


1Department of Dermatology, and 2Department of Transplant Surgery, Hokkaido University Graduate School of Medicine, N15 W7, Sapporo 060-8638, Japan. *E-mail: natsuga@med.hokudai.ac.jp
Accepted Oct 2, 2017; Epub ahead of print Oct 3, 2017
A syringoma is a benign appendageal neoplasm that typically presents in adolescent females. Clinically, syringomas appear as multiple small papules with symmetrical distribution and are normal skin-coloured or slightly pigmented. The 4 subtypes of syringoma are classified according to their clinical features: localized, familial, Down’s syndrome-associated and generalized (encompassing eruptive syringoma) (1–4). The eruptive variant of syringoma, which is observed less commonly than other subtypes, is 1–5 mm in size and is predominantly distributed over the anterior trunk, neck, abdomen and axillae (2, 3). We present here a case of a 70-year-old woman with extensive eruptive syringomas that developed after deceased donor liver transplantation (DDLT).
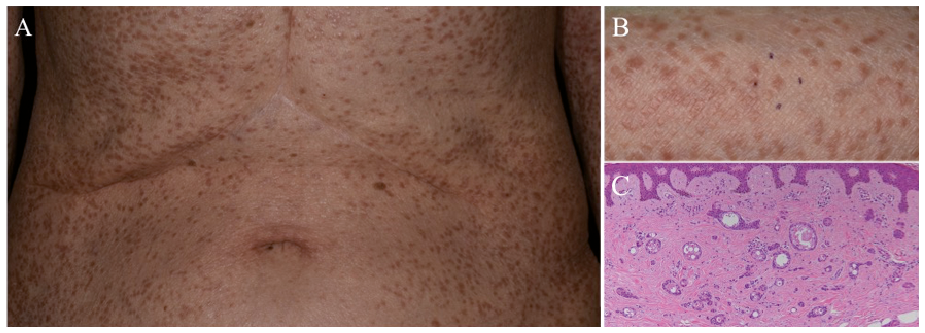
A 70-year-old Japanese woman was referred to our department with an 11-year history of papules on the trunk and upper limbs. The lesions appeared soon after DDLT for her primary biliary cirrhosis and subsequent immunosuppressive therapy (tacrolimus hydrate, myco-phenolate mofetil and corticosteroids). No exacerbation or spontaneous remission had been observed during the 11 years. There was no family history of similar eruptions. Physical examination revealed multiple light-brown papules up to 7 mm in diameter disseminated on the trunk and upper extremities (Fig. 1A). There were no eruptions on the lower extremities, the oral mucosa or the genital area. Physical examination revealed no other significant symptoms, and laboratory results were unremarkable. In light of the immunosuppressive background, she was initially suspected of having verruca plana. Histological examination of a biopsy specimen from a papule on the right forearm (Fig. 1B) revealed multiple small ducts embedded in fibrous stroma. The ducts were lined by 2 layers of epithelial cells and were filled with accumulated eosinophilic secretions. Some of the cells had a tadpole appearance (Fig. 1C). These findings led to a diagnosis of eruptive syringoma.
Fig. 1. (A) Clinical presentation. Multiple brown papules distributed on the trunk and upper extremities. (B) A skin biopsy was performed from a papule on the right forearm. (C) Pathology of the biopsy specimen. The specimen reveals multiple small ducts embedded in fibrous stroma. Some of the cells show a tadpole appearance (haematoxylin and eosin staining, original magnification ×100).
Since syringoma eruptions appear as non-specific papules, clinical diagnosis of eruptive syringoma can be difficult. The differential diagnoses include xanthoma, verrucae, mastocytosis, milia, lichen planus, disseminated molluscum contagiosum and viral-related trichostasis spinulosa. The diagnostic difficulty of the present case owed to the fact that the patient was referred 11 years after liver transplantation and each lesion was larger than a typical syringoma. Although the pathogenesis of eruptive syringoma remains unknown, some studies have suggested an association between syringomas and inflammatory reactions, such as contact dermatitis and drug hypersensitivity (4, 5). To our knowledge, this is the first case of eruptive syringoma occurring after liver transplantation. Apart from the current case, a case of eruptive syringoma that developed after kidney transplantation has been reported (6). These 2 cases might imply the involvement of immunosuppression in the pathogenesis of syringomas, in contrast to the previous speculation of inflammatory reactions (4, 5). A study that showed a greater incidence of adnexal skin tumours in organ transplant recipients than in immunocompetent individuals (7) corroborates the role of immunosuppression in syringoma development. When multiple asymptomatic pigmented papules are observed in immunosuppressed patients, eruptive syringoma can be included on the list of differential diagnoses.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize