


Department of Dermatology and Allergology, University Hospital Jena, Jena, Germany
Granuloma faciale is an uncommon benign chronic dermatosis characterized by reddish-brown to violaceous asymptomatic plaques appearing predominantly on the face. The pathogenesis of granuloma faciale remains unclear, and it is frequently unresponsive to therapy. This systematic review aims to summarize all recent publications on the management of granuloma faciale. The publications are mainly individual case reports, small case series and a few retrospective studies. Treatment options included topical, intralesional and systemic corticosteroids, topical pimecrolimus and tacrolimus, topical and systemic dapsone, systemic hydroxychloroquine, clofazimine, and tumour necrosis factor-alpha inhibitors. More invasive therapies using lasers as well as cryosurgery and surgery were also reported. Topical glucocorticosteroids and tacrolimus remain treatments of first choice, possibly supplemented by topical dapsone.
Key words: tacrolimus; dapsone; review.
Accepted Sep 7, 2017; Epub ahead of print Sep 7, 2017
Acta Derm Venereol 2018; 98: XX–XX.
Corr: Claudia Lindhaus, Department of Dermatology and Allergology, University Hospital Jena, Erfurter Strasse 35, DE-07743 Jena, Germany. E-mail: Claudia.lindhaus@med.uni-jena.de
Granuloma faciale (GF) is an uncommon inflammatory dermatosis with characteristic clinical and histological features. The term granuloma faciale was coined by Wigley in 1945, referring to the condition as an eosinophilic granuloma of the skin (1). Clinically, GF presents as reddish-brown to violaceous plaques, often with follicular accentuation and superficial telangiectasias (2). Plaques are situated almost solely on the face, but occasionally may appear on the trunk, extremities, or in the nasal cavity (extrafacial GF) (3).
Diagnosis is confirmed by skin biopsy, which is often necessary to rule out other skin diseases with a similar appearance: rosacea, sarcoidosis, lupus vulgaris, fungal infection, mycobacteriosis, and discoid lupus erythematosus (2).
Erythema elevatum diutinum (EED) is an important differential diagnosis for GF, especially in its extra-facial presentation. Both lesions are variants of leukocytoclastic vasculitis. The main differences between them are clinical; therefore diagnostic difficulties are increased in atypical locations. EED manifests with multiple lesions on the extensor surface of the joints, while GF manifests typically with isolated lesions, predominantly on the face (4).
The histopathological diagnosis of GF may be challenging, as precise histopathological criteria have not been defined. Several features, such as the presence of many eosinophils in the infiltrate, are thought to be characteristic of GF. In a retrospective analysis of 66 patients and 73 skin specimens, Ortonne et al. (3) demonstrated that the most frequent histopathological features of GF were the presence of a grenz zone, infiltration of neutrophils, and telangiectasia. However, some features usually considered to be of diagnostic value for GF were absent in a proportion of cases. In particular, there were cases with absent or diminished numbers of eosinophils.
Although vascular changes appeared to be frequent, concentric fibrosis around small blood vessels may be demonstrated (4), but necrotizing vasculitis with vessel wall fibroid necrosis is rare, indicating that vessels may be involved in the pathogenesis of GF in a manner different from that seen in necrotizing vasculitis (3). Occasionally, the presence of IgG, IgA, IgM, C3c and C1q deposits surrounding cutaneous skin vessels in GF suggests that activation of complement via the classical pathway may participate in the development of vasculitis (5).
Acute and chronic features are often linked, which suggests that GF follows a chronic course with recurrent acute phases, rather than having distinct acute and chronic stages (3).
The pathogenesis of GF remains unclear. It has been suggested that it is mediated by interferon (IFN)-γ produced by CD4+ T-helper cells. In GF lesions, immunohistochemistry reveals a predominance of CD4+ lymphocytes, responsible for producing IFN-γ, a mediator that acts to express molecules such as ICAM-1 (intercellular adhesion molecule 1) on the surface of keratinocytes, promoting the chemotaxis of lymphocytes (6). Interestingly, in GF lesions, basal keratinocytes do not express ICAM-1, restricting the migration of inflammatory cells into the epidermis, and forming the characteristic grenz zone (6).
Further proposed, but yet unproven, factors that may contribute to the development of GF are hypersensitivity reactions, infection, trauma, actinic exposure, and radiation (4).
Management of GF may be difficult, with multiple topical, systemic and mechanical treatment regimens proposed, and variable clinical responses.
The aim of this review is to summarize recent experience in management of GF, in order to help other physicians choose a suitable treatment.
