


1Melanoma Clinic and Teledermatology Network, University Hospital Virgen Macarena, Seville, Spain, and 2Department of Dermatology, University of Campania, Naples, Italy
Teledermatology and smartphone mobile applications have been at the forefront of advances in the screening and management of patients with skin lesions over the past decade. The Spanish teledermatology network, established in 2004 in the area surrounding the dermatology clinic in Seville, has now managed over 50,000 teleconsultations and has led to validated improvements in waiting times for referral and surgery, allowed patients to be treated in local settings, and improved the early diagnosis and initial prognosis of patients diagnosed with melanoma. Both teledermatology and smartphone mobile applications can be used as training tools to improve the diagnostic skills of physicians and dermatologists. They can also serve as rapid and reliable methods to prioritize patient care and ensure that specialized services and treatments are accessible regardless of patient circumstances.
Key words: teledermatology; skin cancer screening; mobile application; teleconsultation; dermoscopy.
Accepted May 22, 2017; Epub ahead of print Jul 3, 2017
Acta Derm Venereol 2017; Suppl 218: 31–35.
Corr: David Moreno-Ramirez, Dermatology Unit, University Hospital Virgen Macarena, ES-41009 Seville, Spain. E-mail: dmoreno@e-derma.org
E-health has had a major impact on the way patients with skin lesions are screened and diagnosed, and on how their treatment plans are implemented. Teledermatology (TD) and smartphone mobile applications have already made major contributions to improving accessibility to specialized dermatology units and prioritizing referrals to dermatologists for patients with a diagnosis of skin cancer. We describe here how a Spanish teledermatology network established by the skin cancer and melanoma unit in Seville has developed into a successful remote consultation network for patients in this region and discuss how mobile applications can be used by dermatologists, both as a training tool and in the remote management of patients with skin lesions.
TELEDERMATOLOGY: HOW TO INNOVATE IN THE MANAGEMENT OF SKIN CANCER
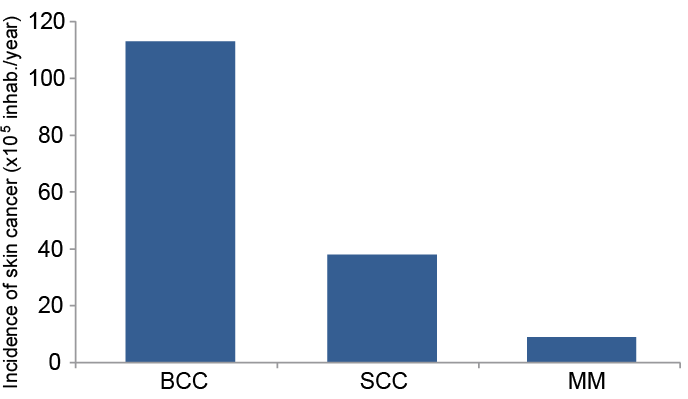
Skin cancer is by far the most common cancer. In Spain, the annual incidence of skin cancer is estimated at 160 cases per 100,000 inhabitants, representing a significant burden for the Spanish national health system (1). Al-though basal cell carcinoma (BCC) is the most frequent form of skin cancer, with a crude incidence of 113 cases per 100,000 person-years, compared with squamous cell carcinoma (SCC) and cutaneous melanoma (CM) (Fig. 1) it is also the least aggressive. In contrast, the rarer CM subtype is the most lethal form, being the leading cause of skin cancer mortality (1).
Fig. 1. Annual incidence of skin cancer subforms in Spain. BCC: basal cell carcinoma; SCC: squamous cell carcinoma; MM: malignant melanoma. Adapted from Tejera-Vaquerizo et al. 2016 (1).
Attempts to improve early management of skin cancer, from the initial consultation with the primary care physician to referral and initiation of treatment by the dermatologist, have concentrated exclusively on reducing waiting times for specialist consultation. However, this approach does not ensure correct prioritization or provision of the immediate response necessary to treat cancer successfully. Numerous specific programmes and fast-track referral systems were launched at the beginning of the century (2, 3). However, as highlighted by the evaluation of the UK 2-week referral system, these programmes repeatedly failed to show any benefit, mainly due to the lack of any clear criteria for referral of patients and the lack of appropriate training of physicians (4). We describe here how the implementation of a teledermatology network (TN) in a southern region of Spain has led to innovation in the management of skin cancer, reducing the public health burden of this frequent form of cancer whilst allowing personalized care in a local setting for the most vulnerable patients.
The TN was implemented in the southern region of Spain in 2004 with the aim of improving outcomes and management for skin cancer patients by providing a web-based connection between 56 primary care centres within a 100-km radius of the specialized skin cancer and melanoma unit of the Hospital universitario Virgen Macarena, Seville, Spain.
The TN led to clear changes in the way skin cancer was managed between the primary care centres and the skin cancer unit (Fig. 2): rather than referring all patients with suspicious lesions to the dermatologist, primary care physicians used the TN to send digital clinical photographs of the lesions to be assessed remotely by dermatologists at the skin cancer unit. These dermatologists then provided the physicians with a report and likely diagnosis, together with a final decision regarding the need for referral. The TN has developed into a highly effective routine screening programme for skin cancer in this region, allowing prioritized referral of patients with lesions of a high level of suspicion of malignancy.
Fig. 2. Patient management by the teledermatology network. AK: actinic keratosis.
The TN covers an area with over 800,000 inhabitants, resulting in more than 50,000 teleconsultations being managed by the system between 2004 and 2015. This has given rise to a mean work-load of 450 teleconsultations per month, with a mean response time of less than 3 working days (DMR, unpublished observation). The first validation studies of the system revealed that teledermatology results in a major reduction in waiting times for specialized opinion compared with the conventional letter referral system (Table I) (5). Pick-up rates for patients with any form of melanoma were also higher under the TD management system (Table I) and diagnostic accuracy was also found to be very high, with sensitivity reaching a mean of 0.99 (95% confidence interval; 95% CI) (5).
Table I. Key advances in the management of skin cancer patients associated with the teledermatology network compared with conventional teleconsultations
Further improvements in the management of skin cancer patients via the TN were observed with the introduction hand-held dermoscopes for use by the primary care physicians (dermoscopy teleconsultations, DTC), in addition to conventional digital cameras (conventional teleconsultations, CTC) (Fig. 2). Preliminary clinical trials revealed that use of DTC resulted in a significant reduction in the number of referrals for face-to-face consultations at the skin cancer and melanoma clinic compared with CTC (Table I) (6). The decreased referral rate for DTC compared with CTC was a consequence of the higher degree of diagnostic confidence associated with the dermoscopy images, together with increased diagnostic sensitivity (1.0 vs.0.6, p = 0.001) and specificity (0.09 vs. 0.81, p = NS) (Table I) (6). These major improvements to the TN system were achieved without causing any major increases in the length of consultations, with collection of dermoscopy images in addition to conventional clinical pictures adding only 1 min to consultation times for primary care physicians and only a few seconds for dermatologists (6).
In addition to the screening and prioritization of patients with skin lesions, we found that the TN could be used as a preoperative management tool for diagnosis in clear-cut cases, allowing direct referral and pre-surgical management of patients requiring surgery and reconstruction (Fig. 2). This pre-surgical teledermatology more than halved waiting times for surgery (Table I) (7). By allowing direct referral of patients to the surgical team, pre-surgical TD also reduced the number of hospital visits (at least two with the conventional system to only one with pre-surgical TD) and the number of on-the-day cancellations (Table I) (7). The level of accuracy of pre-surgical TD for predicting the type of surgery required was also found to be high, κ=0.75 (95% CI 0.71–0.79) (7). Pre-surgical TD has been shown to be very useful for providing personalized care to bed-ridden or handicapped patients, or elderly patients living far from the hospital. The TN allows physicians to fit the care they provide to the special needs of these vulnerable patients, thus ensuring that all patients receive the same level of specialized management, regardless of where they live or their personal circumstances.
Use of the TN can also be extended beyond screening and preoperative planning to therapeutic management of patients with conditions such as actinic keratosis (AK) (Fig. 2). In patients with a poor health status, treatment of clear-cut isolated or multiple AK lesions diagnosed via the TN has been initiated at the primary care centres. The TN allows detailed information on the treatment strategy and any potential side-effects to be transferred to the primary care physician, without the need for face-to-face consultations at the skin cancer and melanoma clinic. The therapeutic response and monitoring of side-effects has also been conducted entirely by TD in some cases, particularly when the personal circumstances of the patient have made visits to clinic problematic. The success of treatment management of AK by TD has led to a 2-fold increase in the number of patients with AK that we have opted to treat via TD over the past 5 years, from 254 in 2009 to 572 in 2015 (DMR, unpublished observation).
For any health solution to be feasible, efficient, and widely accepted by all users, complicated and expensive technology needs to be avoided and the systems deployed need to be simple and accessible with user-friendly software and devices. The TN uses a very simple straightforward platform and working procedure. For example, the platform used for AK is very user-friendly, with the only additional information recorded by the primary care physician being the time course of the lesion, whilst other data (age and sex of the patient) are automatically transferred from health system data. This simple, optimized platform allows dermatologists using the TN to manage approximately 50 teleconsultations per hour. Given that the main aim of the programme is to screen and prioritize patients for referral, dermatologists minimize the risk of misdiagnosis by always referring ambiguous cases for consultations at the clinic.
