


1Department of Dermatology, and 2Clinical Investigation and Research Unit, Gunma University Graduate School of Medicine, Maebashi, Japan
The efficacy and safety of botulinum toxin B (BTX-B) for treatment of Raynaud’s phenomenon and digital ulcers in patients with systemic sclerosis was assessed. A total of 45 patients with systemic sclerosis who had Raynaud’s phenomenon were blinded and divided randomly into 4 groups: a no-treatment control group, and 3 treatment groups, using 250, 1,000 or 2,000 international units (U) of BTX-B injections in the hand with more severe symptoms. Four weeks after injection, pain/numbness visual analogue scale scores and Raynaud’s score in the groups treated with 1,000 and 2,000 U BTX-B were significantly lower than in the control group and the group treated with 250 U BTX-B. These beneficial effects were sustained until 16 weeks after the single injection. At 4 weeks after injection skin temperature recovery in the group treated with 2,000 U BTX-B was significantly improved. The numbers of digital ulcers in the groups treated with 1,000 and 2,000 U BTX-B were significantly lower than in the control group. In conclusion, 1,000 and 2,000 U BTX-B injections significantly suppressed the activity of Raynaud’s phenomenon and digital ulcers in patients with SSc without serious adverse events.
Key words: systemic sclerosis; botulinum toxin B; Raynaud’s phenomenon; digital ulcers; clinical trial.
Accepted Mar 27, 2017; Epub ahead of print Mar 30, 2017
Acta Derm Venereol 2017; 97: xx–xx.
Corr: Sei-ichiro Motegi, Department of Dermatology, Gunma University Graduate School of Medicine, 3-39-22 Showa-machi, Maebashi, Gunma, 371-8511, Japan. E-mail: smotegi@gunma-u.ac.jp
Systemic sclerosis (SSc) is an autoimmune generalized connective tissue disorder characterized by vascular dysfunction, and fibrosis of the skin and internal organs (1–3). More than 90% of patients with SSc develop Raynaud’s phenomenon (RP) and often develop digital ulcers (DUs). Several studies have reported that SSc patients with chronic DUs tend to have complications, including interstitial lung disease (ILD), cardiac involvement and decreased survival (4, 5). Cold exposure or emotional stress induce spasmodic contraction of the peripheral vessels that supply blood to the skin of the fingers and toes. The pathogenesis of RP in SSc is complex and still undetermined. It has been suggested that episodic vasospasm may be caused by dysregulation of the balance between vasoconstriction and vasodilation, and that dysregulation of the autonomic nervous response may be involved in the pathogenesis of RP (6). It has also been suggested that cold- or stress-induced noradrenaline stimulates adrenergic receptor α (ARα) on pericytes and/or vascular smooth muscle cells, resulting in vasoconstriction (7, 8). In addition, ARα responses are increased in the digital arteries in patients with SSc (8), suggesting that noradrenaline might be involved in the pathogenesis of RP in SSc. We reported recently that noradrenaline is also associated with the pathogenesis of fibrosis in SSc (9). Noradrenaline and other neurotransmitters, including substance P, glutamate, and calcitonin gene-related peptide, are increased in peripheral nerves of the affected skin and induce severe pain and numbness of fingers in patients with RP (10–14).
Pharmacological treatments of RP have targeted the regulation of vasodilation and/or vasoconstriction, and calcium channel blockers, antiplatelet agents, sarpogrelate hydrochloride, cilostazol, and oral and intravenous prostanoids have been administered. The endothelin receptor antagonist bosentan and phosphodiesterase-5 inhibitors may be beneficial for functional impairment in patients with SSc-related RP (15, 16). However, a satisfactory outcome for RP in SSc remains elusive. Several recent studies have shown the beneficial effects of botulinum toxin-A (BTX-A) on RP in patients with SSc (17–24). BTX-A at a dose of 10–100 international units (U) per hand on each neurovascular bundle at the level of the metacarpophalangeal joint was injected in patients with SSc with RP. The majority reported an improvement in severe resting pain and a reduction in the frequencies of RP. DU was also healed after BTX-A injection. There were a few adverse effects, such as intrinsic weakness and dysesthesia. However, these symptoms disappeared within 2–5 months after treatment. These results suggest that BTX-A might have therapeutic potential for RP and RP-related DU in patients with SSc.
