


1Department of Dermatology, University Hospital, 2Laboratory on Interactions Neurons-Keratinocytes (LINK), University of Western Brittany, Brest, 3Rennes University, UPRES EA 7449 REPERES Pharmacoepidemiology and Health Services Research, 4Department of Dermatology, University Hospital, Rennes, and 5French Association of Eczema, Redon, France
#These authors contributed equally to this work.
The objective of this study was to explore characteristics of pruritus in atopic dermatitis (AD) in relation to the severity of AD. A web-questionnaire was used, which included the Patient-Oriented SCORing Atopic Dermatitis index, the 5-D itch scale and the Brest questionnaire. A total of 170 participants were included (86.5% women, mean age 30.9 years). Severity of AD was mild for 8.2% of patients, moderate for 38.2% and severe for 53.5%. Mean 5-D itch scale was 13.2. The mean intensity of pruritus was 5.8, and mean sleep loss was 4.7 (from 0 to 10). The participants frequently described burning (61.8%) and stinging (58.8%); these symptoms suggest a neuropathic component. Pruritus was worse in severe AD compared with moderate AD, exhibiting a higher impact on sleep and more associated symptoms. The majority of participants reported sleep disturbance as a result of pruritus. The characteristics of pruritus varied depending on the severity of AD.
Key words: atopic dermatitis; pruritus; questionnaire; itch; web questionnaire; PO-SCORAD; 5-D itch scale.
Accepted Sep 27, 2018; E-published Sep 28, 2018
Acta Derm Venereol 2019; 99: XX–XX.
Corr: Emilie Brenaut, Department of Dermatology, University Hospital, FR-29609 Brest, France. E-mail: emilie.brenaut@chu-brest.fr
Pruritus is a frequent symptom in atopic dermatitis and it has a major impact on quality of life. Only a small number of studies have explored the characteristics of pruritus in atopic dermatitis. The aim of our study was to characterize pruritus while considering the severity of atopic dermatitis, thanks to a web-questionnaire. One hundred and seventy participants were included. The mean intensity of pruritus was 5.8, and the mean sleep loss was 4.7 (from 0 to 10). The participants frequently described burning (61.8%) and stinging (58.8%). In severe atopic dermatitis compared to moderate atopic dermatitis, pruritus was more severe, exhibiting a higher impact on sleep and more associated symptoms.
Pruritus is defined as an unpleasant sensation that provokes the desire to scratch (1, 2). It is a frequent symptom in many skin diseases, as well in systemic diseases (3, 4). Pruritus is a primary symptom of atopic dermatitis (AD) and constitutes one of the major diagnostic criteria, according to Hanifin & Rajka’s (5) and the UK Working Party’s diagnostic criteria for AD (6). AD is a common, chronic, pruritic, relapsing inflammatory skin condition, which is an increasingly important public health problem worldwide, with a prevalence of 10–30% in children and 2–10% in adults (7). In France, the prevalence of AD is estimated at 3.6–4.7% in adults (8, 9). The condition has a high burden, with serious psycho-social impact and impaired quality of life (10–12). However, only a few studies have explored the characteristics of pruritus in AD (4, 11, 13–15), and none have analysed the correlation of pruritus with severity of AD. The aim of the current study was to characterize pruritus in relation to the severity of AD, using Patient-Oriented SCORing Atopic Dermatitis (PO-SCORAD).
A web questionnaire on pruritus in AD was available on the website of the French Association of Eczema (Association Française de l’Eczéma) between January 2015 and March 2016. This association was established in 2011 for patients with AD or contact eczema and provides information and advice regarding these diseases via its website and social networks.
The initial questions were related to age, sex and eczema type (atopic dermatitis, contact eczema or other). The severity of AD was evaluated using the validated self-assessed AD severity score: the PO-SCORAD index. The PO-SCORAD, established in 2011 by Stalder et al. (16), measures the severity of AD during the previous 3 days and integrates objective and subjective symptoms with the help of an illustrated tutorial (16). The score ranges from 0 to 103, with a higher score indicating a more severe disease. The evaluation of severity of AD by PO-SCORAD is divided into several parts: surface area of skin affected by eczema, objective symptoms from 0 (non-existent) to 3 (severe): dryness of the skin without eczema and redness, swelling, oozing/crust, scratching, and thickening of the skin affected by eczema, and a visual analogue scale from 0 (absence) to 10 (very important) to evaluate pruritus and sleep loss. In the next section, participants responded to the Brest questionnaire, which has been used in previous studies of different diseases, such as small-fibre neuropathies, neurofibromatosis 1 or systemic sclerosis (13, 17–19). Participants were asked about the duration, chronology, and intensity of pruritus in AD. The intensity of pruritus was assessed with a visual analogue scale from 0 to 10 (i.e. at its worst, best, average, and at the time of the study). Participants were asked about symptoms associated with pruritus: sweating, headaches, pain, heat and cold in the region of the pruritus. The following symptoms were evaluated from 0 (non-existent) to 3 (severe): stinging, tickling, crawling, stabbing, pinching, heat sensation, biting and stroking. Participants were asked whether they scratched, how pleasurable it was, and whether pain alleviated the pruritus. Finally, participants completed the validated 5-D itch scale. This multidimensional score, from 5 (no pruritus) to 25 (most severe pruritus), was developed by Elman et al. in 2009 (20) and contained 5 domains (duration, degree, direction, disability, and distribution).
Statistical analysis was performed using RStudio Version 1.0.136 (RStudio, Inc., Boston, MA, USA). Descriptive statistics for quantitative variables were presented as the means and standard deviation (SD) and as percentages for qualitative variables. To compare the 3 groups (mild, moderate and severe AD), Kruskal–Wallis test was used to compare means, and a Fisher’s exact test was used to compare frequencies. Statistical significance was set at p < 0.05.
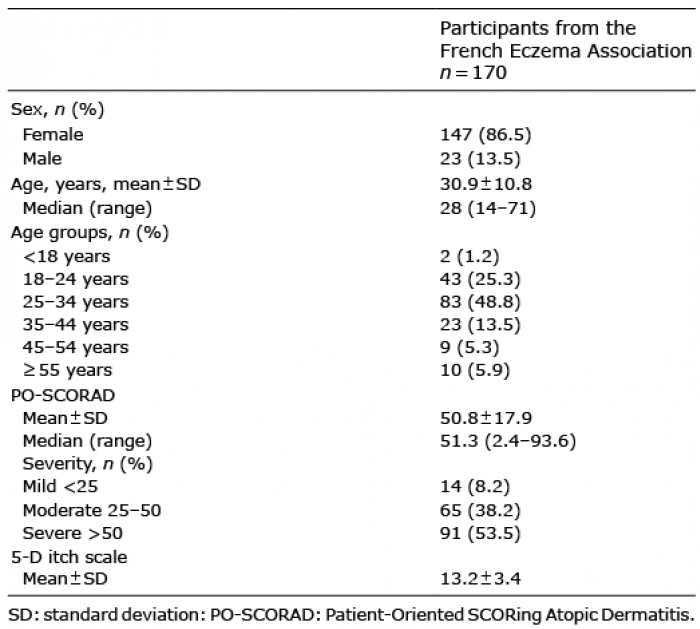
Among the members of the French Eczema Association, 202 completed the questionnaire. Finally, 32 participants were excluded: 13 subjects were too young (< 14 years) to understand the questionnaire because it was not adapted for children, and 19 subjects reported another diagnosis (psoriasis, contact eczema, dyshidrosis). A total of 170 participants were included. Demographic data are presented in Table I.
Table I. Demographic data
Characteristics of PO-SCORAD are presented in Table I. The following objective symptoms affected the participants from an extreme to a moderate intensity: scratching for 68.8%, redness for 65.9%, skin dryness for 63.5%, thickening for 61.8%, oozing/crust for 24.7% and swelling for 20.0%. Over the most recent 3 days, the mean intensity of pruritus was 5.8, and the mean sleep loss was 4.7 on a visual analogue scale ranging from 0 to 10.
Most participants (81.8%) had had pruritus for years, 9.4% for months, 3.5% for weeks and 5.3% for days. For 62.3% of participants, pruritus was intermittent; in the remaining participants, pruritus was continuous.
The presence of pruritus at different times of day is shown in Fig. 1. Pruritus was reported to occur “always or often” in the morning by 51.8% of subjects, in the afternoon by 52.9% of participants, in the evening by 78.8% of participants and at night by 69.4% of participants.
During the 2 weeks before completing the questionnaire, 73 participants (42.9%) had had pruritus for less than 6 h a day, 18.2% between 6 and 12 h a day, 18.2% between 12 and 18 h a day, 11.9% between 18 and 23 h a day, and 8.8% all day.
Fig. 1. Presence of pruritus at different times of day reported by the participants (n = 170).
