


1Department of Dermatology and Allergy, 2Department of Cardiology, Herlev and Gentofte Hospital, University of Copenhagen, Hellerup, 3The Danish Heart Foundation, 4The National Institute of Public Health, University of Southern Denmark, Copenhagen, Denmark, and 5Eli Lilly and Co, Indianapolis, Indiana, USA
The incidence and temporal trends of psoriasis in Denmark between 2003 and 2012 were examined. There was a female predominance ranging between 50.0% (2007) and 55.4% (2009), and the mean age at time of diagnosis was 47.7–58.7 years. A total of 126,055 patients with psoriasis (prevalence 2.2%) were identified. Incidence rates of psoriasis (per 100,000 person years) ranged from 107.5 in 2005 to a peak incidence of 199.5 in 2010. Incidence rates were higher for women, and patients aged 60–69 years, respectively. Use of systemic non-biologic agents, i.e. methotrexate, cyclosporine, retinoids, or psoralen plus ultraviolet A (PUVA) increased over the study course, and were used in 15.0% of all patients. Biologic agents (efalizumab, etanercept, infliximab, adalimumab, or ustekinumab) were utilized in 2.7% of patients. On a national level, incidence of psoriasis fluctuated during the 10-year study course. The relationship between psoriasis incidence and age appeared to be relatively linear, and disease prevalence was comparable to that in other European countries.
Key words: psoriasis; incidence; prevalence; epidemiology.
Accepted Apr 6, 2017; Epub ahead of print Apr 17, 2017
Acta Derm Venereol 2017; 97: xx–xx.
Corr: Alexander Egeberg, Department of Dermatology and Allergy, Herlev and Gentofte Hospital, Kildegårdsvej 28, DK-2900 Hellerup, Denmark. E-mail: alexander.egeberg@gmail.com
Psoriasis is a prevalent chronic inflammatory disease characterized by localized or widespread, thick, silvery-white, scaly, pruritic plaques. The exact aetiology of psoriasis is not fully understood, but both genetic and environmental factors are involved in the onset and progression of the disease (1). Approximately 70–80% of all patients with psoriasis are considered to have mild disease that can be managed with topical treatment alone (2, 3). Studies have shown that psoriasis negatively affects patients’ quality of life, and that depression occurs more often than in controls (2, 4, 5). Along this line, studies have also shown that psoriasis is a systemic disease, which also affects the joints, vasculature and other tissues. Indeed, approximately one-third of patients with psoriasis develop psoriatic arthritis, and patients with severe psoriasis have a shortened life expectancy as well as several major comorbidities (6, 7).
While most recent epidemiological studies have examined comorbidities in psoriasis, potential changes in disease prevalence and incidence are less common. Based on past studies, psoriasis is estimated to affect approximately 2–4% of the population in western countries (8); however, the prevalence varies with age, sex, geography and ethnicity. For example, while some studies have suggested that the onset of psoriasis is bimodal, with peaks at ages between 15 and 20 years and, later, at between 55 and 60 years (2), others have described that the prevalence increases are roughly linear over the life-course (3). Since few studies on psoriasis prevalence in Denmark have been published (9–11), we examined the time trend in incidence, as well as the prevalence of psoriasis in a Danish nationwide cohort.
Study approval was obtained from the Danish Data Protection Agency (ref. 2007-58-0015, int. ref. GEH-2014-018, I-Suite 02736). Approval from an ethics committee is not required for registry studies in Denmark. The study was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) recommendations (12).
Using the unique personal identification number assigned to all Danish citizens, individual-level information from nationwide administrative registers was linked. The Civil Registration System (13) contains information on sex, date of birth, and updated information on vital status and emigration, thus minimizing loss to follow-up. All inpatient and outpatient (ambulatory) hospital consultations are recorded in the Danish National Patient Register (DNPR) (14) including one primary and up to 19 secondary diagnoses coded by discharging physicians according to the International Classification of Diseases, 8th revision (ICD-8) (prior to 1994), and according to the 10th revision (ICD-10) thereafter. The primary diagnosis is the main reason for the hospital consultation or hospitalization, and secondary diagnoses are additional conditions, including complications. The DNPR was established in 1977, and outpatient data has been available from 1995 onwards. Since 1994, detailed and accurate information on all pharmacy-dispensed medications has been registered in the Danish Registry of Medicinal Products Statistics according to the Anatomical Therapeutic Chemical (ATC) classification (15). Hospital administered pharmacotherapy is coded in the DNPR as treatment procedure (SKS) codes. We defined patients with incident psoriasis as those recorded with a corresponding first-time ICD-10 code (L40) or an ATC code for pharmacotherapy for use exclusively in psoriasis (D05AX), and thus excluded all patients with a history of psoriasis based on the above criteria before 1 January 2003 in analyses of incident psoriasis. When examining the prevalence of psoriasis, these patients were not excluded. The study period was divided into 1-year groups from 2003 to 2012. We identified use of systemic therapy, i.e. methotrexate, cyclosporine, PUVA, retinoids, efalizumab, etanercept, infliximab, adalimumab, and ustekinumab.
The number of incident psoriasis cases within each of the predefined 1-year periods was estimated and the frequency of psoriasis cases within sex and age subgroups (0–19, 20–29, 30–39, 40–49, 50–59, 60–69, 70+ years) calculated. The incidence rate within each 1-year period was computed as the number of newly diagnosed psoriasis cases divided by the risk time of the underlying population. The population size in each of the 1-year periods was estimated as the number of Danes alive in the mid-year of each period, as recorded in the Civil Registration System, and the risk time as 1 year times the estimated number of Danes in each period. The prevalence of psoriasis was estimated among all Danes alive and resident in the source population on 31 December 2012. Due to data security requirements, data on 1 or 2 subjects are shown as “less than 3”, and the derived percentages are not shown. SAS statistical software version 9.4 (SAS Institute Inc. Cary, NC, USA) was used for statistical analysis.
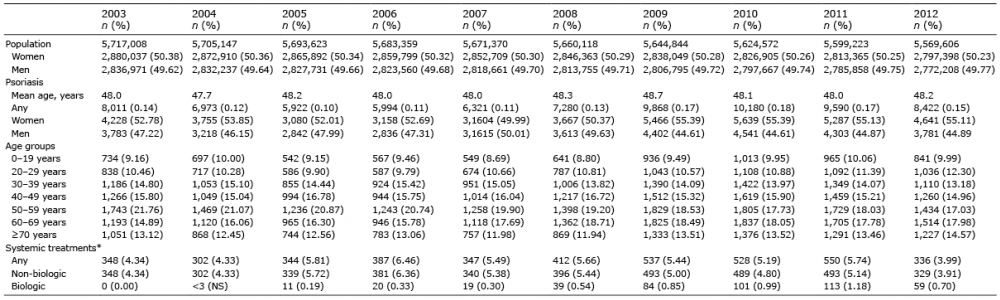
During the study period, the total Danish population comprised approximately 5.7 million individuals with nearly equal sex distribution. Among patients with psoriasis there was a slight female predominance, ranging from 50.0% (2007) to 55.4% (2009/2010), and the mean age at time of diagnosis was between 47.7 and 48.7 years (Table I).
Table I. Characteristics of patients with first-time psoriasis in Denmark
The incidence of psoriasis (presented as incidence rates per 100,000 person-years) ranged from 107.5 in 2005 to a peak incidence of 199.5 in 2010 (Fig. 1 and Table II).
Fig. 1. Incidence rates of psoriasis. Total and sex-specific incidence rates per 100,000 person-years of psoriasis over the study period 2003 to 2012. Blue: overall; Red: women; Green: men.
Table II. Incidence rates per 100,000 person-years of psoriasis in Denmark, 2003 to 2012
Estimates with 25% error margins are shown in Fig. 2. The highest percentage of patients with incident psoriasis was initially observed among individuals aged between 50 and 59 years, but during the study course there was a shift towards a higher incidence in individuals aged between 60 and 69 years. Incident psoriasis was least frequent among younger individuals aged 0–19 years (Table I and Fig. 3). Similarly, age-specific incidence rates were highest among subjects aged 60–69 years and lowest among individuals aged 0–19 years (Fig. 4).
Fig. 2. Incidence rates of psoriasis, with 95% confidence intervals.
Fig. 3. Distribution of incident psoriasis, stratified by age.
Fig. 4. Age-specific incidence rates of psoriasis per 100,000 person-years over the study period 2003 to 2012.
Use of systemic non-biologic agents increased over the 10-year study course. The first recorded use of biologic agents for patients classified with psoriasis within the same year, occurred in 2004, after which their use steadily increased (Table I).