Of 7 serotypes of BTX (A–G), BTX-A and BTX-B have been used widely for various therapeutic and cosmetic indications. BTX-A and BTX-B cleave SNARE proteins SNAP-25 and VAMP, respectively (25). Several studies demonstrated that the efficacy of BTX-B treatment appeared sooner than that of BTX-A, and that BTX-B was more effective than BTX-A in patients with diseases regulated by the autonomic nervous system (26–28). However, the efficacy of BTX-B injection for RP has not been examined. The objective of this study was to assess the efficacy and safety of BTX-B for RP in patients with SSc by a prospective, single-blind, randomized, investigator-initiated, clinical trial.
This investigator-initiated clinical trial was designed as a prospective, single-blind (patients-blind), randomized trial (trial registration: UMIN Clinical Trials Registry, https://upload.umin.ac.jp/cgi-open-bin/ctr_e/ctr_view.cgi?recptno=R000023017, UMIN000019985) at a single centre in Japan (Gunma University Hospital). Forty-five SSc patients with RP were screened and blinded and randomly selected for either a no-treatment control group or treatment groups given 250, 1,000, or 2,000 U of BTX-B injections per hand. Randomizations remained blinded to all patients who were injected with BTX-B until the data through week 16 were finalized. Random selection of patients was performed using the Hope eACReSS system (Fujitsu, Japan). The study was initiated in December 2015 and conducted over the winter months from 2015 to 2016 to maximize the development of RP, as well as to minimize seasonal effects on RP. This study was performed at the Department of Dermatology, and Clinical Investigation and Research Unit, Gunma University in Japan. The study was approved by the Institutional Review Board of Gunma University (#1367). All patients provided written informed consent before participation. Treatment was started at day 0 (baseline) and reviewed at weeks 4, 8, 12 and 16. The primary end-point was the change in severity of RP, including frequency, pain, colour and duration, according to the Raynaud’s score at 4 weeks after treatment, compared with baseline values. The secondary end-point was the difference in change in temperature at the tip of the treated finger from just after cold-water challenge to 10 min later, assessed with thermography at each visit. The changes in the number of DUs over 16 weeks, and the changes in the severity of RP according to the Raynaud’s score and VAS at 8, 12 and 16 weeks after treatment were compared with the baseline, and were also considered secondary outcome variables. Adverse events were reviewed at each visit.
A total of 45 Japanese patients (4 males, 41 females; mean age ± standard error (SE), 60.7 ± 1.9 years) with RP secondary to SSc were selected (Table I). All patients fulfilled the criteria of SSc proposed by the American College of Rheumatology (1980) (29) and the American College of Rheumatology/European League Against Rheumatism Classification Criteria (2013) (30). Twenty-five patients were classified as limited cutaneous type SSc (lcSSc) and 20 were classified as diffuse cutaneous type SSc (dcSSc) according to LeRoy et al.’s classification (31). Skin sclerosis was assessed using the modified Rodnan total skin score (mRTSS), and the mean mRTSS was 11.7 ± 1.2. Fifteen patients had DUs at the tips of their fingers at baseline. All patients had a history of severe RP for various periods and had taken oral prostanoids, beraprost sodium, and/or antiplatelet agents, such as sarpogrelate hydrochloride or cilostazol. Patients with DU were also treated with an intravenous prostanoid, including lipoprostaglandin E1. However, these therapies were not effective and severe RP and/or DU persisted before BTX-B treatment. Patients under 18 years of age, pregnant patients, and patients previously treated with BTX-B were excluded.
