


Departments of Dermatology, 1Utrecht University Medical Centre, Utrecht, 2Amphia Hospital, Breda, 3Bravis Hospital, Roosendaal, and 4Leiden University Medical Centre, Postbus 9600, NL-2300 RC Leiden, The Netherlands. *E-mail: N.A.Kukutsch@lumc.nl
Accepted Mar 15, 2017; Epub ahead of print Mar 15, 2017
Naevus spilus (NS) is characterized by congenital or acquired darkly pigmented macules and papules with background hyperpigmentation. It usually presents as a single lesion, but can be multiple, and may be distributed in a zosteriform pattern along a dermatome (1). NS has also been described in association with an epidermal naevus and scoliosis (1). The prevalence of NS in the general population is estimated to be 0.2–2.3%. Frequent locations are the trunk and lower limbs (2–5). NS occur in all skin types (3). Somatic activating HRAS mutations were identified recently as the potential underlying cause of small single NS, which separates them from the congenital melanocytic naevi that show NRAS or BRAF mutations (6, 7).
Malignant transformation of a NS is rare. In 1957, Perkinson described for the first time a melanoma appearing in NS in a patient with neurofibromatosis (8). Since then, several cases have been reported of in situ melanoma developing in NS (2, 4, 5, 9–30).
This article focusses on patients with segmental NS. They can show a flag-like, block-like or chequerboard café-au-lait pattern with superimposed naevi increasing in number during childhood and adolescence (31). The prevalence of segmental NS or the incidence of melanomas occurring within the NS has not been well studied.
Patients with segmental NS >20 cm were collected from the database (January 2004 to December 2015) of the department of dermatology, Leiden University Medical Centre, the Netherlands. Clinical records were reviewed for initial presentation, changes during follow-up and results of biopsies or excisions. Photographic documentation was observed. Patients with NS-type congenital naevi, which were described recently as a specific subtype of congenital naevi were excluded (32). A review of the literature (PubMed search 1936–September 2015, Search ((((((“nevus spilous”) OR “naevus spilous”) OR “naevus spilus”) OR “nevus spilus”) OR “zosteriform lentiginous nevus”) OR “speckled lentiginous nevus”) was performed.
RESULTS
Five patients with segmental NS > 20 cm were included; 2 men and 3 women with a mean age of 45.8 years at first follow-up (Table SI and Fig. 1).
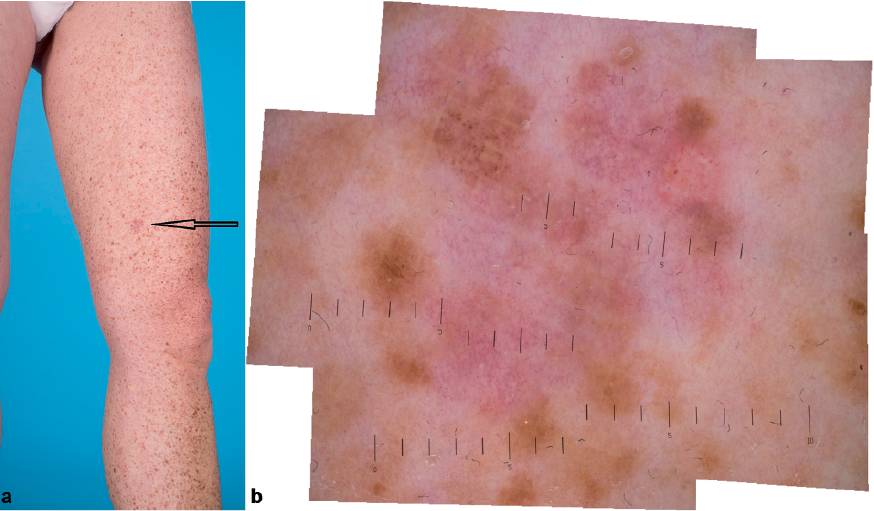
Fig. 1. (a) Patient 2 with a segmental naevus spilus on the left leg, melanoma indicated by the arrow. (b) Dermatoscopy of the melanoma on left leg (patient 2). The scale is in mm.
