


1Department of Preventive Medicine, Korea University College of Medicine, Seoul, and 2Department of Dermatology, Incheon St Mary’s Hospital, College of Medicine, The Catholic University of Korea, Incheon, Korea
Treatment of vitiligo is challenging and requires a multidisciplinary approach. Fractional carbon dioxide (CO2) laser as an add-on to conventional treatment has been reported to be effective, but there is no consensus on its use. A systematic review was performed by searching major databases for relevant publications to February 2017. Six studies with 85 participants were included. For those with refractory vitiligo, the addition of fractional CO2 laser to routine treatment modalities was superior to conventional treatment alone in terms of > 50% re-pigmentation (risk ratio (RR) 4.90, 95% confidence interval (95% CI), 1.15–20.93; p = 0.03), physician improvement score (mean difference (MD) 0.81, 95% CI 0.33–1.29; p < 0.001), < 25% re-pigmentation (RR 0.64, 95% CI 0.49–0.85; p=0.002) and patient satisfaction (MD 1.61, 95% CI 0.73–2.49; p < 0.001). Side-effects were minor. These results provide evidence supporting that fractional CO2 laser is a valuable treatment modality for patients with vitiligo, especially for those with refractory vitiligo.
Key words: fractional CO2 laser; add-on treatment; vitiligo; refractory vitiligo; systematic review; meta-analysis.
Accepted Nov 2, 2017; Epub ahead of print Nov 9, 2017
Acta Derm Venereol 2018; 98: XX–XX.
Corr: Hei Sung Kim, Department of Dermatology, Incheon St. Mary’s Hospital, The Catholic University of Korea, 56 Dongsuro, Bupyeong-gu, 150-713, Incheon, Korea. E-mail: hazelkimhoho@gmail.com
Vitiligo is a common skin disease with an estimated prevalence of 0.5–2% worldwide. It is characterized by melanocyte loss, which results in patchy depigmentation of the skin and hair. The white patches impose immense psychological burden, and as a result, there is high demand for treatment. Existing treatments include topical and systemic immune-suppressants, phototherapy and surgical techniques that serve to halt the disease progression, stabilize depigmented lesions, and encourage re-pigmentation (1). Combination of treatment modalities often yields better results than monotherapy, and thus various combinations have been tried to enhance treatment efficacy.
Despite numerous available treatment options, a high proportion of patients with vitiligo have resistant disease (2). Therefore, new therapeutic approaches are required.
Lasers are a popular treatment modality for a myriad of dermatological conditions. In recent years, fractional CO2 laser has been introduced as an add-on treatment for vitiligo (3–12). Fractionated ablative laser represents a new modality for skin resurfacing based on the theory of fractional photothermolysis (13). It is efficient in treating facial photo-aging and scars, and has an improved safety and recovery profile compared with traditional CO2 laser resurfacing. The beneficial effect of fractional CO2 laser on vitiligo is postulated to come from the release of cytokines and growth factors that act as mitogens for melanogenesis (3). The preceding laser also alters the skin barrier, which results in increased penetration of topical drugs and ultraviolet (UV) radiation (4).
While the use of fractional CO2 laser followed by narrow-band ultraviolet B (NB-UVB), sunlight exposure, or topical agents has demonstrated promising results, there is lack of firm evidence on its potential in vitiligo due to the absence of sufficiently powered randomized controlled trials. Through systematic review of the literature, the aim of this study was to investigate the effectiveness and safety of fractional CO2 laser as an add-on treatment, in patients with vitiligo.
Systematic review and meta-analysis were conducted and reported in accordance with the PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analysis) statement (14).
The review was performed on studies that investigated the effect of fractional CO2 laser in vitiligo. In order to collect all available evidence, EMBASE (1988 to present), MEDLINE (1946 to present), Web of Science (1975 to present), Scopus (1996 to present), and Cochrane Central register of Controlled Trials (CENTRAL) (1991 to present) databases were searched on 9 February 2017, without limitation in terms of dates or language. To search for studies of fractional CO2 laser, the following keywords were used: [“fractional” or “carbon dioxide” or “CO2” or “gas”] and [“laser” or “lasers”]. To search for vitiligo, the following keyword was used: “vitiligo”. The full search strategy in Appendix S1 was developed for MEDLINE and was tailored to the other electronic databases.
