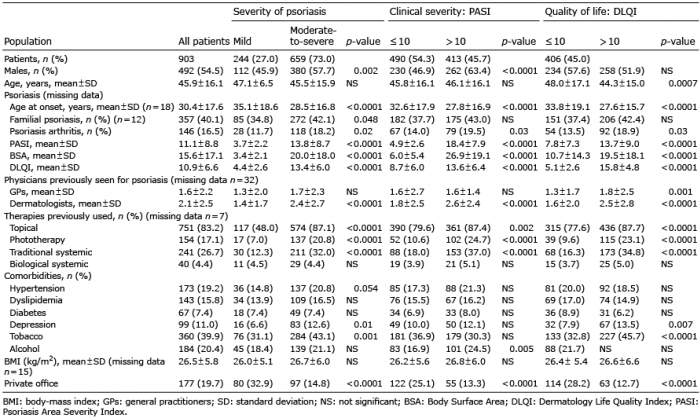
A total of 1,328 patients were included during the 11-month inclusion period. Of these, 26 were excluded because of incomplete data (age, sex) or duplicated data. Among the 1,302 patients, 926 (71.1%) had plaque psoriasis. PASI or DLQI were not evaluated in 23 cases. Thus, 903 patients with plaque psoriasis were finally included: 54.5% were males, overall mean age was 45.9 ± 16.1 years. The characteristics of psoriasis, the number of physicians seen for psoriasis, the treatments used, and the comorbidities are detailed in Table I. Severe psoriasis represented 73.0% of cases, and 45.7% and 45.0%, respectively, if only PASI or DLQI are considered. The socioeconomic and demographic characteristics are detailed in Table II.
Table I. Influence of medical data on severity of psoriasis at the first consultation in a dermatology center. Univariate analyses
Table II. Influence of socioeconomic and demographic data on severity of psoriasis at the first consultation in a dermatology center. Univariate analyses
Univariate analyses on “global” severity of psoriasis showed that severity of disease at the first consultation was associated with male sex (p = 0.002), younger age at onset of psoriasis (p < 0.0001), familial psoriasis (p = 0.048), psoriasis arthritis (p = 0.02), a higher number of dermatologists seen for the disease (p < 0.0001), and higher frequencies of local treatments, phototherapy, and traditional systemic therapies (p < 0.0001). Hypertension (p = 0.04), depression (p = 0.01), and tobacco consumption (p = 0.001) were more frequent in the moderate-to-severe group. Patients with moderate-to-severe psoriasis more frequently consulted in a hospital setting (p < 0.0001) (Table I). In the multivariate analysis, severity was associated with male sex (p = 0.001), age of onset of psoriasis (p < 0.0001), psoriasis arthritis (p = 0.04), depression (p = 0.009), and tobacco consumption (p = 0.01) (Table III).
Table III. Impact of demographic and socioeconomic data on severity of psoriasis at the first consultation in a dermatology center. Multivariate analyses
If we take “clinical” severity into account (i.e., PASI >10), in the univariate analyses, severity of the disease at the first consultation was associated with male sex (p < 0.0001), younger age at onset of psoriasis (p < 0.0001), psoriasis arthritis (p = 0.03), greater number of dermatologists seen for the disease (p < 0.0001), higher frequency of local treatments (p = 0.002), and more phototherapy and traditional systemic therapies (p < 0.0001). Alcohol consumption (p = 0.005) was more frequent in the severe group. Patients with PASI ≥10 more frequently consulted in a hospital setting (p < 0.0001) (Table I). In the multivariate analyses, severity was associated with male sex (p = 0.001), age of the patient (p = 0.036), and age at onset of the disease (p < 0.0001) (Table III).
If we take the severity of psoriasis into account, according to changes to QoL (DLQI >10), in the univariate analyses, severity of disease at the first consultation was associated with a younger age of patient (p = 0.0007), younger age at onset of psoriasis (p < 0.0001), psoriasis arthritis (p = 0.03), higher number of GPS (p = 0.001), number of dermatologists seen (p < 0.0001), and high-er frequency of local treatments, phototherapy, and traditional systemic therapies (p < 0.0001). Depression (p = 0.007) and tobacco consumption (p < 0.0001) were more frequently associated with the moderate-to-severe group. Patients with DLQI >10 more frequently consulted in a hospital setting (p < 0.0001) (Table I). In the multivariate analysis, severity was associated with age of onset (p < 0.0001), depression (p = 0.026), and tobacco consumption (p = 0.005) (Table III).
Whatever the severity score obtained, there was no association between severity and the use of biological therapies, diabetes, dyslipidemia, or BMI (Table I).
If we take “global” severity of psoriasis into account, in the univariate analyses, severity of psoriasis at the first consultation was associated with a lower education level (p = 0.005) and a lower household income (p = 0.04) (Table II). In the multivariate analyses, severity was associated with a lower educational level (p = 0.02) (Table III).
If we take “clinical” severity of psoriasis into account, in the univariate analyses, severity of psoriasis at the first consultation was associated with lower working class (p = 0.02), a lower education level (p = 0.0001), and a lower household income (p = 0.01) (Table II). In the multivariate analyses, severity was associated with a lower educational level (p = 0.004) (Table III).
If we take severity of psoriasis into account according to changes to QoL, in the univariate analyses, severity of disease at the first consultation was associated with contact with the public in occupational activity (p < 0.0001) (Table II). In the multivariate analyses, severity was not associated with educational level (Table III).
Whatever the severity score obtained, there was no impact of living in a rural area, familial structure, or reimbursement system on the severity of disease (Table II).
Among patients with clinically severe psoriasis, patients with a lower household income and educational level had seen fewer dermatologists (p ≤ 0.0001), and fewer patients had received a systemic therapy (p = 0.01 for household income, p = 0.1 for educational level) (Table IV). In these two groups, duration of psoriasis and PASI were not statistically associated (data not shown).
Table IV. Impact of household income and educational level on access to treatments and physicians, among patients with clinically severe psoriasis (PASI >10)
During an 11-month period, in 40 French centers, we evaluated the association of socioeconomic and demographic characteristics with severity of psoriasis among 903 patients consulting for the first time for plaque psoriasis. We show that low educational level, low household income, and a lower-class type of work were associated with severity of psoriasis at the first consultation. Moreover, patients of lower class with severe psoriasis had seen fewer physicians and had received less systemic treatments.
The assessment of the severity of psoriasis is debated: do we need to evaluate immediate severity (PASI, DLQI, BSA), clinical aspects, QoL, lifelong severity, impact of the disease on social activities, use of treatments, or not …?
(30) Herein we chose to evaluate clinical severity and impact of QoL on the day of a first consultation, independently of the treatments received. We have shown that demographic and socio-economic characteristics were associated with severity according to the score obtained. If we evaluated differences in clinical severity, there was an important role for socioeconomic factors; if we evaluated differences in QoL, there was an important role for depression and addiction; if we evaluated both together, both criteria were identified.
In the field of dermatology, infectious diseases, such as scabies, tinea, leprosy, can affect everybody but are clearly linked to promiscuity and socioeconomic status (31, 32). Many evaluations have been performed to evaluate the impact of socioeconomic status on the severity of some skin diseases: information has been mainly derived from oncology. For instance, in a German study, the vertical depth of invasion of basal cell carcinomas depended of the type of health insurance, which was lowest in urban areas (33). For melanoma, there is a deprivation gradient for patients according to melanoma stage: the most deprived patients have a higher probability of having advanced-stage cancer at diagnosis (18, 34). In chronic inflammatory diseases, such as lupus or systemic sclerosis, the same evidence has been reported: lower socioeconomic status is associated with a worse prognosis (35, 36).
Two major explanations are proposed: a delay in consultation and lower adherence to treatments. Conversely, atopic diseases seem to be more frequent in higher socioeconomic populations (37–39), but adherence to treatments is altered by low socioeconomic status (23–25). Herein we have shown that patients with psoriasis have the same socioeconomic inequalities as those with various other skin and non-skin-related diseases. Socioeconomic status is mainly correlated with clinical severity of the disease and not alteration to QoL at a first consultation.
In another French study, among 142 psoriatic patients, occupation, education, and monthly income were not associated with a delay in systemic treatment as assessed by the patients (22). We did not confirm this result. Herein, even though education level was not associated with access to a systemic treatment, income was, although this difference was not statistically important. In the first study on this topic (22), population size was relatively small, and thus was probably not statically powerful. French social security protects 95% of the French population, but incompletely. Complete medical coverage needs complementary private insurance, which can be a limitation for those of lower socioeconomic status.
Unlike cancer, lupus, or psoriasis arthritis, for instance, we have no proof that the clinical outcome of psoriasis is influenced by the early management of this disease, nor by skin evolution, nor the frequency of psoriasis arthritis (26, 40). However, recent data show that psoriasis is associated with several co-morbidities including an increased risk of cardiovascular diseases, probably caused by the inflammatory load over time (5–8). This increased risk can be reduced, at least partly, if psoriasis receives systemic treatment, such as methotrexate or a biological treatment (9–14). In our study, access to a dermatologist and receipt of a systemic therapy in moderate-to-severe psoriasis were linked to income.
Finally, we know that familial, professional, social, and moral aspects are impacted by severe disfiguring forms of psoriasis, which increase with the clinical severity of this disease (40). The social stigma of psoriasis can be devastating for patients (41, 42). Thus, social difficulties increase the delay in psoriasis management, and this delay can, by itself, increase social stigma (42). Consequently, dermatologists need to break this vicious circle.