The back was the most common site of the NS. Two patients had NS smaller than 40 cm in diameter and 3 patients had NS larger than 40 cm. Two patients had congenital NS and 3 patients developed NS during childhood. Follow-up ranged from 10 to 120 months. Four invasive melanomas and one melanoma in situ appeared in 3 of our 5 patients. Three melanomas developed within the NS; patient 2 developed a melanoma within the NS on the leg, patient 3 developed 2 melanomas within the NS on the back and arm. In patient 3 a melanoma developed outside of the NS on the back. The melanoma in situ developed within the NS of patient 1 on the back. Melanomas were excised following the standard protocols, and histopathological investigation confirmed the diagnosis. In our cases, histopathology showed 2 superficial spreading melanomas; the subtypes of the other melanomas were unknown.
A review of the literature showed 11 other publications with segmental NS and melanoma (5, 11–13, 19, 27, 28, 33–36). However, it sometimes remained unclear whether a large or segmental NS was described.
We describe here 5 patients with NS > 20 cm with a segmental distribution. Three of 5 patients developed melanomas within and outside of the NS. Previously, NS were regarded as having no malignant potential; however, several reports of melanomas developing in NS have been published. From (37) reported that during 15 years of practice only 3 patients were found with melanoma within a NS. It was suggested that the malignant potential of NS appears to be 0.13% (9). Another group found no major risk of melanomas arising within NS (38). However, the number of patients with a NS was small; 27 of the 2,134 patients with a melanoma presented with a NS (all < 20 cm) in a different body region than the melanoma. A comparable study could not demonstrate NS as an important marker for melanoma risk: no significant difference was seen in the prevalence of NS between patients with cutaneous melanoma and controls from general dermatology outpatients (39). The number of patients with large NS (> 20 cm) was not reported. A review of the literature revealed 16 other patients with segmental NS and a melanoma (5, 11–13, 19, 27, 28, 33–36).
The specific risk of melanoma in large segmental NS has not been studied in the literature so far. A former analysis of 4 case reports concluded that the risk of developing a malignancy in a NS seems to increase when its size is ≥ 4 cm (9). In our patients, melanoma developed in 2 out of 3 patients with segmental NS > 40 cm. Another risk factor seems to be time of appearance of the NS. Two studies reported that in the majority of melanoma cases the NS were congenital (27, 28). It has been suggested that acquired NS have a different behaviour in terms of malignancy compared with congenital NS (13). Melanomas in our case series developed in both congenital and acquired NS. Also, the risk of developing a melanoma might be higher when the type of NS is macular rather than papular (9, 40). Lastly, the majority of published case reports of melanomas in NS are of the type SSM (5, 9, 28), followed by nodular melanoma. In our study, 2 superficial spreading melanomas (SSM), one melanoma of unknown type and one melanoma in situ developed within the segmental NS in 3 patients, all with a Breslow thickness < 1 mm.
The risk for melanoma arising in giant congenital naevi (according to the definition as > 20 cm in adulthood) is reported to be 5–15% (41). Although further data from the literature are missing, the risk of melanoma arising in giant congenital naevi seems to be lower than in large segmental NS. The fact that the Leiden University Medical Centre is a tertiary referral centre might explain the high number of melanoma (60%) in our case series, as a selection bias may have occurred; however, we think that most cases with a large segmental NS will be referred to our institution since our centre is the reference centre for the Netherlands.
Based on the case series reported here and the current literature, it appears that the risk of developing a melanoma in patients with (segmental) NS increases with lesions > 40 cm, harbouring a significant risk for the development of melanoma. It is unknown if the segmental distribution of NS contributes to the risk of melanoma. Since there are only reports on small case series, conclusions about other risk factors are speculative. Guidelines for the management of NS are lacking. We recommend following up patients with large segmental NS at least once per year with the aid of detailed photographs. Patients should be instructed how to perform self-examination. Suspicious lesions should be biopsied and sent for histopathological evaluation. An international database of large NS and multicentre studies on prevalence and risk factors of melanoma in (segmental) NS are needed to further characterize these patients and develop proper guidelines.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize