


Department of 1Dermatology and 3Pathology, Rabin Medical Center - Beilinson Hospital, Petach Tikva, and 2Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel
Data on the treatment of early folliculotropic mycosis fungoides, a recently defined clinicopathological subgroup of folliculotropic mycosis fungoides with an indolent course, is limited. Treatment outcomes were studied in a retrospective cohort of 47 adults with early folliculotropic mycosis fungoides, with a focus on psoralen plus ultraviolet A (PUVA) monotherapy, including dosimetric data, and the findings were compared with data for PUVA in 18 adults with early-classic mycosis fungoides. PUVA was given to 27 patients with early folliculotropic mycosis fungoides: 70% achieved complete response and 26% partial response. Significantly more treatments were needed to achieve complete response in stage IB compared with stage IA. There was no significant difference in the complete response rate from classic plaque-stage disease, although the early folliculotropic mycosis fungoides group required more treatments to achieve complete response, and a higher cumulative dose of UVA. Thus, PUVA is an effective treatment for early folliculotropic mycosis fungoides. Its complete response rate might be equal to early-classic mycosis fungoides; however, a longer induction phase is needed to achieve complete response.
Key words: folliculotropic; mycosis fungoides; psoralen and ultraviolet A; PUVA; phototherapy; cutaneous T-cell lymphoma.
Accepted Aug 7, 2018; Epub ahed of print Aug 7, 2018
Acta Derm Venereol 2018; XX: XX–XX.
Corr: Iris Amitay-Laish, Department of Dermatology, Rabin Medical Center – Beilinson Hospital, Petach Tikva 4941492, Israel. E–mail: amitaylaishiris@gmail.com
Since data on the treatment of early folliculotropic mycosis fungoides is limited, we studied the treatment outcomes in patients with this subset of mycosis fungoides. The majority of patients responded to nonaggressive treat-ments and had an indolent course. Systemic PUVA was the most common first line treatment, associated with a high response rate, whereas narrowband UVB was found to have low efficacy. Although PUVA, according to our study, might be an equally effective treatment as for early classic mycosis fungoides, significantly more exposures were needed to achieve complete response in early folliculotropic mycosis fungoides.
Folliculotropic mycosis fungoides (FMF) has long been considered an aggressive variant of mycosis fungoides (MF) (1, 2). However, our experience has shown that FMF presents with 2 distinct patterns of clinicopathological features representing an early variant and an advanced tumour variant. Their prognostic implications differ, with early FMF following a more indolent course (3). These findings were validated by the Dutch Cutaneous Lymphoma Group (4).
Traditionally, treatment recommendations for FMF have followed those for classic tumour-stage MF. Recently, the Dutch Cutaneous Lymphoma Group reported a response of patients with early FMF to skin-targeted therapy, and specifically psoralen plus ultraviolet A (PUVA) (5). In fact, in a few earlier publications (6–10) PUVA was found to be beneficial in a subset of cases of FMF, which, based on recent insights into the disease (3, 4), can be redefined as early FMF. In addition, in a small study of adults and children with clinicopathological features that were defined by us as those of early FMF, we observed a beneficial effect of skin-targeted therapy with PUVA bath and, in few cases, systemic PUVA (11, 12). Yet, data on the treatment outcome of PUVA in early FMF is still scarce, and there is no data on the specific protocol including the dosimetric parameters needed to achieve optimal response.
Early-classic MF is histologically characterized by the infiltration of lymphocytes into the epidermis, the dermo–epidermal junction, and the papillary dermis (13). By contrast, early FMF is characterized by epithelial infiltration to the follicle (3). The different and frequently deeper location of the dominant pathological focus in early FMF (3) may make it less accessible to skin-targeted therapy than early-classic MF. No comparisons of the efficacy of PUVA have been reported between early FMF and early-classic MF.
The aim of the present study was to assess the response of early FMF to initial treatments, especially systemic PUVA monotherapy, with an emphasis on dosimetric data, and to compare the findings with those for early-classic MF.
A retrospective cohort design was used. The study group consisted of consecutive patients treated for early FMF from January 1995 to June 2016 at the tertiary Cutaneous Lymphoma Clinic of Rabin Medical Center. FMF was defined according to the World Health Organization-European Organization for Research and Treatment of Cancer (WHO-EORTC) classification for cutaneous lymphomas (14).
Early FMF was defined according to the clinicopathological criteria, described in recent reports by our group and the Dutch group (3, 4). Clinically, we included patients who presented with follicle-based patch/flat plaques, keratosis pilaris-like lesions, and/or acneiform lesions. None of the patients had heavily infiltrated skin plaques, tumours, or nodules. The clinical findings were combined histologically with intrafollicular and sparse or lichenoid perifollicular infiltrates of atypical lymphocytes that were confined to the adventitial perifollicular dermis. No cases with diffuse perifollicular infiltrates extending to the reticular dermis, as reported in advanced FMF (3, 4), were included.
Of the 58 patients with early FMF who met the inclusion criteria, 11 were excluded from the final analysis because of inadequate follow-up. All presented with stage IA–IIA disease.
Data on background parameters, treatments administered, response to initial treatment, and disease status at the last follow-up were collected from the medical files. For systemic PUVA, we also recorded the number of treatments and the total treatment dose needed to achieve a complete response (CR). The response to treatment was assessed clinically from the time of treatment initiation to the best/maximal response and categorized as CR, partial response (PR), stable disease (SD), and progressive disease (PD), according to the criteria and clinical end-points recommended by the International Society for Cutaneous Lymphomas, the United States Cutaneous Lymphoma Consortium, and the Cutaneous Lymphoma Task Force of the EORTC (15). We also calculated the overall response rate (ORR) where appropriate.
For comparison, data were retrospectively collected from a control group of patients with well-defined, clinically and histologically proven early-classic plaque-type MF who were initially treated with systemic PUVA monotherapy at the same centre during the same period using the same protocol. Patients with early-classic MF found to have some follicular involvement on histological or clinical examination were excluded. Of the group of early-stage classic MF patients treated at our clinic from January 1995 to June 2016, 24 were initially treated with systemic PUVA monotherapy, 6 patients were excluded from the analysis because of inadequate follow-up.
PUVA treatment consisted of oral 8-methoxypsoralen, 0.5 mg/kg, with UVA exposure 2 h later. UVA radiation was delivered in a Waldmann UV 1000-k cabin (Herbert Waldmann GmbH & Co KG, Villingen-Schwenningen, Germany) with spectral distribution mainly in the 320- to 410-nm range and peak emission at 351 nm. The starting dose was 1 J/cm2 and was increased at fixed increments of 1 J/cm2 every second session. Sessions were conducted 3 times/week, up to a maximal median dose of 12 J/cm2 (range 5–15 J/cm2), according to the tolerability.
Maintenance treatment was given to patients who achieved CR. The protocol was as follows: continuous treatment at a constant dose (the dose needed to attain CR), twice weekly for 4 weeks, followed by once weekly for 4–6 weeks, followed by once every 2 weeks for 8 weeks and then once every 3–4 weeks.
The study was approved by the institutional ethical Helsinki Committee.
Rates of CR to PUVA were compared between patients with stage IA and stage IB early FMF and between patients with early FMF and early-classic MF using Fisher exact test. The number of treatments and the total treatment dose needed to achieve CR were compared between the same groups using the non-parametric Wilcoxon two-sample test. SAS version 9.4 was used for statistical analysis.
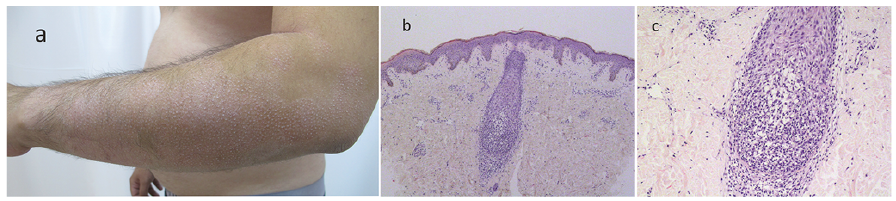
Initial treatment data were collected for 47 patients. There were 33 male and 14 female patients, all Caucasian, of median age 42 years (range 18–71 years); of note, 34 patients were reported in our previous study (3). Twenty-three patients had stage IA disease, 23 stage IB, and 1 stage IIA disease. The median time from symptom onset to diagnosis was 24 months (range 2–168 months). All patients were diagnosed clinicopathologically with early FMF (Fig. 1).