Table I. Demographic and clinical characteristics of 45 patients with systemic sclerosis (SSc) with Raynaud’s phenomenon (RP) in the botulinum toxin-B (BTX-B)-treated group and a control group with no treatment
The hand with the most severe symptoms in each patient was selected for injection. BTX-B was injected into both sides of all fingers (at 6 points: 50, 200 and 400 U/web space between fingers, and 25, 100 and 200 U/radial side of the thumb and ulnar side of the small finger, respectively). Each 2,500 U (0.5 ml) vial of BTX-B (NeuroBloc®, Eisai, Hatfield, UK) was diluted in 2.0 ml saline (1,000 U/ml). For the group treated with 250 U, 0.25 ml (250 U) of BTX-B was diluted in 2.25 ml saline (total: 2.5 ml). For the group treated with 1,000 U, 1 ml (1,000 U) BTX-B was diluted in 1.5 ml saline (total 2.5 ml). For the group treated with 2,000 U, 2 ml (2,000 U) BTX-B was diluted in 0.5 ml saline (total 2.5 ml). Then, 0.5 or 0.25 ml of these BTX-B dilutions were injected subcutaneously into the palmar aspect of the hand, targeting the neurovascular bundles just proximal to the A1 pulley, using a 30-gauge needle (Fig. 1a: injection points indicated by black mark). The changes in the severity of RP, including frequency, pain, colour, and duration, were assessed using Raynaud’s score (32, 33). The Raynaud’s score is a modified Raynaud’s Condition Score (34), used for assessment of RP activity (range 0–16), including frequency of attacks (0: none, 1: once per 2 weeks, 2: once per week, 3: once per 2 days, 4: every day), pain (0: none, 1: fairly rare, 2: rare, 3: sometimes, 4: always), colour (0: none, 1: red, 2: purple, 3: sometimes white, 4: always white), and duration of RP (0: none, 1: ≤ 15 min, 2: 15–30 min, 3: 30–60 min, 4: > 60 min). The total score at baseline was set as 100% and the relative scores at each visit were quantified. Pain/numbness severity was assessed using the 100-mm VAS (range 0–100: 0 is “no pain/numbness” and 100 is “pain/numbness as bad as imaginable”) (35). To assess the recovery of skin temperature in the treated finger, the skin temperature at the tip of the finger was measured just after and 10 min after an ice-bath immersion. First, both hands were put into cold water (12°C water bath) for 5 min. Both hands were then taken out of the cold water, and the skin temperature at the tip of the treated finger was measured using thermography in a temperature-controlled room (26°C). Ten min later, the skin temperature at the tip of the treated finger was recorded again, and the difference in temperatures from just after the cold-water challenge to 10 min later was recorded. The changes in the number of DUs were assessed during the 16-week period.
Fig. 1. Botulinum toxin-B (BTX-B) injection improved the symptoms of Raynaud’s phenomenon in patients with systemic sclerosis (SSc). (a) BTX-B was injected subcutaneously into the palmar aspect of the hand (black marker), just proximal to the A1 pulley, targeting the neurovascular bundles. (b) The mean values of Raynaud’s score in patients with SSc in the no-treatment control group or treatment groups using 250, 1,000, and 2,000 U BTX-B injections per hand 4 weeks after injection. The value of Raynaud’s score at baseline was assigned a value of 100%. **p < 0.01, *p < 0.05. (c) The mean values of Raynaud’s score in the no-treatment control group or treatment groups using 250, 1,000, and 2,000 U of BTX-B injections per hand during 16 weeks. The mean air temperature in our city at the examined days of all patients. The value of Raynaud’s score at baseline was assigned a value of 100%. **p < 0.01, *p < 0.05 relative to values in the no treatment control group at each visit over 16 weeks.
p-values were calculated using one-way analysis of variance (ANOVA), followed by Bonferroni’s post hoc test. χ2 analysis was used to compare frequencies. Error bars represent the standard errors of the mean.
It has been suggested that BTX-B is as effective as approximately 20–40× the dose of BTX-A in the treatment of several diseases (36, 37). Since we reported previously that 10 U BTX-A per injection site improved the symptoms of RP (24), we used 3 doses of BTX-B: 50 U (5×10 U: total 250 U per hand), 200 U (20×10 U: total 1,000 U per hand), and 400 U (40×10 U: total 2,000 U per hand) per injection site in the present study. Among 45 patients with SSc, 9 SSc patients with RP in the group treated with 250 U (mean age 55.4 years), 10 patients in the group trea-ted with 1,000 U (mean age 65 years), 18 patients in the group treated with 2,000 U (mean age 61.7 years), and 8 SSc patients in the no-treatment control group (mean age 58.8 years) were randomly selected (Table I). The ratios of lcSSc and dcSSc, total skin thickness score (mRTSS), and the positivity of autoantibodies in each group were comparable. The frequency of DU in patients at baseline was comparable between the 4 groups; however, the total number of DUs at baseline was different between the 4 groups (no-treatment: n = 3, BTX-B 250 U: n = 5, BTX-B 1,000 U: n = 3, BTX-B 2,000 U: n = 13). No significant differences in the frequency of ILD, pulmonary arterial hypertension, and reflux oesophagitis were identified in the 4 groups.
The present study was started in winter, and the mean temperature in our city was below 10°C from December 2015 to March 2016 (38). Therefore, the Raynaud’s score (indicating the severity of RP, including frequency, pain, and duration) in the no-treatment control group was exacerbated at 4 weeks after injection (Fig. 1b, c). Raynaud’s score in the group treated with 250 U BTX-B was significantly lower than that in the control group (p < 0.05, Fig. 1b, c). Raynaud’s scores in the groups treated with 1,000 and 2,000 U BTX-B were also significantly lower than those in control group and the group treated with 250 U BTX-B (p < 0.01, Fig. 1b, c). Raynaud’s scores in the groups treated with 1,000 and 2,000 U BTX-B were comparable. Since the mean air temperature in our city at approximately 16 weeks after injection had increased, Raynaud’s score in the control group also decreased 12 weeks after injection (Fig. 1c). Raynaud’s score in the group treated with 250 U BTX-B also decreased gradually, but was not significantly different from the score in the control group. In contrast, Raynaud’s scores in the groups treated with 1,000 and 2,000 U BTX-B were significantly reduced starting 4–16 weeks after injection (Fig. 1c). These results suggest that 1,000 and 2,000 U BTX-B injections might improve the activity of RP, including the frequency of attacks/pain, colour changes and duration of RP; the beneficial effects of 1,000 and 2,000 U injections were sustained until 16 weeks after the single injection.
Similar to the results of Raynaud’s score, pain and/or numbness VAS in no-treatment control group was exacerbated at 4 weeks after injection (Fig. 2a, b). Although VAS in the group treated with 250 U BTX-B tended to be lower than in the control group, this difference did not reach statistical significance (Fig. 2a, b). VAS scores in the groups treated with 1,000 and 2,000 U BTX-B were significantly lower than in the control group at 4 weeks after injection (Fig. 2a, b). VAS scores in the groups treated with 1,000 and 2,000 U BTX-B were comparable. Although the mean temperature in our city at 16 weeks after injection was elevated, VAS score in the control group was not decreased until 12 weeks after injection (Fig. 1b). In contrast, VAS scores in the groups treated with 250, 1,000 and 2,000 U BTX-B gradually decreased, and VAS scores in the groups treated with 1,000 and 2,000 U BTX-B were significantly reduced 4–16 weeks after injection, compared with the score in the control group (Fig. 2b). These results suggest that 1,000 and 2,000 U BTX-B injections might resolve pain and/or numbness in the fingers and hand caused by RP; the beneficial effects of 1,000 and 2,000 U BTX-B injections were also sustained until 16 weeks after the single injection.
Fig. 2. Botulinum toxin-B (BTX-B) injection improved the pain/numbness of Raynaud’s phenomenon in patients with systemic sclerosis (SSc). (a) The mean values of pain/numbness visual analogue scale (VAS) in patients with SSc in the no-treatment control group or treatment groups using 250, 1,000 and 2,000 international units (U) of BTX-B injections per hand at 4 weeks after injection. The value of VAS at baseline was assigned a value of 100%. **p < 0.01. (b) The mean values of pain/numbness VAS in the no-treatment control group or treatment groups using 250, 1,000, and 2,000 U BTX-B injections per hand during 16 weeks. The mean air temperature in our city at the examined days of all patients. The value of VAS at baseline was assigned a value of 100%. **p < 0.01, *p < 0.05 relative to values in no treatment control group at each visit over 16 weeks.
Next, we examined the skin surface temperature before and after BTX-B injection using thermography. To avoid the effect of air temperature, the differences in temperature from just after to 10 min after cold-water stimulation were measured. At 4 weeks after BTX-B injection, the skin temperature recovery after cold-water stimulation in the group treated with 2,000 U BTX-B was significantly improved compared with the control group and the group treated with 250 U BTX-B (Fig. 3a). In the group treated with 2,000 U BTX-B, a thermographic image at 10 min after cold-water stimulation at 4 weeks after BTX-B injection showed that the skin temperatures in the BTX-B injected fingers of the right hand were significantly elevated compared with those in the non-treated fingers of the left hand (Fig. 3b). Skin temperature recovery after cold-water stimulation in the group treated with 2,000 U BTX-B tended to be faster than in the control group from 8 to 16 weeks after injection, but this difference did not reach statistical significance (Fig. 3c). These results suggest that BTX-B injection might enhance blood flow to the fingers, leading to enhancement of skin surface temperature recovery after cold-water stimulation.