The TN has resulted in notable changes in the frequency of diagnosis of non-melanoma skin cancer (NMSC) and precancerous lesions, and in the stage at diagnosis of CM. Since the implementation of the TN in 2004, there has been a 2-fold increase in the number of patients diagnosed with BCC, with just 569 cases diagnosed in 2004 to 1,088 cases diagnosed in 2014 (8). This increase in NMSC has been accompanied by a rise in diagnosis of precancerous lesions (for example, AK) and a rise in consultations for seborrhoeic keratosis (DMR, unpublished observation), the lesion gives that rise to the greatest problems in the differential diagnosis of CM. In addition, the TN has had a positive impact on the prognosis of patients diagnosed with CM: mean Breslow thickness at initial diagnosis (the most critical prognostic factor for the outcome of CM) has been found to be lower in patients managed through the TN than in patients managed through the conventional referral system (Table I) (9). There was also found to be an increase in the number of patients with favourable prognosis at initial diagnosis associated with management by the TN compared with conventional systems (Table I) (9)).
The striking changes in the frequency of NMSC, occurring over the relatively short time-period of 10 years, are unlikely to reflect a true rise in the incidence of these lesions and are more likely a result of improved access to specialized diagnosis via the TN. Similarly, the TN appears to result in an increase in diagnosis of early-stage CM and precancerous lesions, leading to improvements in the prognosis for patients. As a consequence of improved detection rates of cancerous and precancerous lesions, the TN has also led to an increase in diagnosis of benign lesions, such as seborrhoeic keratosis.
In addition to specific programmes such as the TN described above, smartphone applications (mobile apps) and social media tools are also beginning to play a role in improving the management of patients with skin lesions. In 2005 the editor of JAMA Dermatology stated that “we are beginning to move away from clinic-pathologic diagnosis into an era of clinico-imaging diagnosis” in dermatology. Clinico-imaging diagnosis is now a part of daily practice for dermatologists, with much less need for skin biopsies and pathological studies. This major change in clinical practice can be attributed mainly to the widespread introduction of dermoscopy, and social media and smartphone apps into the daily clinical routine.
Although many dermatology apps are available, some apps are targeted for use by patients whilst others have been designed for use by dermatologists. Two mobile apps designed specifically for use by dermatologists, which may be useful in daily clinical practice, are VisualDx (https://www.visualdx.com/) and YouDermoscopy (http://www.youdermoscopytraining.org/). VisualDx is an affordable app that can be used in 2 ways. On the one hand, it can be used to search for information on given diseases, providing a summary of the key points of the disease, together with images, a synopsis of clinical signs, diagnostic tools, differential diagnosis, diagnostic tests, and management and therapy. On the other hand, it can be used to provide a list of possible diagnoses based on clinical signs (age of the patient, type of skin rash, location of the lesions, additional symptoms, onset, medical history etc.) entered by the dermatologist. YouDermoscopy is an application that was developed as a training tool for dermatologists and is now available worldwide. Users are required to correctly diagnose lesions on the basis of dermoscopy images. This app contains a series of levels, each containing a set of images requiring diagnosis within a 10-s interval. Users obtaining low scores are requested to retry the level, thus this tool provides an excellent example of how mobile apps can be used to increase knowledge and training in dermatology.
Other mobile apps have been developed recently with the aim of facilitating exchange of expertise between dermatologists and healthcare professionals worldwide. Skindiag is a mobile teledermatology app available free to registered users of the Pierre Fabre Dermo-cosmetique Club Dermaweb site (http://www.clubdermaweb.com/en). The app can be used to provide diagnostic and therapeutic assistance, with users able to submit a smartphone photograph and query to which 2 hospital experts will respond within 48 h, depending on the continent. Skindiag also allows dermatologists to discuss cases with their peers and consult cases archived by category for educational purposes.
In addition to apps designed for use by dermatologists and health professionals, many apps are designed for use by the patient. One such app is SkinVision (https://skinvision.com/), an application designed to be used by patients to check skin lesions, such a moles, for signs of cancer. Users provide an image of a skin lesion, which is analysed to provide an assessment of cancer risk. However, although this is the most popular app chosen by users searching with the term “melanoma”, evidence suggests that such automated diagnostic tools are unlikely to be efficient. MelaFind (MELASciences Inc, Irvington, New York, USA) was the first machine available on the market capable of making an automated diagnosis of melanoma. However, even this well-funded 20-year project resulted in a machine that detects 98.4% of melanomas, but with only 10% specificity (10). Automatic diagnosis is therefore not likely to be feasible for melanoma and these mobile apps should perhaps be treated with caution.