The intensity of pruritus was assessed with a visual analogue scale ranging from 0 to 10. At the time of the study, the mean intensity was 3.9; at its worst, the intensity was 8.8; at its best, the intensity was 1.7; and mean intensity was 4.9. During the 2 weeks preceding the study, participants were asked to evaluate the intensity of the pruritus from none to unbearable. It was unbearable for 12.9% of participants, severe for 30.6%, moderate for 45.3%, mild for 10.0% and not present for 1.2%.
In the PO-SCORAD, the most frequently involved areas were head (64.1%), neck (54.1%), inside the elbow (58.2%), forearms (53.8%), and popliteal fossa (49.1%). The pruritus was described as symmetrical for 64.1% of participants.
On the 5-D itch scale, pruritus was present in 0–2 zones of the body in 7.1% of subjects, 3–5 zones in 9.4%, 6–10 zones in 28.8%, 11–13 zones in 12.9% and 14–16 zones in 41.8%.
Heat sensation (83.5% of subjects) and pain (54.1%) were the most frequently reported associated symptoms. Sweating was reported by 34.1% of the participants, whereas headaches and cold sensation were rarely described (< 5%). Associated symptoms are reported in Fig. 2. Each sensory symptom was assessed by the subject from 0 (absence) to 3 (intense). Symptoms that were reported more frequently (evaluated as moderate or intense) were burning (61.8%) and stinging (58.8%).
Fig. 2. Associated symptoms in patients with atopic dermatitis.
Exacerbating/alleviating factors of pruritus are shown in Fig. 3. A total of 86 participants (50.6%) responded that pain relieved pruritus. Pruritus impaired sleep, as shown in Fig. 4.
Fig. 3. Exacerbating and alleviating factors of pruritus in patients with atopic dermatitis.
Fig. 4. Effect of pruritus on sleep in patients with atopic dermatitis.
For the question: “Do you scratch?”, 54.1% of participants answered “very often”, 39.4% “often”, 5.9% “rarely”, and 0.6% “never”. Scratching was described as very pleasurable by 34.1% of participants, moderately pleasurable by 36.5%, neutral by 7.6%, moderately unpleasant by 7.1% and very unpleasant by 14.7%.
Patients were classified into 3 groups according to their PO-SCORAD score: slight AD (< 25), moderate AD (25–50) and severe AD (> 50). The characteristics of the 3 groups are shown in Table II; only moderate and severe AD were compared.
Table II. Comparison according to the severity of atopic dermatitis
Pruritus is a major symptom of AD, but no qualitative assessment of its characteristics according to severity has been published to date. In the current study, pruritus of AD was severe, with frequently associated sensations and frequent scratching. Yosipovitch et al. was the first to describe pruritus in AD using a qualitative approach (11); several other studies have thereafter also been published (4, 13–15). A previous study used a web-questionnaire to analyse itch characteristics in AD (21). Some characteristics were similar to those previously described in studies about pruritus in AD: aggravation in the evening, factors exacerbating pruritus as dryness, sweating, and physical effort (14).
In the current study, pruritus tended to appear more frequently in the evening and at night. These tendencies have been well described in AD (11, 14, 15) and in other dermatoses (17, 22). To date, the underlying mechanisms responsible for nocturnal pruritus are not well-understood, but could be related to the circadian rhythm of various mediators as well as skin temperature and barrier function (15, 23) or to the absence of distracting tasks for patients. Exacerbation of pruritus in the evening and at night might cause under-evaluation of the pruritus intensity by physicians. By interfering with sleep, pruritus greatly impaired quality of life (24, 25). This study supports previous reports concerning the major exacerbating factors of pruritus in AD: skin dryness, stress, sweating, specific fabrics, fatigue, hot ambient temperature, hot water, and physical effort (11, 13). These characteristics are also described in other diseases (17, 22). The simplest intervention that should be recommended first to treat the itch associated with AD is avoidance of these exacerbating factors (26). Alleviating factors are cold water and rest, as highlighted in previous studies (11, 13, 14).
Although scratching may ultimately aggravate itching in AD, 93% of participants admitted to scratching often or very often; the majority of participants perceived scratching as pleasurable. The majority of participants answered that pain relieved pruritus (4, 13). Itch and pain have many similarities; specifically, scratching relieves itching by activating nociceptors and pain inhibits itching (15). In AD, these similarities could lead to a vicious itch-scratch cycle, in which scratch damage enhances itching (15).
We used the validated 5-D itch scale to explore pruritus in AD. This scale is a multidimensional, reliable and replicable measure of itching that may allow further comparisons. Elman et al. (20) first established the 5-D itch scale in 2009 and evaluated itching in different pruritic diseases. In AD, the 5-D itch scale score was higher than in other diseases, such as skin carcinoma (27), neurofibromatosis 1 (18), and systemic sclerosis (19).
