


1Centre for Population Health Sciences (CePHaS), Lee Kong Chian School of Medicine, Nanyang Technological University, Singapore, Singapore, 2Global eHealth Unit, Department of Primary Care and Public Health, School of Public Health, Imperial College London, London, 3Division of Population Medicine, Cardiff University School of Medicine, Health Park, Cardiff, UK, 4Dermatology and Skin Biology Programme, Lee Kong Chian School of Medicine, Nanyang Technological University, 59 Nanyang Drive, Experimental Medicine Building, Singapore 636921, Singapore, and 5Division of Dermatology, Department of Clinical Sciences, Lund University, Lund, Sweden. *E-mail: artur.schmidtchen@ntu.edu.sg
Accepted Sep 7, 2017; Epub ahead of print Sep 7, 2017
The term “chronic wound” was first used in the literature in the 1950s, to refer to wounds that were difficult to heal or did not follow a normal healing process (1, 2). However, the term has met criticism for its uncertainty regarding the duration of chronicity (3). Various alternative terminologies have been suggested, such as hard-to-heal wounds, difficult to heal wounds, non-healing wounds and complex wounds (4, 5). “Chronic wounds” are commonly defined as “wounds that have not proceeded through an orderly and timely reparation to produce anatomic and functional integrity after 3 months” (6). However, Martin & Nunan (7) defined a “chronic wound” as a barrier defect that has not healed in 3 months, and Leaper & Durani (8) defined it as a wound that lacks a 20–40% reduction in size after 2–4 weeks of optimal treatment or when there is not complete healing after 6 weeks. Recent reviews have also highlighted the lack of consensus regarding the definition of a “chronic wound” and the need for further research in this area (9, 10).
The increasing prevalence of non-communicable diseases and the ageing population have put the spotlight on wound care and the considerable societal burden of wounds (11, 12). However, the lack of a common terminology when sharing and applying scientific research implies a risk of inaccuracy, with serious consequences for patients with wounds. For instance, the great disparity in the definitions of “chronic wounds”, leading to only a few studies being included in 2 systematic reviews (3, 9), may, at a later stage, have a negative impact on the management and care of “chronic wounds”. Moreover, the undefined terminology may also hamper future comparisons between separate clinical retrospective or prospective studies.
The aim of this study is to highlight the wide heterogeneity in the definitions and reference staging of “chronic wounds”, and along with the review by Gould et al. (9), discuss this problem according to category of wound.
Based on the published search strategy applied in a systematic review on the prevalence of chronic wounds (13), we reviewed the full-text of the included titles (in the title/abstract stage) for the definition of chronic wounds used by the different authors. We classified the studies, by aetiology, into the following groups: pressure ulcers (PU), venous ulcers (VU), arterial insufficiency ulcers (AIU) and diabetic foot ulcers (DFU), implying also that studies on ulcers of mixed aetiologies were excluded, as the purpose was to describe chronicity by ulcer group.
A total of 669 articles on chronic wounds that met the review criteria (13) were identified (Fig. S1), of which 400 articles corresponded to PUs (60%), 238 to DFUs (36%), and 28 to VUs (4%) (despite this being one of the most common causes of chronic wounds), and 3 to AIUs.
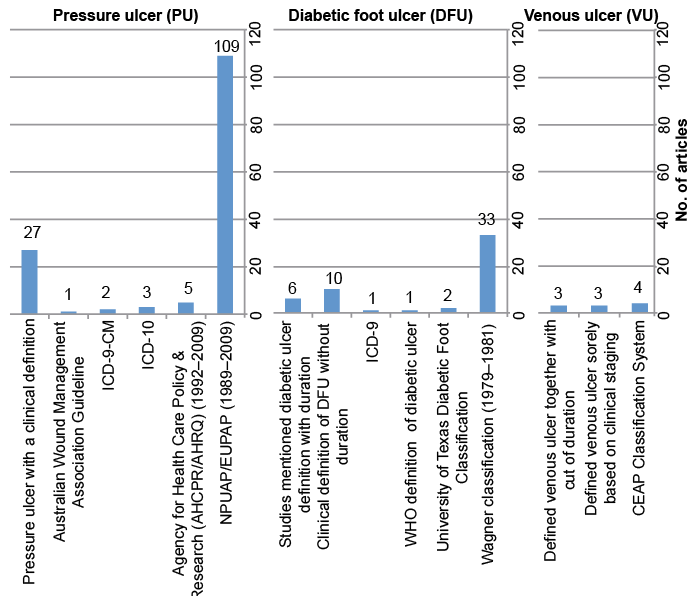
Sixty-three percent of the articles describing PUs did not provide a definition or a staging system. One hundred and forty-seven articles (37%) provided either a reference staging system or a definition. Details are shown in Fig. 1. No studies mentioned the duration of chronic PU in their definitions.
Fig. 1. Number of articles on pressure ulcers, diabetic foot ulcers and venous ulcers that provided a definition or a reference staging system.
Only 53 of 238 articles on DFUs provided a definition or a staging system, of which 33 (22%) used the Wagner classification of diabetic ulcer (1979–1981) without providing any information on the duration (Fig. 1). Only 6 articles provided duration in their definition of a chronic DFU, with a cut-off range for defining chronicity varying from 2 to 8 weeks.
Of the 28 papers on VUs, 10 (36%) used a staging system or provided a definition. The most commonly cited classification system was Comprehensive Classification System for Chronic Venous Disorders (CEAP), which was cited in 4 papers without any specified duration of the ulcer. Another 3 articles defined VU based exclusively on clinical and pathophysiological findings. Only 3 articles defined VU using the duration of the ulcer as part of their definitions, applying a range from 6 weeks to 2 months. Two of the 3 articles on AIUs cited the Rutherford grading system for the definition without integrating the duration in their definitions.
This study examined the preliminary stages of including articles in a systematic review on prevalence of “chronic wounds” of different aetiologies (13) in order to assess the uniformity, or lack of it, in defining the duration of “chronic wounds” as a factor of importance to healing (14). Most papers did not provide a clear cut-off duration to define the chronicity of wounds in the categories of PU, DFU, VU and AIU. Those papers that did include a specific duration in their definitions, did not agree on the timeline that defines an ulcer as chronic. For papers on DFU, an ulcer lasting 2–8 weeks was classified as chronic, in stark contrast to VUs, where chronicity was defined when ulcers were present for at least 6 weeks to 2 months. PUs and AIUs did not include duration in any of the reviewed papers.
A comprehensive definition of “chronic wounds” is essential in order to enhance patient care and strengthen the clarity of management guidelines. This new definition may include several clearly stated components adding to the actual duration of the wound, and take into account the aetiology of the wound. In addition, a scoring system for chronic wounds should be introduced, including characteristics such as recurrence, patient’s age and sex, comorbidities, etc. for better informing patient management and improving transfer of new research findings. It is of note that such scoring and diagnostic criteria are used in the diagnosis and definition of other diseases, as exemplified by psychiatric diseases, or various inflammatory diseases, such as systemic lupus erythematosus or multiple sclerosis. The diagnostics within wound care would also significantly benefit from increased agreement regarding definitions. International disease coding systems, such as the International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10), could eventually also include codes separating acute and chronic wounds in order to support better tailored treatments.
This research was supported by the A*STAR BMRC Strategic Positioning Fund (SPF) for Skin Biology awarded to the Institute of Medical Biology, and Lee Kong Chian School of Medicine, Nanyang Technological University Start-Up Grant.


 Click to show fullsize
Click to show fullsize