Fig. 1. Early folliculotropic mycosis fungoides: clinicopathological features. (a) Patches with spiky hyperkeratotic follicular papules and alopecia, located on the outer aspect of the arm. (b) Biopsy specimen from 1 of the lesions shows a hair follicle surrounded by a patchy lichenoid infiltrate and prominent folliculotropism. (Haematoxylin-eosin stain; original magnification ×40). (c) Magnification of (b) shows prominent folliculotropism. (Haematoxylin-eosin stain; original magnification ×100).
The treatment data are delineated in Table I. Photo-therapy was the most common first-line treatment, administered to 38 patients. The other 9 received different types of skin-directed therapy or systemic therapy or combination treatments.
Table I. Initial treatments administered to patients with early folliculotropic mycosis fungoides (n = 47), and responses
A total of 27 early FMF patients received systemic PUVA (Fig. 2). Response rates, the number of treatments, and UVA dose needed to achieve CR are delineated in Table II. Of note, there was no significant difference in the CR rate between stage IA and stage IB early FMF, although the IB group required more treatments to reach CR (p = 0.03).
Fig. 2. A patient with early folliculotropic mycosis fungoides presenting with patches with folli-cular accentuation on the abdomen. (a) Before treatment. (b) Complete response after 75 treatments with psoralen plus ultraviolet A (PUVA).
Table II. Response to psoralen plus ultraviolet A (PUVA) monotherapy in patients with early folliculotropic mycosis fungoides (FMF) and early classic plaque-stage mycosis fungoides (MF)
In all patients who underwent biopsy study (15/19), histopathological remission was confirmed.
Of the 10 patients treated initially with narrowband ultraviolet B (NB-UVB) (Table I), after a median of 30 treatments (range 24–60), only 3 responded.
Overall, clinical CR to initial treatment, (systemic PUVA or other skin-targeted/systemic modalities), was achieved in 26 of the total 47 patients (Table I).
The response to treatment in the 2 groups of patients is outlined in Table II.
The 27 PUVA-treated patients with early FMF included 21 men and 6 women of median age 41 years (range 21–70 years). Fourteen had stage IA disease and 13 had stage IB. The 18 PUVA-treated control patients with early-classic MF included 13 men and 5 women of median age 48 years (range 30–74 years). Five had stage IA disease and 13 had stage IB.
Although there was no significant difference in the overall CR rate between the 2 groups, compared with the early classic MF group, patients with early FMF required a significantly higher number of PUVA treatments and a higher cumulative dose of treatment to achieve CR. The difference between early FMF and early-classic MF in the number of treatments needed to achieve CR remained significant on further analyses by disease stage. The difference in the cumulative dose remained significant only for IB early FMF compared with IB early-classic MF.
Maintenance treatment was given to all 19 patients who were treated with systemic PUVA and achieved CR, for a median duration of 12 months (range 3–84 months). Relapse occurred in 7 of the 19 patients. The median time to relapse, from the first time of CR observed during the induction phase, was 18 months (range 6–60 months).
Of the 27 patients with FMF treated with PUVA, 3 subsequently acquired non-melanoma skin cancers (basal and/or squamous cell carcinoma) during a median follow-up period of 62 months (mean 84 months, range, 8–240 months). All these 3 patients received maintenance PUVA, for periods of 12, 24 and 36 months. None had other types of skin cancer.
At the last follow-up, median time of 61 months (mean 83 months, range 8–240 months), 46 patients were alive, of whom 22 (47%) had no evidence of disease, 17 (36%) had minimal disease, and 7 (15%) had significant disease. One patient died of disease. Stage progression from early to advanced FMF was noted in 3 patients (6.5%).
The present study evaluates the type and response to treatment of early FMF. It is the first study to provide more detailed outcomes including quantitative dosimetric data on PUVA treatment for early FMF. Furthermore, it is the first to provide a comparison of the efficacy of systemic PUVA between early FMF and early-classic MF (plaque-stage).
