


1Department of Dermatology, Venereology and Allergology, and 2Department of Pathomorphology, Wroclaw Medical University, Chalubinskiego 1, 50-368, Wroclaw, Poland. *E-mail: wojciech.baran@umed.wroc.pl
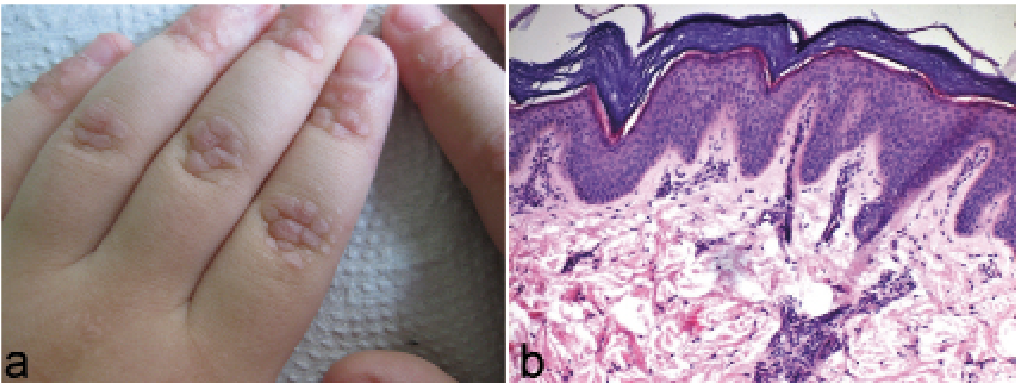
A 4-year-old Caucasian boy with non-consanguineous parents was admitted to the Department of Dermatology for evaluation of asymptomatic keratotic papules on the dorsal aspects of both hands (Fig. 1a). The lesions had developed 2 years prior to hospitalization and had gradually increased in number. Treatment with topical corticosteroids had been ineffective. There was no family history of similar lesions and the boy was otherwise healthy. No abnormalities of the hair, nail or teeth were seen on physical examination. Full blood count, routine biochemical analysis and urinalysis were within normal limits. A 4-mm punch biopsy was performed from lesional skin (Fig. 1b). Orcein staining revealed normal elastic fibres.
What is your diagnosis? See next page for answer.
Fig. 1. Clinical and histological features. (a) Multiple flesh-coloured, crateriform and confluent papules located symmetrically over metacarpo-phalangeal and interphalangeal joints. (b) Histopathological image displays orthohyperkeratosis with acanthosis, focal hypergranulosis, scarce lympho-cytic infiltrate in the dermis (haematoxylin and eosin (H&E), original magnification ×100).
Acta Derm Venereol 2017; 97: XX–XX.
Diagnosis: Focal acral hyperkeratosis
Focal acral hyperkeratosis (FAH) is a rare entity characterized by yellowish or flesh-coloured papules with a tendency to coalesce into plaques, located along the margins and on the dorsal aspects of the hands and feet. Skin lesions are usually bilateral and asymptomatic. The first papules occur in childhood or early adult life and gradually increase in number over the years (1–4).
In 1953, Brazilian dermatologist Oswaldo Costa (1) introduced the term “acrokeratoelastoidosis” (AKE) to describe palmoplantar keratoderma characterized by crateriform, keratotic papules and plaques on the borders and dorsal aspects of the hands and feet and prominent elastorrhexis in histopathology. The term “focal acral hyperkeratosis” was coined in 1983 by Dowd et al. (2), who described 15 cases with the same clinical presentation as AKE, but with no alterations in elastic fibres in histopathology.
FAH was initially considered a genodermatosis of an autosomal dominant pattern of inheritance, which occurred only in females of Arabian or Afro-Caribbean origin (1, 2). In 1994, the first 2 cases in Caucasian patients were described (3). An increasing number of sporadic cases have been published recently (3–9).
FAH is thought to be a focal keratinization disorder with accelerated proliferation and differentiation of lesional keratinocytes (4). Histopathologically, it is characterized by orthohyperkeratosis, hypergranulosis and normal dermis with no evidence of elastorrhexis, which is the only feature differentiating it from AKE (1, 2, 5). The cause of increased keratinization remains unknown. No association with trauma, exposure to light, topical irritants or human papilloma virus (HPV) infection has been documented in sporadic variants. Likewise, in familial cases the underlying genetic abnormalities have not yet been identified.
The nosological positions of FAH and AKE remain undetermined. Rongioletti et al. (3) included FAH in a group of “marginal papular acrokeratodermas”, consisting of 9 entities; AKE, FAH, hereditary papulotranslucent acrokeratoderma, acrokeratoelastoidosis of Matthews and Harman, mosaic acral keratosis, acrokeratoderma hereditarium punctatum, keratoelastoidosis marginalis, digital papular calcinosis and degenerative collagenous plaques of the hands. Some authors consider FAH to be a separate entity (6), while others suggest that it is a histological variant of AKE without elastrorrhexis (7). The classification became even more complicated when cases of intermediate phenotypes, lacking evident elastorrhexis, but displaying focal paucity of elastic fibres, were described (8). Nevertheless, it is noteworthy that distribution of hyperkeratotic papules in these 2 entities may differ (6), with AKE predominantly manifesting on the palms, and FAH on the borders and dorsal surfaces of the fingers, as in the reported patient (5, 9).
To date, fewer than 100 cases of FAH have been reported. To the best of our knowledge, this is the first report in the Polish population.
In the current case, viral warts and acrokeratosis verruciformis of Hopf were considered in the differential diagnosis. These entities were excluded by the absence of their histopathological hallmarks: cell vacuolization in viral warts and “church spire” configuration with dyskeratosis in acrokeratosis verruciformis of Hopf. A diagnosis of AKE was ruled out on the basis of normal appearance of elastic fibres with orcein staining.
Treatment of FAH is challenging. Management options include keratolytic agents, topical retinoids, cryotherapy or intralesional triamcinolone (7). Recent publications underscore high efficacy of systemic therapy with acitretin (5, 8). However, in our opinion, aggressive therapy should be avoided in young patients because of the benign nature and good prognosis of the condition. In the patient described here regular follow-up with no topical treatment was recommended.


 Click to show fullsize
Click to show fullsize