Applying the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (7) a systematic review was performed based on PubMed, Medline and Web of Science databases using the query “granuloma faciale and treatment”. The search was limited to “English” and “German” language, “human” subjects and publications from 1 January 2000 to 31 December 2016, documenting adequately the treatment for GF. Furthermore, the reference lists in the retrieved articles were searched manually to identify additional articles meeting the predefined inclusion criteria.
A total of 62 articles was identified from the initial PubMed search, and 5 additional articles were found via manual review. After searching Medline and Web of Science databases, no further articles were identified. After reviewing all full-text articles and reviews, papers about other diseases and articles that did not report on treatment, a total of 54 text sources, 49 from the initial search and 5 from additional papers, were analysed.
For each paper included, a summary of author, study year, number of patients, location and duration of lesions, therapies and efficacy results is given in Table SI; (8–58).
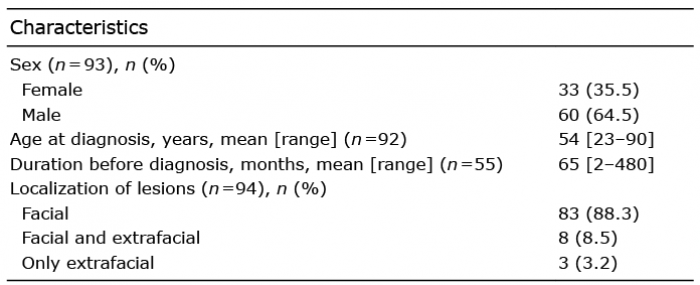
The results are based mainly on individual case reports, small case series and retrospective studies. Information on 94 patients was retrieved (61 males and 33 females), mean age at diagnosis 54 years, mean time before diagnosis 65 months, which is in keeping with published data. Facial localization outweighed extrafacial presentation (Table I).
Table I. Characteristics of 94 patients with granuloma faciale
GF is known to be difficult to treat. This has resulted in numerous therapy modalities, alone or in combination. Typically, topical treatments are used first, followed by systemic drugs and, in case of failure, more invasive procedures. There are occasional reports on clofazimine (59), psoralen plus ultraviolet A (PUVA) therapy (60), and tumour necrosis factor (TNF)-α antagonists (55). The most commonly reported therapies since 2000 are topical corticosteroids or tacrolimus, intralesional corticosteroids, dapsone, and physical interventions such as laser-therapy or cryotherapy. The treatment success for various interventions reported for > 5 patients is summarized in Fig. 1 and the results are discussed separately below.
Fig. 1. Overview of reported successful treatments in 5 or more patients.
Topical corticosteroids, either locally applied or as intralesional injections, are frequently used for treatment of GF. The results vary: in 42%, no effect was seen (Fig. 1), and skin atrophy is of major concern (10, 11, 14, 17, 19–21, 24, 27, 28, 30, 34, 36–38, 40, 41, 43–47, 49–54, 61).
Calcineurin inhibitors, such as the macrolide tacrolimus, decrease the upregulation of interleukin-2 and decrease T-cell activation. In consequence, T-cell activation leads to decreased production of IFN-γ. This may be an explanation for the efficacy of topical tacrolimus in treating GF. Tacrolimus 0.1% ointment applied twice daily seems to be the most valuable treatment option, all 28 reported patients benefitted from this topical treat-ment, and 19 showed excellent results (5, 16, 20, 25, 26, 32–34, 36, 37, 39, 45, 51, 54).
The effectiveness of topical dapsone 5% gel for treatment of GF has been demonstrated recently by Babalola et al. (49). If the efficacy is confirmed in a larger cohort, it may emerge as an important agent in GF treatment due to ease of use and low side-effects.
Dapsone, also known as diaminodiphenyl sulfone (DDS) is a sulfonamide antibiotic commonly used for treatment of GF at a dose of 50–150 mg daily. Although the mechanism of action of dapsone is not completely understood, it is thought to inhibit the activity of lysosomal enzymes, impede chemotaxis of neutrophils and eosinophils, and suppress inflammatory cytokines in the skin (62). The results of oral dapsone therapy vary (8, 9, 11, 23, 24, 30, 37, 44, 45, 50, 53, 55, 56, 61). Common side-effects mentioned in the summary of product characteristics (SPC) include nausea and loss of appetite. Severe side-effects may include haemolysis, methaemoglobinaemia especially in patients with glucose-6-phosphate dehydrogenase deficiency (G-6-PD), or hypersensitivity. Therefore monitoring of full-blood count and methaemoglobinaemia is mandatory. Further side-effects include hepatitis and various types of skin rashes (63).
Reports on systemic corticosteroid therapy are scarce, therefore dose regimens are given. However, the results are not convincing (11, 55, 56).