Systemic PUVA monotherapy was the most common first-line treatment used in our cohort of patients with early FMF. Overall, our results on the response to systemic PUVA are in agreement with the recent report from the Dutch Cutaneous Lymphoma Registry (5) summarizing their experience with the treatment of patients with different subtypes of FMF, including early FMF. However, the CR to PUVA was much higher in our series (70%) than in the Dutch series (30%) (5). This difference may be related to between-study differences in design and therapeutic protocol and to inter-observer variations. Our study group was much smaller than the Dutch study, but all our patients were diagnosed and followed by only 2 physicians, (EH and IAL), using similar protocol treatment and end points.
We found that a significantly higher number of exposures to PUVA was needed to achieve CR in the patients with stage IB FMF than in the patients with stage IA FMF. Likewise, Roenigk et al. (16) reported that the time to CR was much longer for extensive plaque MF than for limited plaque MF. Thus, it is not unlikely that in the Dutch series (5) the induction period was short relative to our series, resulting in a PR in patients who might otherwise have achieved CR had the induction phase been prolonged.
Recently, a retrospective study on 32 FMF cases was reported in which a response defined as “adequate PUVA response” was recorded in 34% of the patients. However, data regarding the subtypes of FMF included in that study, and detailed data regarding PUVA treatment were not provided (17).
According to the literature (18), CR rates under PUVA for stage IA MF are 70–100%, and for stage IB MF, 43–100%. Our CR rates of 80% for stage IA classic MF and 77% for stage IB classic MF fall within these ranges. Data are particularly sparse on the number of exposures to PUVA that are necessary to achieve CR specifically in patients with stage IA or IB MF (18). Studies of early stage MF in general reported a range of 17–42 PUVA treatments to CR (18). However, it should be emphasized that some of these cohorts of PUVA treatment in MF may have included patients with early FMF, as there was usually no attempt to separate this subgroup. In addition, summarizing the results of these reports is problematic given the differences in treatment protocols, study quality, patient selection, sample size, and outcome measures. It should also be noted that the literature regarding the effect of the type of lesion on the response to PUVA is strikingly scarce (18). Therefore, the reported data might not be accurate specifically for early-classic plaque-stage MF. By contrast, we limited our control group to a very select group of patients with early-classic plaque-stage MF only, all of whom were evaluated for response to PUVA at our clinic. Patients with some follicular involvement on histologic or clinical examination were excluded. Thus, the control group in the present study, albeit relatively small, was solid and informative. Our results showed that CR rates to systemic PUVA for early FMF, both overall and stage-based, were not significantly different from the rates for early-classic MF. Yet, regardless of disease stage, a significantly higher number of PUVA sessions were needed to achieve CR in the patients with early FMF than for patients with early-classic MF, and a significant higher cumulative dose of UVA was needed for early FMF. Accordingly, expert experience has shown that patches and thin plaques respond better to PUVA than thick plaques (19).
Retinoids decrease the thickness of the epidermis, (20) enhancing UV penetration and causing a more brisk response to UV exposure. A few studies have suggested that the combination of retinoids and PUVA could reduce the total number of PUVA sessions needed to achieve CR in early MF (21–25). Whether the addition of a systemic retinoid to PUVA could shorten the time to achieve CR also in early FMF is still unclear and warrants evaluation in a clinical trial.
NB-UVB treatment of stage IA–IIA MF has been associated with CR rates of 54% to 90% (19). Not unexpectedly, CR rates were higher for general patch (> 80%) than for plaque disease (> 50%) (26–29). In the present study of adults with early FMF, the CR rate for NB-UVB was only 30% (3 of 10 patients). This is close to the 25% (1 of 4 patients) found in our previous, albeit limited, experience with youth with early FMF (12). In contrast, no cases of CR were noted under NB-UVB in the Dutch cohort of 6 patients with early-stage FMF (5). Thus, treatment with NB-UVB appears to have relatively low efficacy in early FMF, similar to findings for plaque-stage classic MF.
Finally, the present findings strengthen the growing impression that most patients with early FMF have an indolent disease course (3, 4). In this study, which constitutes an extended follow-up of our previous study (3) with the addition of new patients, stage progression from early to advanced FMF was observed in only 6.5% of cases during a median follow-up time of 5 years (mean 7 years).