In addition to targeted dermatology apps, social media tools such as WhatsApp (https://www.whatsapp.com/) can also play an essential role in the remote management of patients with skin lesions. These tools allow images to be taken by patients and analysed remotely by dermatologists. Social media tools can therefore increase efficiency by decreasing the need for face-to face consultations for patients with clearly benign conditions. They can also serve to reassure patients by providing rapid expert opinions and can even be used to recommend topical treatments and monitor follow-up, without the need for patients to travel to the clinic. However, these social network tools have their limitations, for example patients with naevi and conditions requiring dermoscopy for accurate diagnosis should be routinely prioritized for clinical consultations.
The TN has shown that e-health is a highly successful approach for the management of patients with skin cancer, reducing waiting times and providing a rapid and reliable screening method that allows prioritization of patients with skin cancer requiring immediate treatment. The TN also makes specialized care available in local primary care centres, giving all patients access to the same level of care regardless of their general health status and personal circumstances. The TN has now managed over 50,000 teleconsultations and has played a critical role in improving the knowledge and diagnostic skills of primary care physicians in the field of dermatology. This combination of accessible care and well-trained local primary care providers has led to an increase in patients seeking care for skin lesions, patients who may otherwise never have sought specialist treatment. In addition to specific networks, mobile apps are already being used in dermatology, both by dermatologists and patients. These apps, combined with social media, which are at the forefront of the change to clinical imaging diagnosis of skin lesions, are likely to play an increasingly important role in the management of patients by teledermatology.
Medical writing services were provided by Emma Pilling and Marielle Romet (Santé Active Edition) and funded by Pierre Fabre Dermocosmetique.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize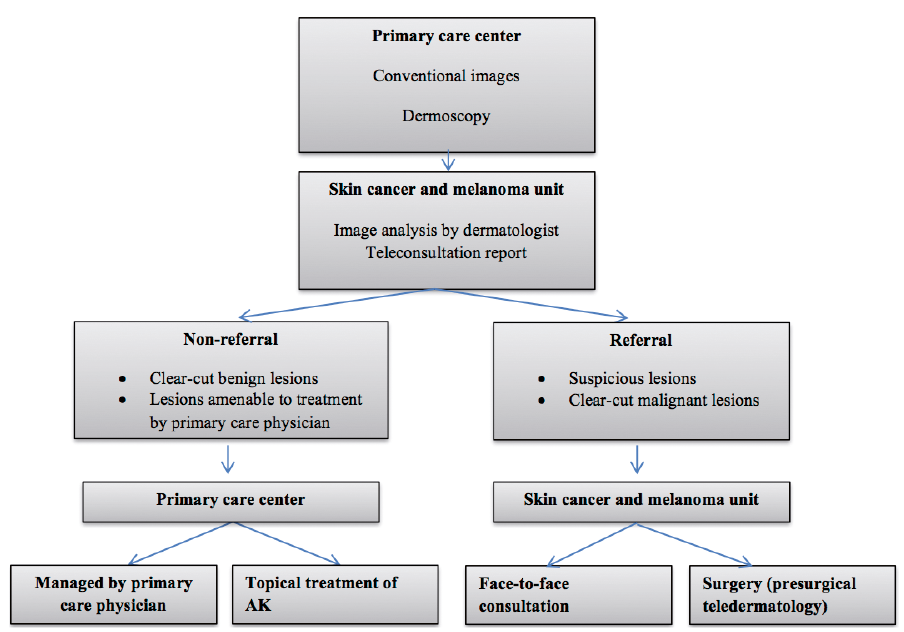 Click to show fullsize
Click to show fullsize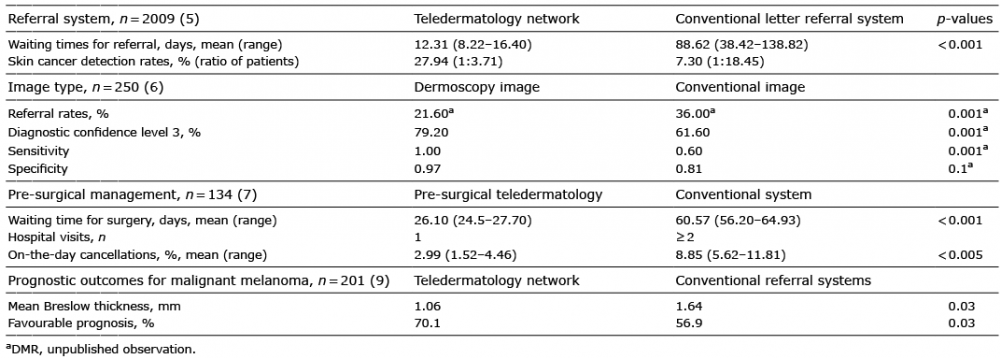 Click to show fullsize
Click to show fullsize