As shown in Table III, a total of 126,055 patients with psoriasis were identified (prevalence 2.2%), and patients were predominantly female (54%) with a mean age of 45 years. The highest prevalence was among patients aged 60–69 years, followed by those aged 50–59 years (Table III and Fig. 5). Fifteen percent of patients had received treatment with systemic non-biologic immunosuppressants, whereas biologics were used in 2.7% of patients (Table III).
Table III. Characteristics and prevalence of patients with psoriasis on 31 December 2012
Fig. 5. Distribution of prevalent psoriasis (% with psoriasis of all Danish residents) on 31 December 2012, stratified by age.
In this nationwide study of the Danish population, an overall psoriasis prevalence of 2.2% was identified. We described the temporal trends in the incidence of psoriasis between 2003 and 2012, and found the highest incidence among older individuals and females. Fifteen percent of patients received treatment with systemic non-biologic therapy, and one-fifth of patients were treated with biologics at some point.
While a number of studies from different countries have examined the prevalence of psoriasis (8), the prevalence in Denmark remains poorly characterized. One previous survey-based study from 1981 examined the prevalence of psoriasis in Denmark among individuals aged 16–99 years (9) in which the estimated point prevalence was 3.2% and 2.5% for men and women, respectively. Moreover, it was estimated that a total of 113,000 Danish residents had psoriasis, whereas 2 survey-based studies indicated a prevalence of 3–4% (10, 11). On the other hand, a 1964 study from the Faroe Islands reported a psoriasis prevalence of 2.8% (16). Data from other Scandinavian countries have shown similar results, with an overall prevalence of 2.0% (women 2.3%; men 1.5%) in Sweden (8), and a somewhat lower prevalence among children (girls 2.3%; boys 1.5%) (17). While older Norwegian studies have reported a prevalence of 1.4% (18, 19), newer data suggest that the prevalence in Norway may be as high as 8.5% (20). However, a fundamental limitation of the abovementioned studies is the cross-sectional design, since temporal changes in incidence and prevalence of psoriasis may occur.
We found a higher incidence of psoriasis among women. Similar findings have been reported in some, but not all, studies (8). Although speculative, it is plausible that men may not seek medical treatment for their psoriasis and thereby go undiagnosed to a greater extent than women. Because of its nationwide and population-based design within a setting with equal access to healthcare for the entire population, the risk of referral and selection bias is arguably very low, and our study is likely to provide highly generalizable results. Nonetheless, certain limitations need to be addressed. Despite unfettered access to healthcare in Denmark, including general practitioners and hospitals, it is likely that some patients may not seek medical treatment for their psoriasis, resulting in conservative estimates of incidence and prevalence, and a bias towards a higher incidence in older age due to diagnostic delay. While some studies have suggested a bimodal peak in psoriasis incidence, the somewhat linear increase observed in our study is in line supported by Boehncke & Schon, stating that the increase is “roughly linear over the life course” (3). Also, patients in primary or secondary care who were treated with topical corticosteroids alone or ultraviolet B (UVB) treatment were not included, as these would not have been captured in the DNPR. However, in Denmark, topical vitamin D analogues are the preferred first-line therapy for psoriasis, and used in 94% of patients with psoriasis (21). Nevertheless, assuming a 25% error margin in the prevalence of psoriasis, the most conservative and liberal estimates would yield 94,541 (prevalence 1.7%) and 157,569 (prevalence 2.8%), respectively. Nevertheless, we identified psoriasis based on either a diagnosis or use of highly psoriasis-specific pharmacotherapy. However, since all patients were not necessarily diagnosed by dermatologists, we cannot refute that some misclassification may have occurred, since studies have suggested that psoriasis can be difficult to diagnose, especially in children (22). Misclassification of patients with psoriasis as having other skin disease, or if patients did not seek medical attention, would lead to an underestimation of the true incidence and prevalence. On the other hand, if patients with other skin disease were misclassified as having psoriasis, this would lead to an overestimation of incidence and prevalence. However, we believe that such misclassification would be non-differential between the different time points (2003 to 2012) and is unlikely to explain the observed time trends. The general population distribution has been stable in Denmark during the current study period. Nevertheless, in Fig 2, a more conservative approach has been applied to show the estimated time trends in psoriasis incidence in Denmark. Indeed, assessment of incidence of psoriasis is a fundamental issue in all large-scale settings because of the difficulty in accurately identifying and documenting such cases. Indeed, given the considerations listed above, the present findings should be interpreted accordingly and with caution.