Inclusion criteria were: original reports (trial studies, case series, items of correspondence, posters, and meeting abstracts) which compared the effect of fractional CO2 laser plus conventional therapy with that of conventional therapy alone in vitiligo (in humans). All vitiligo subtypes were included in this systematic review. According to the pre-defined criteria, 2 authors (HJK and HSK) independently selected reports based on the title and abstracts. Any discrepancies were resolved in consultation with a third party (ESH). The 2 authors then examined the full texts of those reports. Duplicate publications were identified by several criteria (authors, title, intervention characteristics, and number of patients). In case of duplicates, the most complete report was chosen. Randomized controlled trials (RCTs) that used the quartile grading scale for assessment (grade 0, no improvement; grade 1, 1–25% re-pigmentation; grade 2, 26–50% re-pigmentation; grade 3, 51–75% re-pigmentation; grade 4, >75% re-pigmentation) were included in meta-analysis.
For each selected report, 2 authors (ESH and HSK) independently extracted information on the first author, publication year, country/setting, study design, vitiligo subtype and duration, characteristics of patients, details of the treatment measures (fractional CO2 laser, conventional treatment), and outcome (efficacy and side-effects). Any disagreement was resolved by discussion. A data table was established for each study. The extraction table was developed by 3 dermatologists (CSH, LJD and KHS) who are familiar with vitiligo. For missing data, the first author of the report was contacted when possible. An intention-to-treat analysis was planned, and drop-outs were included in the analysis, if possible.
The risk of bias and methodological quality were assessed as outlined in the Cochrane Handbook for Systematic Reviews of Interventions (15). For RCTs, we used Cochrane Collaboration’s “risk of bias” tool. We adopted the Newcastle-Ottawa Scale for other study designs. The magnitude of effect and quality of evidence for each outcome were assessed. Two investigators (HJK and HSK) independently assessed the methodological quality of each study. Any disagreement was resolved by consensus or by consultation with a third investigator (ESH). Publication bias was not assessed due to the small number of studies.
Our primary outcomes were treatment success, defined as more than 50% re-pigmentation of each designated patch or whole lesion in a patient, and physician improvement score (mean ± SD, 0–4). The secondary outcome was treatment failure, defined as re-pigmentation of 25% or less of each designated patch or whole lesion in a patient, and the patients’ overall satisfaction score (VAS, 0–10).
Meta-analysis was conducted using Review Manager (RevMan) Version 5.2 (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark). We conducted pooled analyses using the Mantel-Haenszel method with random-effects weighting. Dichotomous data was assessed using risk ratio (RR) with 95% confidence interval (CIs). Continuous outcomes were analysed using the mean difference (MD) or, when different studies used different scales, the standardized MD. Heterogeneity of the trial results were assessed by virtually examining the forest plot to detect non-overlapping CIs, using the χ2 test of heterogeneity (with p < 0.1 indicating statistical significance) and the I2 statistic of inconsistency (with 30–60% denoting moderate, > 60% high levels of heterogeneity).
The literature search yielded 222 relevant articles. After removing duplicates, 135 records remained. Ten full articles were retrieved for further evaluation after screening the titles and abstracts. Six studies satisfied all selection criteria and were included in this review. Meta-analysis was performed on 4 studies (Fig. S1) (3–6).
Characteristics of the included trials are summarized in Table SI and Table SII. A total of 85 patients with vitiligo were included. All study patients were adults; 67.9% were women and 32.1% were men. Of the 6 trials, 2 were from Thailand (4, 5), and 1 from each of the following countries: Brazil (6), Iran (8), Lebanon (7) and Korea (3). Five studies adopted the quartile grading scale for clinical assessment (3–7). The mean disease duration varied from 3.6 to 16.8 years. Five studies recruited patients with refractory vitiligo (3, 4, 6–8) and one was on facial vitiligo (5).