To our knowledge, this study is the first to perform a qualitative analysis of pruritus according to the severity of AD using PO-SCORAD. A majority of participants had a severe form of AD with a PO-SCORAD >50. We chose to compare only moderate and severe AD because the group of mild AD included only 14 patients. The mean PO-SCORAD was 50.8, which was higher compared with other studies: 39.32 in Stalder’s study (16), 46.0 in Chrostowska’s study (28) and 41 in Darsow’s study (29). Moreover, those who have severe AD may be more inclined to help research by completing a questionnaire. In severe compared with moderate AD, pruritus was significantly more intense, with a higher negative impact on sleep and more frequently associated symptoms, including stinging, tickling, stabbing, burning, stroking, and increased scratching. Interestingly, the correlation between the severity of the disease and the intensity of pruritus is less obvious in some diseases, such as psoriasis (30).
The results of the current study showed that stinging, burning and pain sensations were very frequent, suggesting a nociceptive component to the pruritus (31). A recent study highlighted in 305 patients with AD that skin pain is a common and burdensome symptom in AD (32–34). The underlying cause of this phenomenon could be because of direct skin nerve damage secondary to scratching. Stumpf & Ständer (35) reported similar phenomena in post-burn and post-surgery scars. In severe forms, some medications, such as gabapentin or pregabalin, could be used to alleviate the pruritus. These medications are structural analogues to gamma-aminobutyric acid and are used in severe pruritus in several diseases (36).