Fig. 3. Botulinum toxin-B (BTX-B) injection enhanced the skin temperature recovery after cold-water stimulation. (a) Mean values of skin surface temperature recovery after cold-water stimulation in patients with systemic sclerosis (SSc) in the no-treatment control group or treatment groups using 250, 1,000 and 2,000 U BTX-B injections per hand at 4 weeks after injection. The value of skin surface temperature recovery after cold-water stimulation at baseline was assigned a value of 1. **p < 0.01. (b) Thermographic images at just after and 10 min after cold-water stimulation at baseline and 4 weeks after 2,000 U BTX-B injection. BTX-B injected hand is indicated by an arrow. (c) Mean values of skin surface temperature recovery after cold-water stimulation in the no-treatment control group or treatment groups using 250, 1,000 and 2,000 U BTX-B injections per hand during 16 weeks. The mean air temperature in our city is shown for the examined days for all patients. The value of skin surface temperature recovery after cold-water stimulation at baseline was assigned a value of 1. **p < 0.01, relative to values in no treatment control group at each visit over 16 weeks.
At baseline, 3 SSc patients with RP in the no-treatment group had intractable DUs on the tips of the fingers; treatment with oral prostanoids and antiplatelet agents for 16 weeks did not heal the DUs (Fig. 4a). In contrast, 3 DUs were present at baseline in the group treated with 1,000 U, and all DUs were healed at 4 weeks after injection. In addition, 10 out of 13 DUs in the group treated with 2,000 U were healed at 4 weeks after injection, and all DUs were healed within 16 weeks after injection (Fig. 4a). The numbers of DUs in the groups treated with 1,000 and 2,000 U were significantly lower than those in the control group 4–16 weeks after injection (Fig. 4a). Furthermore, in the control group, 4 new DUs developed at 4 weeks after injection, and a total of 7 DUs appeared by 16 weeks after injection (Fig. 4b). However, no new DUs developed in the groups treated with 1,000 and 2,000 U for 16 weeks after injection (Fig. 4b). A representative result in the group treated with 2,000 U showed that a DU on the tip of the finger of one SSc patient with RP at baseline was healed 4 weeks after BTX-B injection (Fig. 4c). These results suggest that 1,000 and 2,000 U BTX-B injections might accelerate the healing of RP-related intractable DUs and prevent formation of new DUs.
Among adverse effects, transient muscle weakness occurred in one patient in the group treated with 2,000 U from 5 days to 3 weeks after injection, but no systemic or local adverse events, such as an anaphylactic reaction, reduction in muscle contraction force, swallowing difficulty, dry mouth, and abnormal liver function, were observed in any patients. Patients experienced pain at the injection sites, but this pain disappeared within a few hours.
Fig. 4. Raynaud’s phenomenon-related intractable digital ulcers were healed after BTX-B injection. (a) Rate of digital ulcers (DUs) in patients with systemic sclerosis (SSc) in the no-treatment control group or treatment groups using 250, 1,000 and 2,000 U BTX-B injections per hand during 16 weeks. The mean air temperature in our city on the examined days for all patients. The number of DUs appeared at baseline was assigned a value of 100%. **p < 0.01, *p < 0.05 relative to values in no treatment control group at each visit over 16 weeks. (b) The number of new DUs in patients with SSc in the no-treatment control group or treatment groups using 250, 1,000 and 2,000 U of BTX-B injections per hand during 16 weeks. (c) A representative result in the group treated with 2,000 U showed that a DU on the tip of the finger of one patient with SSc healed 4 weeks after BTX-B injection.
To the best of our knowledge, this is the first clinical study to examine the effects of BTX-B injection on RP and RP-related DU in patients with SSc. Our study found that 1,000 and 2,000 U BTX-B injection significantly improved the activity of RP, including the frequency of attacks/pain, colour changes, duration of RP, and the severity of pain/numbness in SSc patients. Furthermore, the efficacies of 1,000 and 2,000 U were sustained until 16 weeks after a single injection. In contrast, the efficacy of treatment with 250 U BTX-B was weak, and comparable to that of the no-treatment control group, suggesting that more than 250 U BTX-B might be an appropriate dose for RP in Japanese patients with SSc. In the group treated with 2,000 U, transient muscle weakness occurred in only one patient, but no serious adverse events were experienced. In addition, the maximum dose of BTX-B injection for the treatment of spasmodic torticollis in Japan is 10,000 U, suggesting that 4,000 U BTX-B injection into the hand might be well tolerated in clinical use for the treatment of RP in SSc. However, further studies are required.