The regimens for both the treatment arm (fractional CO2 laser + conventional treatment) and control arm (conventional treatment alone) differed among studies. As for fractional CO2 laser treatment, the total number of treatment varied from 1 to 10 sessions, with the treatment interval ranging from 1 week to 2 months. The common laser settings were as follows: pulse energy 100 mJ, spot density 150–200 spots/cm2, 2 passes over the assigned area. Conventional treatment included topical agents (topical steroid, topical salicylic acid), UVB (NB-UVB, targeted broadband UVB), sun exposure, and autologous hair transplant in a number of combinations. Treatment duration ranged between 2.5 and 5 months and assessments (by physicians and patients) were made 2–3 months after the final treatment. Of the 6 studies included, 5 were RCTs (3–6, 8). One trial did not have a randomized design (7). The quality of the studies evaluating fractional CO2 laser as an add-on to vitiligo varied, but was generally poor (Fig. S2).
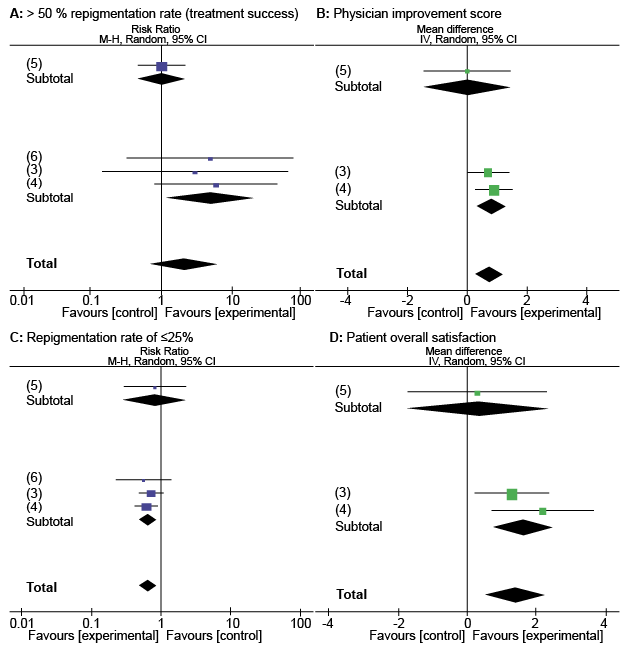
Four RCTs (3–6) assessed the outcome of greater than 50% re-pigmentation rate (treatment success rate), physician improvement score, and re-pigmentation rate of 25% or less (treatment failure rate). Subjects had refractory vitiligo in 3 studies (3, 4, 6), and 1 study consisted of patients with facial vitiligo (5). In terms of treatment success, pooled analysis showed a RR of 2.1 between the treatment and control group (4 studies; 95% CI 0.67–6.61; p = 0.21). Subgroup analysis according to vitiligo subtype (“refractory vitiligo” vs. “facial vitiligo”) identified a RR of 4.9 on treatment success with fractional CO2 laser add-on for refractory vitiligo (3 studies; 95% CI 1.15–20.93; p = 0.03) and a RR of 1 for facial vitiligo (1 study; 95% CI 0.45–2.23; p = 1.0). The overall heterogeneity was I2 = 33% (p = 0.21) and the heterogeneity within the refractory vitiligo subgroup was I2 = 0% (p = 0.93). The difference between the 2 subgroups was I2 = 71.6% (p = 0.06) (Fig. 1A).
Fig. 1. Efficacy of fractional carbon dioxide (CO2) laser add-on to facial (5) and refractory (3, 4, 6) vitiligo. (A) Treatment success greater than 50% re-pigmentation rate, (B) physician improvement score, (C) re-pigmentation rate ≤ 25%, (D) patient’s overall satisfaction. Favours on the x-axis; [control] represents conventional treatment alone and [experimental] denotes fractional CO2 laser add-on to conventional therapy. CI: confidence interval. References in parentheses. M-H: Mantel Haenszel Method; IV: inverse variance.