In real-life practice, we need to be very vigilante of patients with a low socioeconomic status. Both low socioeconomic status and less access to dermatologists and to general treatments are associated with the clinical severity of psoriasis at a first consultation. These factors directly impact on the burden of this disease, and moderate-to-severe psoriasis may also increase the risk of cardiovascular and metabolic complications.
The authors would like to acknowledge Drs Martine Avenel-Audran (Angers), Dominique Barthelme (Pau), Marie Bastien (Joinville-le-Pont), Danielle Bouilly-Auvray (Dijon), Ali Dadban (Amiens), Jean-Noël Dauendorffer (Paris), Suzanne Devaux (Bayonne), Germaine Gabison (Saint-Maurice), Gwendeline Géner (Brunoy), Juliette Jégou (Chalons-en-Champagne), Mathilde Kemula (Charenton-Le-Pont), Bruno Labeille (Saint-Etienne), Morad Lahfa (Toulouse), Cristina Livideanu (Toulouse), Elisabeth Lorier (Paris), Hervé Maillard (Le Mans), Valérie Pallure (Perpignan), Christine Pauwels (Saint-Germain-en-Laye), Jean-Luc Perrot (Saint-Etienne), Pierre Pfister (Paris), Nathalie Quiles-Tsimaratos (Marseilles), Mahtab Samimi (Tours), Domitille Thomas-Beaulieu (Saint-Germain-en-Laye), Annie Vermersch (Valenciennes), Laurent Wagner (Paris), and Michèle Zeitoun (Antony) for their kind collaboration.
Disclosures: EM is a consultant for Novartis, Abbvie, Pfizer, Janssen Cilag, has been an investigator for Leo Pharma, Amgen, Astra Zeneca, Abbvie, Novartis, and Pfizer, and has received speaker honoraria from Abbvie, Janssen Cilag, Novartis, and Pfizer. ZR is a consultant for Janssen and Pfizer; has been an investigator for Abbvie, Novartis, and Pfizer; has received speaker honoraria from Abbvie, Janssen Cilag, and Pfizer, and Schering-Plough. FM is a consultant for Janssen; and has received speaker honoraria from Abbvie, Janssen Cilag, Leo Pharma, and MSD. GC is a consultant for Janssen; and has received speaker honoraria from Abbvie, Leo Pharma, and Pfizer. TLG has received speaker honoraria from Novartis and Janssen Cilag. EE has received speaker honoraria from Abbvie, Janssen Cilag, Leo Pharma, Pfizer, and MSD. CG-H is a consultant for Abbvie. HB is a consultant for Abbvie, Janssen Cilag, Leo Pharma, MSD, and Pfizer; and has received speaker honoraria from Abbvie, Janssen Cilag, Leo Pharma, MSD, and Pfizer. EB has received speaker honoraria from Abbvie, Janssen Cilag, Leo Pharma, MSD, and Pfizer. NB has been an investigator for Pfizer, and Novartis; is a consultant for Janssen Cilag; and has received speaker honoraria from Janssen. TB has received speaker honoraria from Abbvie and Janssen. LM-B has received speaker honoraria from Abbvie, Pfizer, and Leo Pharma. J-LS has been an investigator for Pfizer. PB has been an investigator for Abbvie; and has received speaker honoraria from Abbvie, Janssen Cilag, and Pfizer. The other authors declare no conflict of interest.


 Click to show fullsize
Click to show fullsize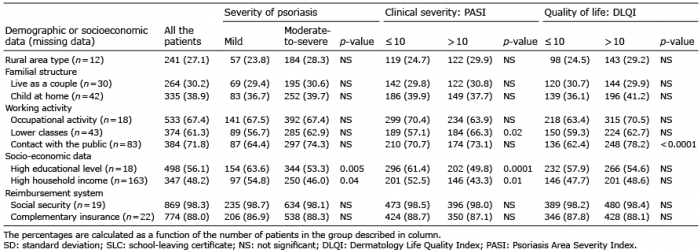 Click to show fullsize
Click to show fullsize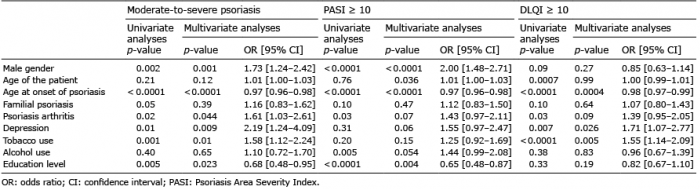 Click to show fullsize
Click to show fullsize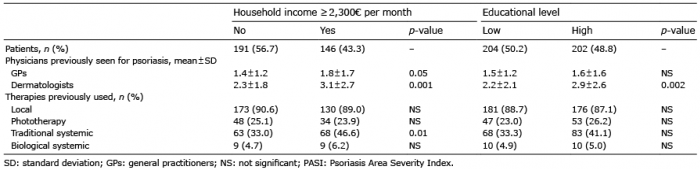 Click to show fullsize
Click to show fullsize