In addition, a 1,000 and 2,000 U BTX-B injection accelerated the healing of RP-related intractable DUs, and prevented new formation of DUs, indicating that BTX-B might have therapeutic potential for severe RP symptoms. The oral endothelin receptor antagonist, bosentan, is clinically used for the prevention and treatment of DU in patients with SSc (39). In the present study, only one patient in the group treated with 2,000 U received bosentan before BTX-B treatment for several years, but severe RP and 3 DUs in the left hand were present at baseline. It is of note that all DUs were healed at 4 weeks after injection. Since the route of administration and the mechanisms by which bosentan and BTX-B dilate the peripheral blood vessels are different, the combination treatment with bosentan and BTX-B may have an additive effect for RP-related DU.
In the present study, a 2,000 U BTX-B injection enhanced skin surface temperature recovery after cold-water stimulation at 4 weeks after injection, suggesting that BTX-B might enhance blood flow to the fingers. In addition, Schweizer et al. (40) reported that both BTX-A and B enhanced blood flow and survival of ischaemic cutaneous flaps using animal models. The mechanisms by which BTX-A and B improve impaired blood flow to the fingers are unclear. It has been suggested that cold- or stress-induced noradrenaline causes vasoconstriction (6, 7), and that this response might be involved in the pathogenesis of RP in SSc. Morris et al. reported that BTX-A inhibited sympathetic vasoconstriction through attenuation of noradrenaline release in autonomic neurones (41), suggesting that BTX-B also might inhibit noradrenaline release, leading to the inhibition of spasm and vascular contraction and enhancement of blood flow. This mechanism may be considered to contribute to the improvement in RP with BTX-B. However, further research is needed to clarify the mechanisms of the improvement of RP with BTX-B.
BTX can block the release of various neuropeptides, including calcitonin gene-related peptide (CGRP), glutamate, and substance P, which increase in chronic nerve irritation and pain and can exacerbate these symptoms (12, 14, 42); this suggests that BTX-A and B may inhibit the release of pain/numbness-related neuropeptides, resulting in the reduction in pain/numbness in the fingers in SSc patients with RP. However, the inhibition of the neurogenic inflammation with less release of neuropeptides, such as substance P, CGRP and vasoactive intestinal peptide (VIP), might inhibit vasodilatation.
In addition, BTX-B inhibits sweating of the palms (43, 44); therefore, injection of BTX-B might inhibit such sweating, and the consequent cooling of the fingers, which may be a trigger for RP. This mechanism may be associated with the improvement in RP by BTX-B.
Several clinical differences between BTX-A and B have been reported. Several studies have demonstrated that the efficacy of BTX-B treatment in forehead wrinkles appeared sooner than that with BTX-A (26, 45, 46). In an animal cutaneous flap model, BTX-B showed faster onset of vasodilation and better flap survival than BTX-A (40). These results suggest that the early response to BTX-B treatment may be of benefit in BTX injection therapy for RP. In addition, several studies have indicated that BTX-B is highly effective in the treatment of diseases regulated by the autonomic nervous system, such as hyperhidrosis, sialorrhoea, spasticity, and dystonia, compared with BTX-A (26–28). RP is thought to result from dysregulation of vasoconstriction/vasodilation by the autonomic nervous system, suggesting that BTX-B may have a highly beneficial effect on RP compared with that of BTX-A.
It has been suggested that BTX-A and BTX-B at 1:20 to 1:40 dose ratios were equally effective in the treatment of several diseases (36, 37). Based on these findings, and 10 U of BTX-A injection per injection site was performed in our previous study (24), we selected the dose of BTX-B in our study, as 50 (5×10 U), 200 (20×10 U) and 400 U (40×10 U) per injection site. However, Rystedt et al. reported the dose-response studies on healthy volunteers, investing BTX-A and BTX-B on autonomic sympathetic sudomotor fibres, and the dose conversion ratio was found to be 1:1.1–1.3 (43), suggesting that our selected doses of BTX-B (50, 100 and 200 U) may not be the optimal for autonomic (sudomotor) fibres. In addition, Rystedt et al. (44) reported that the optimal concentration of BTX-B for anhidrotic effect was 100 U/ml. We used BTX-B at concentrations of 100, 400 and 800 U/ml, suggesting that our dilutions may not be the optimal for autonomic (sudomotor) fibres.