Among factors influencing AD pruritus, it is important to note that it is relieved by cold ambient temperature and cold water. This observation is supported by another study in which a cold water bath was the method that was most used to relieve pruritus in patients with AD (11). One of the hypotheses to explain the effect of cold in AD pruritus is the role of TRP member-8 (TRPM-8) or Cold and Menthol receptors (CMR) (37).
The main limitation of this study was that patients could not be examined by a physician to confirm the diagnosis and severity. Moreover, patients with no access to the internet and who are unfamiliar with the French Association of Eczema could not participate, thus creating a selection bias. Patients who are members of the French Association of Eczema are not representative of the patients with AD because they most likely have moderate or severe AD compared with mild AD. Moreover, our population was not representative because the majority of the study population was women (86.4%). In a recent study, Barbarot et al. (8) described a feminine predominance (54.5%) of AD and a prevalence of AD in France estimated at 3.6%. Possible explanations are that women have more involvement in health associations than men and that women completed web surveys more often than men.
This study confirms that pruritus is severe in AD. Sensory symptoms (burning, stinging, tickling, crawling) are frequent, suggesting a neuropathic component to pruritus in AD. In patients with severe AD, pruritus is more severe, with a higher impact on sleep and more associated symptoms compared with moderate AD.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize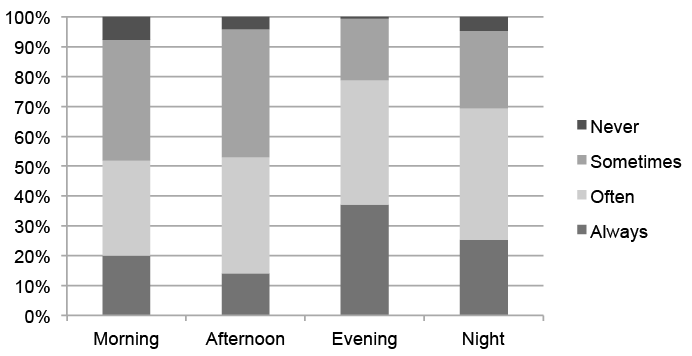 Click to show fullsize
Click to show fullsize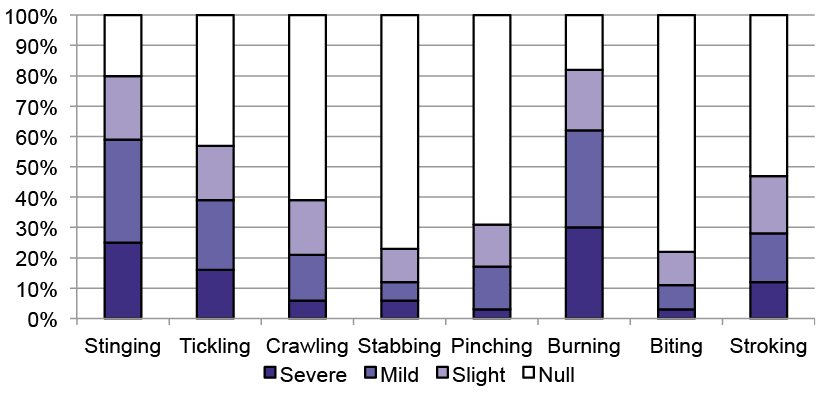 Click to show fullsize
Click to show fullsize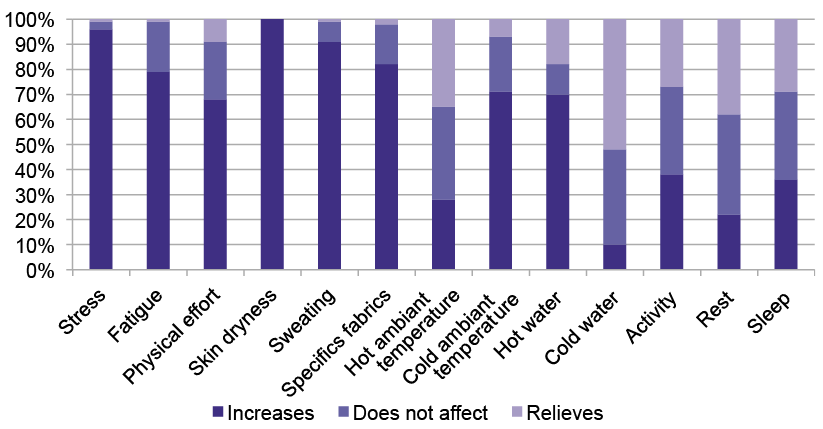 Click to show fullsize
Click to show fullsize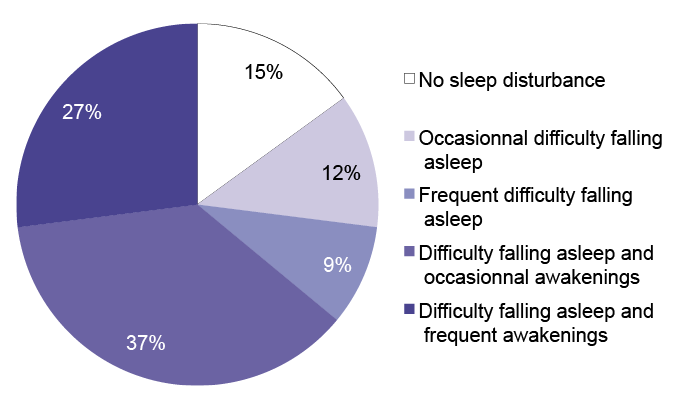 Click to show fullsize
Click to show fullsize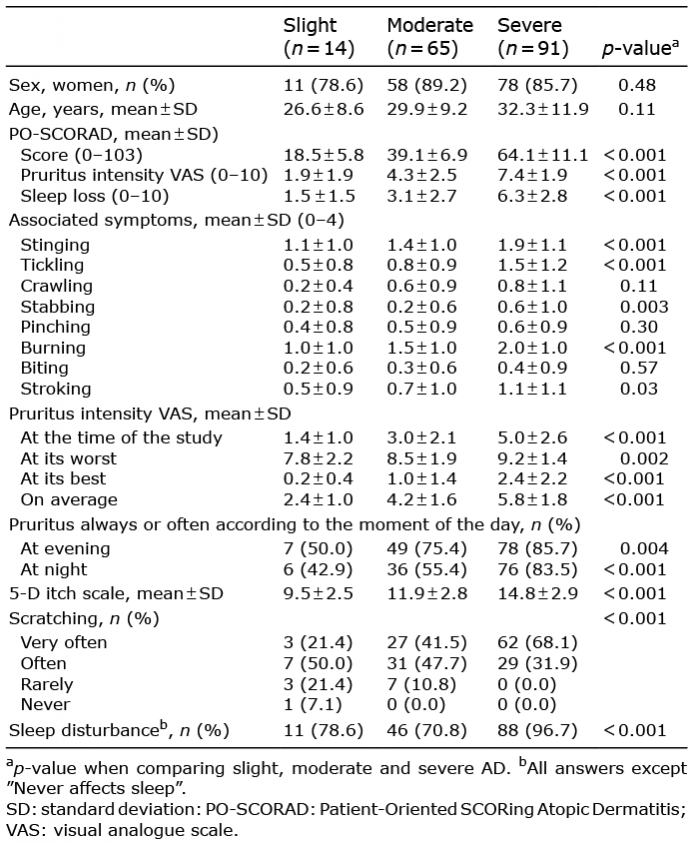 Click to show fullsize
Click to show fullsize