Clofazimine, an anti-leprosy drug with anti-inflammatory effects and anti-proliferative activity for lymphocytes and carcinoma cells, was reported to be successful by Gomez-de la Fuente et al. (10) at a dose of 300 mg daily for 5 months with remarkable clinical response.
Sand & Thomsen (55) reported on a single experience of 6-month treatment with adalimumab for GF in a male patient with large facial pigmented plaques without marked improvement.
Physical therapies, such as cryotherapy and laser therapy or surgical excision, may cause scarring or post-inflammatory pigmentation. In addition, recurrence of the condition may occur, or the treatment may not be successful in first place (41, 64).
Graham & Stewart (65) were the first to report the use of cryosurgery in 1977. Its effectiveness as the sole treat-ment for GF was subsequently reported by Panagiotopoulos et al. (28) using open-spray cryotherapy or contact technique. No significant side-effects were noted, and no recurrences were seen after a 2-year follow-up period. Mashood (27) reported excellent results in combining intralesional steroids with cryotherapy. Less successful results were reported by Firkle & Pizinger, who finally used 595-nm pulsed dye laser to clear the GF lesions (40).
Various types of laser, such as pulsed dye laser (PDL) (9, 40, 42, 66), potassium-titanyl-phosphate (KTP) laser (16) and carbon-dioxide (CO2) laser (61), have been applied, with different cosmetic results. However, the aesthetic outcome also depends on the operator, not only on the laser type and mode.
The PDL targets oxyhaemoglobin in blood vessels. Telangiectasia in GF suggests that this type of laser may be an effective treatment option. Good cosmetic results with 595-nm PDL are expected in flat lesions, as the low depth-penetration of these wavelengths will not be able to significantly improve severe exophytic GF.
Hruza & Amarati (42) have stressed the need for high energies, sometimes with pulse stacking, to achieve clearance using PDL. Achieving deep purpura appeared to be important for the effectiveness of the PDL. By changing pulse durations and energies, most patients’ lesions cleared in 2–3 treatments. Some patients’ lesions recurred after 1–3 years, or they developed adjacent or new lesions.
Ludwig et al. (16) used a KTP 532-nm laser because of its known success in the treatment of vascular lesions. They achieved persistent clinical resolution without scarring, permanent pigmentary alteration or systemic morbidity.
CO2 lasers target tissue water and vaporize tissues in a non-selective manner. They carry a higher risk of scarring or hypopigmentation. Bakkour & Madan (50) successfully treated a rhinophyma-like GF with a CO2 laser.
Due to the low incidence of GF, controlled clinical trials do not seem feasible, and it is likely that we will continue to depend on information gained from case reports. Dermatologists should therefore be encouraged to share experiences regarding the management of GF in future publications.
Based on published treatment successes experienced in a minimum of more than 5 patients (Fig. 1), we suggest starting the treatment topically. Tacrolimus 0.1% ointment applied twice daily seems to be the most successful option. A trial with local dapsone gel is a further option that needs to be evaluated.
Cryotherapy is inexpensive and widely accessible, but its effect is limited.
Systemic dapsone therapy is usually well tolerated at a dose of 100 mg daily; however, severe side-effects may occur, patients should be well counseled and followed-up.
Based on our own experience, we suggest the use of laser, preferably PDL laser if available, as the treatment of choice for drug-resistant GF.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize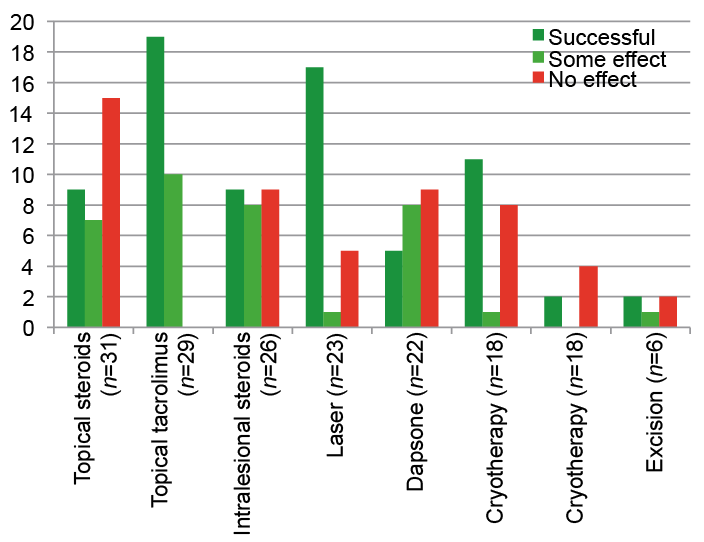 Click to show fullsize
Click to show fullsize