In conclusion, the incidence of psoriasis fluctuated during the 10-year study period, albeit that we did not observe a marked increase. The disease prevalence was comparable to recent studies from other Scandinavian countries.
Declaration of interests: AE has received research funding from Pfizer and Eli Lilly, and honoraria as consultant and/or speaker from Pfizer, Eli Lilly, Novartis, Galderma, and Janssen Pharmaceuticals. JPT is supported by an unrestricted grant from the Lundbeck Foundation and has received speaker honoraria from Galderma and MEDA and attended advisory board meetings for Roche and Sanofi-Genzyme. GHG is supported by an unrestricted research scholarship from the Novo Nordisk Foundation. LS has received consultancy and/or speaker honoraria from Abbvie, Pfizer, Janssen-Cilag, Merck Sharp & Dohme, and Leo Pharma and is a member of the advisory boards of Abbvie, Pfizer, Janssen-Cilag, Merck Sharp & Dohme, Eli Lilly, Celgene, Leo Pharma and Novartis. LM is currently employed by Eli Lilly and Co.
Funding sources: Eli Lilly and Co. The funding sources participated in interpretation of the final analysed study results, but had no access to the raw data, and did not participate in data collection, management, or analysis.


 Click to show fullsize
Click to show fullsize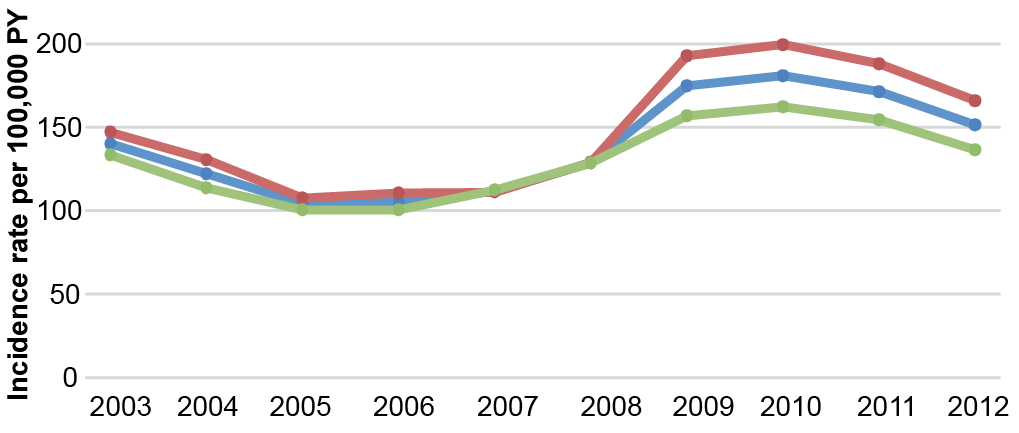 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize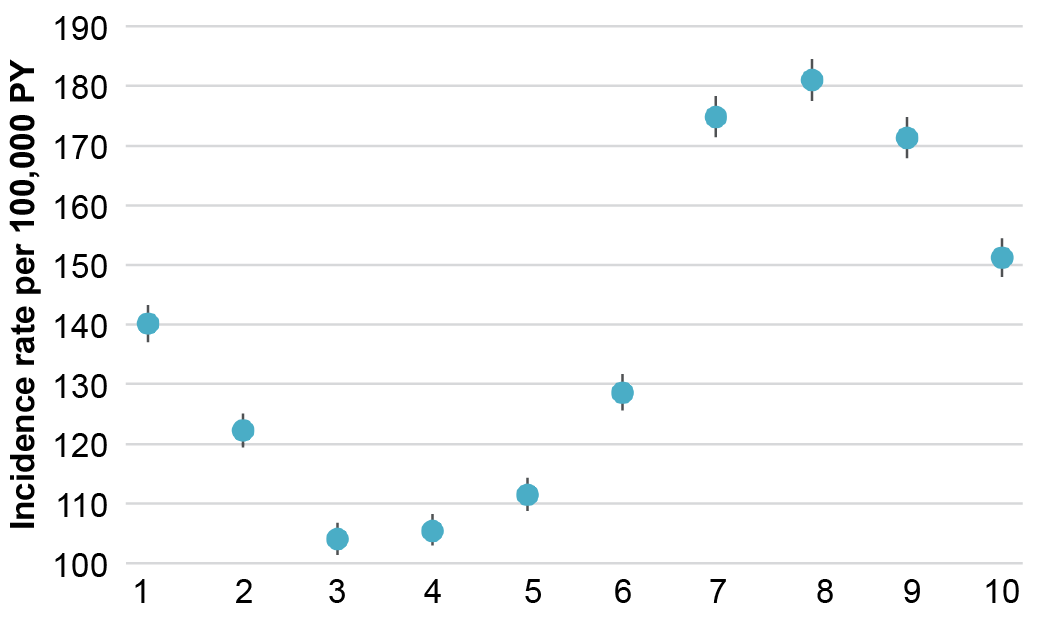 Click to show fullsize
Click to show fullsize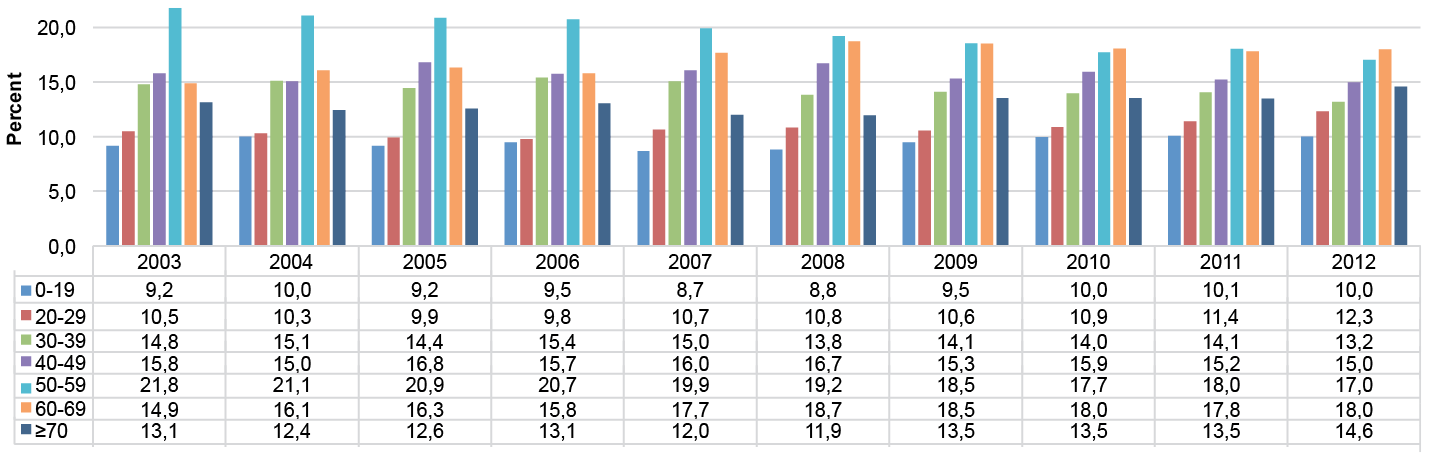 Click to show fullsize
Click to show fullsize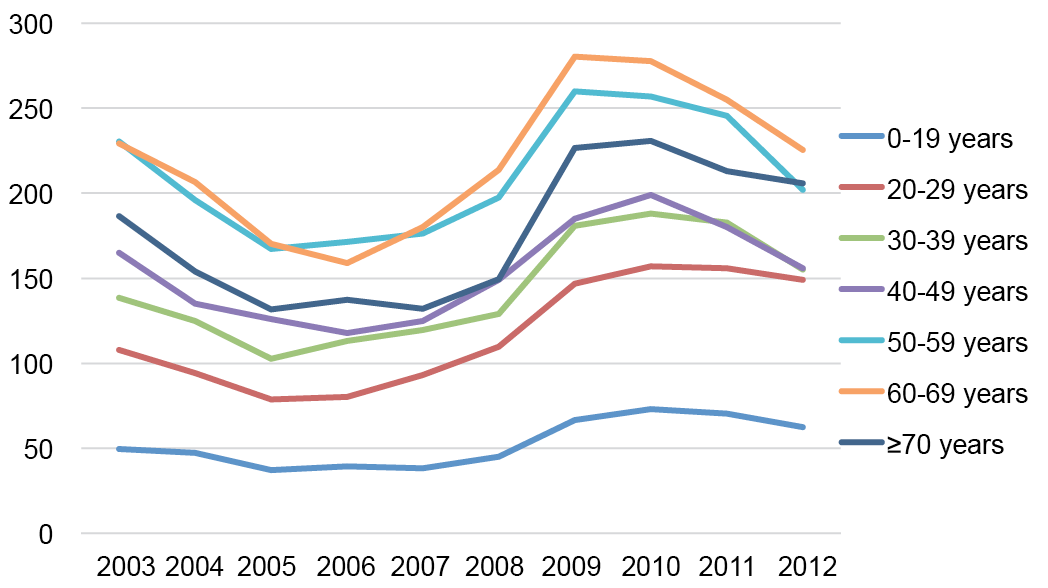 Click to show fullsize
Click to show fullsize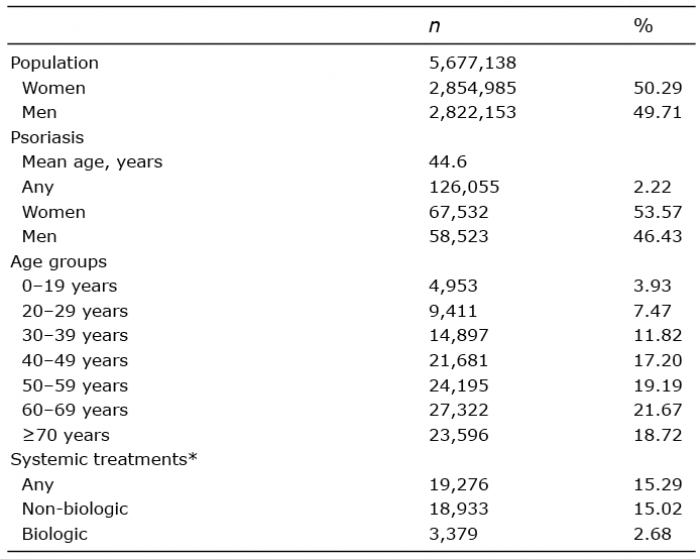 Click to show fullsize
Click to show fullsize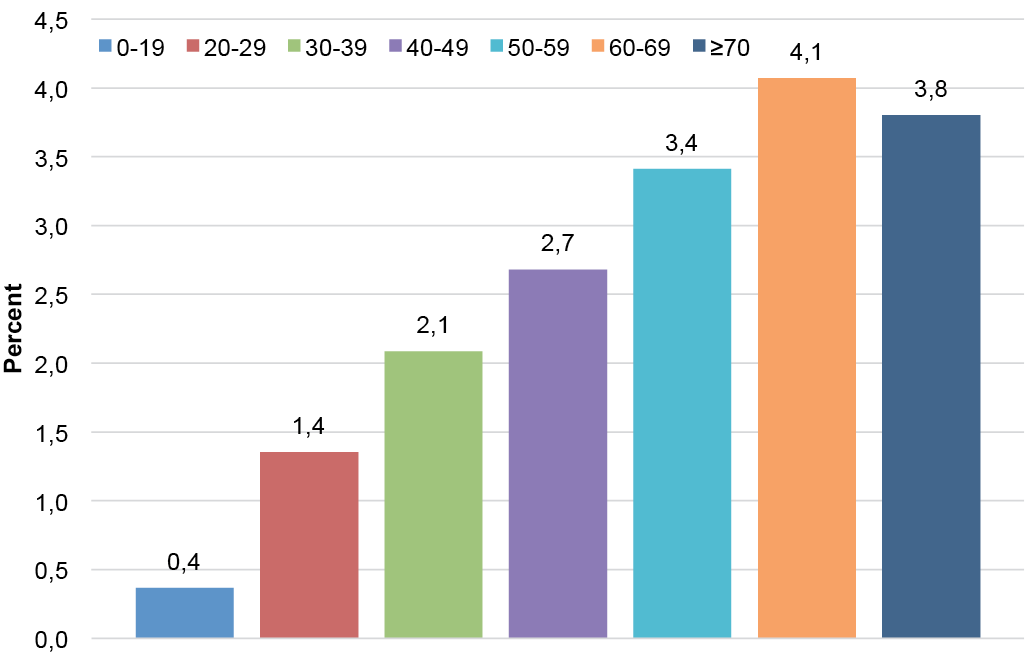 Click to show fullsize
Click to show fullsize