It is known that repeated injection of BTX results in a poor clinical response due to the presence of neutralizing antibodies to BTX (47). Thus, BTX-B may be effective in patients with failure of or resistance to BTX-A. Our previous and present results suggest that both BTX-A and B are effective in RP and RP-related DU in patients with SSc, and that BTX-B might be useful for RP resistant to BTX-A treatment.
In conclusion, 1,000 and 2,000 U of BTX-B injection per hand demonstrated a beneficial therapeutic effect on RP and RP-related DU in patients with SSc without any serious adverse events. The clinical effectiveness of BTX-B was sustained for 16 weeks after a single injection, suggesting that BTX-B might have potential as a long-term preventive and therapeutic agent for RP and DU in patients with SSc, and that SSc patients with RP could be protected from severe exacerbation of RP-associated symptoms during winter with a single injection of BTX-B. A limitation of this study is the lack of a placebo control; therefore, further placebo-control studies are warranted.
This work was supported by Science Research Grant of Project for Securing High Quality Clinical Research (Gunma University Hospital), institutions selected by the Japanese Ministry of Health, Labour and Welfare in fiscal year 2013, Japan (to T. N.).
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize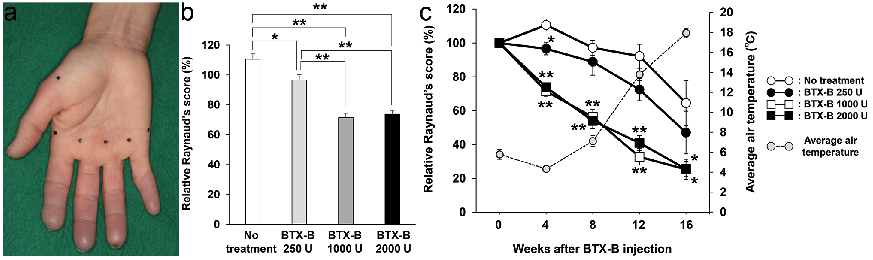 Click to show fullsize
Click to show fullsize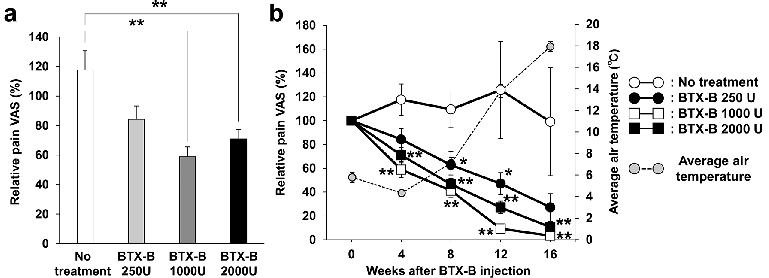 Click to show fullsize
Click to show fullsize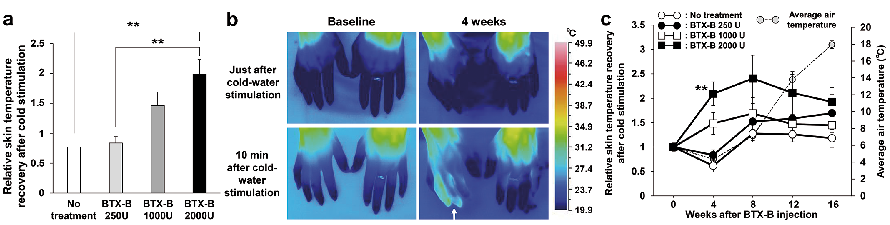 Click to show fullsize
Click to show fullsize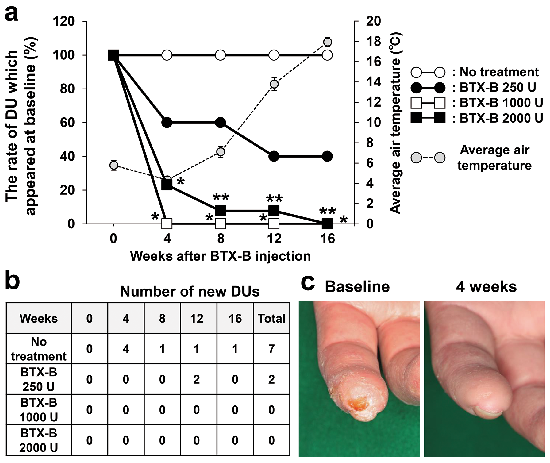 Click to show fullsize
Click to show fullsize