The main limitations of this study are the relatively small control group (although the results for the control group were similar to reports in the literature), and the retrospective data collection.
The majority of cases of early FMF responds to non-aggressive treatment and has an indolent course. In our series, systemic PUVA monotherapy was the most common first-line treatment and was associated with a high CR rate. Initial therapy with NB-UVB was associated with low response rates. Our findings strengthen and extend the results of the very few previous reports on the beneficial effect of PUVA in a subset of FMF cases. Furthermore, our data suggest that systemic PUVA monotherapy might be equally effective for the treatment of early FMF as for early-classic MF, although a longer induction phase is needed to achieve CR in early FMF. A larger prospective study is needed to validate these findings.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize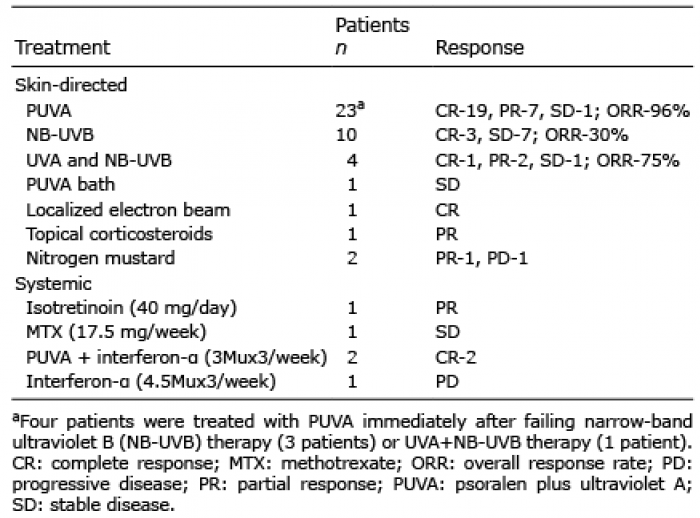 Click to show fullsize
Click to show fullsize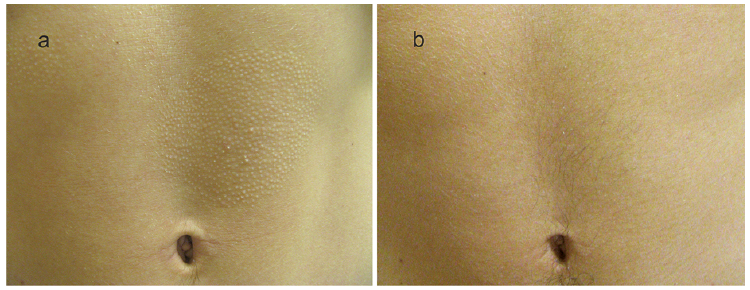 Click to show fullsize
Click to show fullsize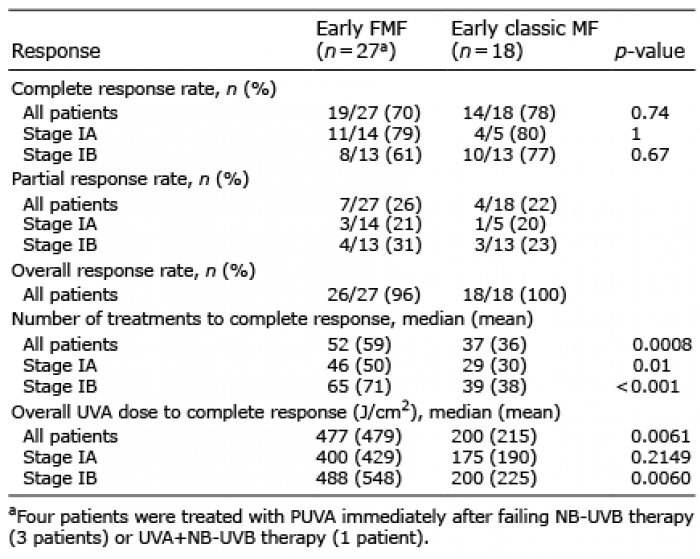 Click to show fullsize
Click to show fullsize