As for physician improvement score, quantitative synthesis including meta-analyses was not possible for 1 RCT study (6) because the mean and SD of its control group was 0. Pooled results showed a MD of 0.74 in physician improvement score between the treatment and control group (3 studies; 95% CI 0.28–1.19; p = 0.002). Subgroup analysis according to vitiligo subtype identified a MD of 0.81 on physician improvement score with fractional CO2 laser add-on for refractory vitiligo (3 studies; 95% CI 0.33–1.29; p < 0.001) and a MD of 0 for facial vitiligo (1 study; 95% CI –1.48–1.48; p = 1.0). The overall heterogeneity was I2 = 0% (p = 0.55) and the heterogeneity within the refractory vitiligo subgroup was I2 = 0% (p = 0.69). Difference between the 2 subgroups was I2 = 4.5% (p = 0.31) (Fig. 1B).
The overall RR of treatment failure was 0.65 between the treatment and control group (4 studies; 95% CI 0.50–0.85; p = 0.002). Subgroup analysis identified a RR of 0.64 on treatment failure with fractional CO2 laser add-on for refractory vitiligo (3 studies; 95% CI 0.49–0.85; p = 0.002) and a RR of 0.8 for facial vitiligo (1 study; 95% CI 0.28–2.27; p = 0.68). The overall heterogeneity was I2 = 0% (p = 0.90) and the heterogeneity within the refractory vitiligo subgroup was I2 = 0% (p = 0.81). The difference between the 2 subgroups was I2 = 0% (p = 0.69) (Fig. 1C).
Three RCTs (3–5) assessed the patients’ overall satisfaction with a 10-point VAS. Subjects had refractory vitiligo in 2 studies (3, 4), and one study consisted of patients with facial vitiligo (5). The overall MD in patient satisfaction was 1.40 between the treatment and control group (3 studies; 95% CI 0.53–2.27; p = 0.002). Subgroup analysis identified a MD of 1.61 in patient satisfaction score with fractional CO2 laser add-on for refractory vitiligo (2 studies; 95% CI 0.73–2.49; p < 0.001) and a MD of 0.30 for facial vitiligo (1 study; 95% CI –1.74–2.34; p = 0.77). The overall heterogeneity was I2 = 11% (p=0.32) and the heterogeneity within the refractory vitiligo subgroup was I2 = 0% (p = 0.34). The difference between the 2 subgroups was I2 = 25.2% (p = 0.25) (Fig. 1D).
Adverse events were identified in all studies (see Table SII). Fractional CO2 laser add-on to conventional vitiligo treatment caused transient pain, erythema, oedema, post-laser crust, tiny brown spots on the nail plate and slight oozing of the treated area. Most symptoms were relieved within a day and post-laser crusting disappeared within a week. None of the studies reported serious adverse events, such as infection, scarring, Koebner phenomenon or aggravation of vitiligo.
Vitiligo remains a great challenge in the field of dermatology with no definitive cure (16). Psychological distress is profound (17), particularly in those with dark skin, due to the distinct colour contrast. Not surprisingly, all our participants had coloured skin (Fitzpatrick type III–V) (see Table SI).
At present, no medical treatment for re-pigmenting vitiligo is approved by the US Food and Drug Administration (FDA), and therefore treatments are used off-label (1). NB-UVB phototherapy is currently the first-line therapy for vitiligo (5, 18). However, there is a risk of deep tanning, burning, and skin ageing from intense UV radiation exposure. Various drugs including topical steroids and topical calcineurin inhibitors have been used in combination with NB-UVB to increase the efficacy of re-pigmentation while reducing the cumulative UV doses (19, 20).
With the available treatment options, a satisfactory response has been observed in the face and neck area. In contrast, the acral parts of the extremities are often recalcitrant to treatment, which is due to the lower hair density in these areas compared with the head and neck region, with the paucity of follicular melanocytes (21, 22).
An increasing number of reports have highlighted the value of lasers, which includes fractional CO2 laser, in the treatment of vitiligo (3–12, 16). Lasers have an advantage of selective application, which blocks unnecessary irradiation to uninvolved skin. Thus, laser treatment should be a reasonable option for localized vitiligo.
Ablative fractional laser does not affect the entire epidermis, but leaves intact skin between the coagulated necrotic columns (13). This characteristic facilitates the skin healing process and also minimizes the side-effects (7, 9, 23, 24). Fractional CO2 laser has been suggested to improve vitiligo by the following mechanisms. First, it produces immediate tissue contraction (shrinkage), which narrows the size of the vitiligo lesions (25). Secondly, there is secretion of cytokines and various growth factors during wound healing, which may serve as mitogens for melanocytes from adjacent normal skin and hair follicles (16, 26). Thirdly, fractional laser promotes trans-epidermal penetration of UV and topical agents, enhancing their effect (5, 9, 16).
The aim of this review was to determine whether the practice of adding fractional CO2 laser to conventional treatment (i.e. phototherapy, topical agents, surgical grafts) is justified in vitiligo patients. Also, we opted to determine whether there is any difference in response between “refractory vitiligo” lesions and “vitiligo in general” (“refractory vitiligo” + “facial vitiligo”; further termed vitiligo) to fractional laser.
The results of this meta-analysis show that fractional CO2 laser add-on is more effective than conventional therapy alone for vitiligo, with regards to treatment failure (RR 0.65; 95% CI 0.50–0.85; p = 0.002), physician assessment (MD 0.74; 95% CI 0.28–1.19; p = 0.002), and patient report (MD 1.40; 95% CI 0.53–2.27; p = 0.002). The 3 outcomes were similar for refractory vitiligo (Fig. S3).
As for treatment success, the benefit of adding fractional CO2 laser was not found statistically significant for vitiligo as a whole (RR 2.1; 95% CI 0.67–6.61; p = 0.21). However, further subgroup analysis showed that fractional CO2 laser add-on is, in fact, greatly beneficial to those with refractory vitiligo (RR 4.9; 95% CI 1.15–20.93; p = 0.03) (Fig. S3). The difference between the “refractory vitiligo” and “facial vitiligo” subgroups (I2 = 71.6%; p = 0.06) was significant, which explains the discrepancy in findings between the “vitiligo” and “refractory vitiligo” population. So, why are the outcomes of treatment success different between “refractory” and “facial vitiligo”? An explanation is that vitiligo on the face often yields good enough response to conventional treatment. In such cases, fractional CO2 laser add-on would not offer further benefit. However, with only one study on facial vitiligo, the limited effect of fractional CO2 laser add-on to facial vitiligo should be interpreted with caution.
The 2 studies that were not available for meta-analysis also showed that there was better improvement on the fractional CO2 laser treated areas (Table SII).
In terms of side-effects, fractional CO2 laser was generally well-tolerated. In addition, skin atrophy or telangiectasia was not reported despite the likelihood of increased steroid absorption. Due to the possibility Koebner response (skin lesions appearing on sites of trauma) with vitiligo (22), fractional CO2 laser should not be applied to patients with active vitiligo.
This study has several limitations. First, with sham treatment simulating fractional CO2 laser therapy being unavailable, the study patients were not blinded. This would have affected the patients’ overall satisfaction score. Secondly, the true benefits of fractional CO2 laser may not have been captured because of the insufficient sample size or the limitations of the available outcome measures. Thirdly, our pre-emptive decision to pool data from studies with different vitiligo subtypes, fractional CO2 laser devices and variations in treatment algorithm (in terms of fluence, number of treatment sessions, treatment intervals, concurrent treatments, etc.) created some heterogeneity. This was partially resolved by performing additional analyses according to vitiligo subtype. Despite these limitations, our systematic review and meta-analysis does provide a snapshot of the best level of evidence currently available on fractional CO2 laser use in the management of vitiligo.
This systematic review and meta-analysis provides evidence supporting that fractional CO2 laser is a valuable treatment modality for patients with vitiligo, especially for those with refractory vitiligo. Further large-scale RCTs are warranted to identify the optimal fluence and treatment schedule (i.e. length of treatment, treatment interval, co-treatments) of fractional laser. Considering the difficulties in complete re-pigmentation of vitiligo, fractional CO2 laser would be most promising when combined with conventional therapy. However, clinical trials evaluating the efficacy of fractional laser alone should also be performed to identify its true effect on vitiligo.
This study was supported by a grant from the Korean Healthcare technology R&D project, Ministry of Health & Welfare, Republic of Korea (grant number HN15C0105).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize