


1Department of Dermatology, CHRU, Tours, 2General Practitioner, Loches, 3Department of Nephrolology, and 4Department of Dermatology, University of Tours, France. *E-mail: machet@univ-tours.fr
A 68-year-old woman was referred for specialized nail consultation in January 2018 due to a painful toe that had developed 2 months previously (Fig. 1). Pain had developed after walking for 2 h in the countryside, and a blister was seen on the toe in the evening, which the patient thought was a mechanical blister. However, the evolution was unusual, with persistent pain and discoloration of the affected toe. The general practitioner suspected infection and treated with oral antibiotics (pristinamycin, 2 g/day), with no effect. Subsequent treatment with colchicine, 1 mg/day, did not alleviate the symptoms. Doppler examination of the lower-limb arteries was normal. Radiography of the affected toe did not reveal osteitis.
The patient had a history of arterial hypertension treated with perindopril, 5 mg/day, for 2 years and with enalapril, 10 mg/day, and lercanidipine, 10 mg/day, for 3 months. She had never smoked.
Skin examination revealed red-bluish discoloration of the distal part of the 5th left toe, with nail dystrophy. Palpation was painful, but there was no increase in skin temperature and no sign of skin or joint infection. Other nails on the hands and feet were normal. Erythrocyanosis was present in other toes, notably the right 5th toe. Discoloration temporarily disappeared with friction of the skin. The remaining skin examination, including hands, was normal. There was no Raynaud’s phenomenon. Blood pressure after 15 min rest was 164/72 mmHg, heart rate 90 bpm, temperature 36.8°C, and body mass index 20 kg/m2. Results of routine blood tests, including C-reactive protein (CRP) and uric acid, were within the normal range, except for mild renal insufficiency (creatinine level 107 µmol/l, clearance 46 ml/min) and elevated thrombocyte count, 619 g/l (normal <400 g/l). Tests for antinuclear and antiphospholipid antibodies were negative.
What is your diagnosis? See next page for answer.
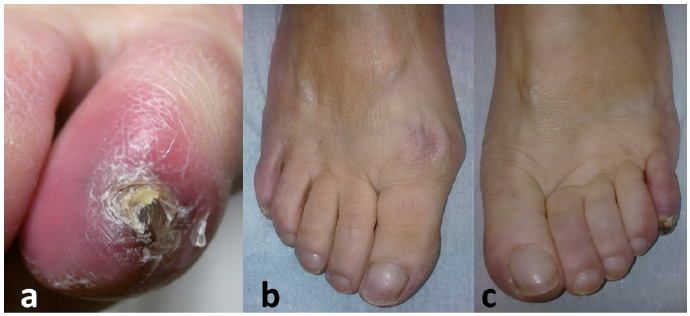
Fig. 1. (a) Close-up of erythematous-violaceous 5th left toe with nail dystrophy. (b and c) Mild erythrocyanosis affecting toes of both feet.
Acta Derm Venereol 2018; XX: XX–XX.
Diagnosis: Essential thrombocythaemia
A diagnosis of blue or purple toe was suspected on clinical examination of the affected toe and was verified by bilateral erythrocyanosis found on other toes, suggesting a more diffuse involvement of cutaneous small vessels of the feet.
The causes of blue or purple toe syndrome are numerous (1). The mechanisms leading to blue toes comprise all causes of interruption or slowing of blood flow in dermal small vessels. These include: (i) decreased arterial perfusion, caused by emboli (especially cholesterol crystals from atherosclerosis of the aorta and its branches), thrombosis, vasoconstriction, or vasculitis; (ii) impaired venous outflow from extensive venous thrombosis; or (iii) abnormalities in the circulating blood, including monoclonal gammopathy causing hyperviscosity, cryoglobulinaemia, cryofibrinogenaemia, cold agglutinins, and excessive number of red cells (polycythemia) or platelets (thrombocytosis).
In our patient, thrombocytosis was present in November 2017 and January 2018, with no skin findings and normal CRP levels. Aspirin, 100 mg/day, was started immediately. The pain improved within a few days, as reported in some previous cases (2). A blood sample was taken to search for Janus kinase 2 (JAK2) V617 mutation, which was present and allowed for the diagnosis of essential thrombocythaemia. The patient was referred to a haematologist for care and eventual specific treatment (3). The disease-specific life expectancy is normal, but thrombosis or, less frequently, bleeding, are common complications requiring a balanced decision before prescribing anti-platelet treatment (4).
Skin involvement may occur in essential thrombocythaemia, as in the case reported. Erythromelalgia is the most frequent manifestation, reported in 6% of cases in large studies (5), but mild forms are probably under-reported. Erythromelalgia was the main symptom leading to the diagnosis of essential thrombocytosis in 26 of 40 patients (6). Livedo reticularis, acrocyanosis and Raynaud’s phenomenon are other manifestations reported in essential thrombocythaemia, the frequency varying from 6% to 22% (5, 7). The diagnosis of erythromelalgia was excluded in our patient because pain was present only in the left 5th toe and was not exacerbated by warmth or alleviated by cold. A recent case-control study showed altered regulation of peripheral circulation in 45 patients with essential thrombocythaemia, including decreased flow and increased resistance, resulting in decreased temperature recorded at the skin surface of distal fingers (8), which is consistent with the case presented here.
Kidney involvement is not rare in essential thrombocythaemia: 29% of 45 patients had mild-to-moderate renal insufficiency and 38% had high blood pressure at the time of diagnosis (9). More than half of the patients showed improved renal function after lowering blood pressure and after treatment with aspirin and hydroxyurea (9).


 Click to show fullsize
Click to show fullsize