


Department of Dermatology, Radboud University Medical Center, Nijmegen, The Netherlands
Treatment of chronic pruritus can be a challenge for clinicians. Several systemic treatments have been suggested to reduce itch, such as gabapentinoids and antidepressants. The aim of this study was to assess the current practice of dermatologists regarding systemic treatment in patients with chronic pruritus, and to identify possible barriers in the prescription of these treatments. An online survey was sent to all dermatologists and dermatology residents in the Netherlands between July 2017 and April 2018. A total of 193 physi-cians completed the questionnaire (response rate 27.0%). Overall, 61.7% prescribed gabapentinoids or antidepressants in patients with chronic pruritus. Amitriptyline was prescribed most frequently, followed by gabapentin, doxepin and mirtazapine. Reasons not to prescribe systemic treatment included lack of knowledge or experience, risk of side-effects, and lack of available evidence. As only a minority of respondents felt comfortable prescribing these drugs, more education on effective and safe dosing is needed.
Key words: pruritus; therapeutics; gabapentin; antidepressive agents; survey.
Accepted Dec 6, 2018; E-published Dec 6, 2018
Acta Derm Venereol 2019; 99: XX–XX.
Corr: Tessa Kouwenhoven, Radboud University Medical Center, Department of Dermatology, PO Box 9101, NL-6500 HB Nijmegen, The Netherlands. E-mail: Tessa.Kouwenhoven@radboudumc.nl
This study analysed the prescription of systemic treatment by dermatologists in patients with chronic itch. Overall, 6 out of 10 dermatologists prescribed antidepressants or gaba-pentinoids, of which, antidepressants were prescribed most frequently. Reasons not to prescribe systemic treat-ment included lack of knowledge or experience, risk of side-effects, and lack of available evidence. Only a minority of the clinicians surveyed felt comfortable prescribing these drugs; therefore, we recommend more education on effective and safe dosing.
Itch is one of the most common symptoms presented in daily dermatological practice, with an estimated point prevalence of 36.2% (1–3). Chronic pruritus (CP) (itch present for a minimum of 6 weeks) can be caused by several dermatological, systemic, neurological and psychiatric disorders (2, 4). CP is associated with a reduced quality of life, including impact on mood, concentration and sleep, and a higher risk of anxiety and depression (5–8).
Several systemic treatment options have been suggested for patients with CP (2, 9–11). For example gabapentinoids, such as gabapentin and pregabalin, were used in patients with uremic pruritus and neurogenic itch (12–20). In addition, treatment with oral antidepressants, such as mirtazapine, paroxetine and sertraline, have been recommended in patients with pruritus unresponsive to conventional treatment options, and particularly in patients with uraemic pruritus, cholestatic pruritus or paraneoplastic pruritus (21–28). Other systemic treatment options include opioid receptor agonists and antagonists, thalidomide and neurokinin 1 receptor (NKR1) antagonists (29–36).
Due to its heterogeneity and difficult to establish underlying origin, treatment of CP remains a challenge for clinicians (37, 38). If systemic treatment is initiated, side-effects can complicate therapeutic attempts, especially in elderly patients. In addition, dermatologists might not feel comfortable prescribing psychotropic medication (39). Data on the use of systemic treatments for CP by clinicians in daily practice is currently scarce.
The aim of this study was to provide more insight into the current practice of dermatologists regarding systemic treatment in patients with CP, including identification of the treatments used, clinicians’ experiences on reducing itch after initiation of systemic treatment, and possible barriers to prescription of systemic treatment.
An anonymous web-based questionnaire was sent by e-mail to all members of the Dutch Society of Dermatology and Venereology (NVDV) between July 2017 and April 2018. It was first piloted to dermatologists (n = 3) and dermatology residents (n = 6) in June 2017 at the Radboud University Medical Center, Nijmegen, the Netherlands, resulting in the adaptation of a few questions and instructions to avoid ambiguity. The final questionnaire consisted of 19 questions, including multiple-choice questions, 5-point Likert scale questions and open-ended questions. Participants were asked about demographic and professional data, prevalence of CP in their clinical practice, use of antiepileptics and antidepressants in treatment of CP, their level of comfort in prescribing these pharmaceuticals and other systemic treatment options used in treatment of CP. In this survey, CP was defined as itch present for a minimum of 6 weeks due to both dermatological and non-dermatological conditions. Study data were collected and managed by Qualtrics web-based survey software (Provo, UT, USA). The entire survey is available in Table SI.
Data of respondents were displayed as means and standard deviations (SD) for continuous variables, and numbers and percentages for categorical variables (n (%)). Age, sex, profession and practice setting of the respondent population were compared with the target population to test for selection bias. Subgroup analyses were conducted to compare the influence of physician subgroup, years of clinical experience and practice setting on the prescription of systemic treatments using independent χ2 tests. p < 0.05 was considered statistically significant. All statistical analyses were performed with SPSS, version 22.0 (IBM SPSS Inc, Chicago, USA).
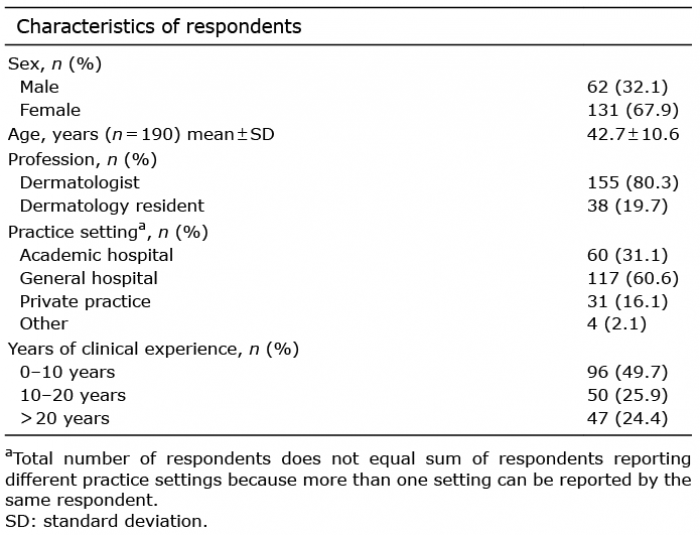
A total of 193 members responded (response rate 27.0%), including 155 (80.3%) dermatologists and 38 (19.7%) dermatology residents (Table I). The mean ± SD age of all respondents (67.9% women) was 42.7 ± 0.6 years. Most respondents practiced in a general hospital (60.6%) or academic hospital (31.1%). A comparison of sex, age, profession and practice setting between the respondent population and target population showed no significant differences (data available on request).
Table I. Demographics of survey respondents (n = 193)
Respondents were asked to estimate the number of patients seen with CP that could not be resolved by treatment of an underlying cause or by conventional treatment options (e.g. topical treatments or oral antihistamines), and therefore had a possible indication for systemic treat-ment. Most respondents estimated that they saw at least one patient in the described population per week (33.2%) or per month (33.7%), followed by one patient per 3 months (13%) or even one patient per day (9.8%) (Table II).
Table II. Prevalence of chronic pruritus in daily clinical practice, prescription of antiepileptic treatment in patients with chronic pruritus (CP) and prescription of antidepressants in patients with CP
Overall, 74 (38.3%) respondents prescribed gabapentinoids for patients with CP (Table II), of whom 47 (64.4%) prescribed gabapentin, 10 (13.7%) prescribed pregabalin and 16 (21.9%) prescribed both. When these respondents were asked about the efficacy of these treatments on reducing itch using a 5-point Likert scale (ranging from very poor to very good), the majority reported a fair (gabapentin 61.9%; pregabalin 66.7%) or good (gabapentin 25.4%; pregabalin 22.2%) treatment effect (Table III). Significantly more respondents who are currently working in an academic hospital (66.0%; p = 0.000) prescribed gabapentin or pregabalin compared with respondents working in general hospitals (26.7%) or private practices (19.0%) (Table SII). In addition, significant differences were found according to profession (dermatologist 32.9%; dermatology resident 60.5%; p = 0.002) and clinical experience (0–10 years 51.0%; 10–20 years 24.0%; > 20 years 27.7%; p = 0.001). When respondents not prescribing gabapentin or pregabalin (n = 119; 61.7%) were asked to explain why they did not prescribe these pharmaceuticals, the majority stated they did not have enough knowledge or experience (86.5%), followed by risk of side-effects of gabapentinoids (13.4%) and lack of available evidence on efficacy of antiepileptic treatment (9.2%) (Table II). Two respondents stated that they had not heard of the option of gabapentin or pregabalin treatment for CP.
Table III. Respondent experiences on reducing itch after initiation of antiepileptic medication (n = 74) or antidepressants (n = 101) using a 5-point Likert scale
Over half of those surveyed (52.6%) prescribed oral antidepressants for treatment of CP (Table II). The majority of these respondents prescribed amitriptyline (81.2%), followed by doxepin (29.7%), mirtazapine (12.9%), paroxetine (11.9%) and nortriptyline (6.9%). Only 2 respondents prescribed fluoxetine (2.0%) or sertraline (2.0%). The treatment effect of these drugs was mostly rated as ‘fair’ or ‘good’ (Table III). One respondent even reported a ‘very good’ treatment effect after initiation of mirtazapine. No significant differences in prescription of antidepressants were found with respect to profession, years of clinical experience or practice setting (Table SII). Respondents not prescribing antidepressants (n = 91; 47.4%) stated they had not enough knowledge or experience (87.9%); or were worried about side-effects (16.5%) and lack of available evidence (12.1%) (Table II).
When participants were asked if they were comfortable about prescribing gabapentinoids, the majority disagreed (32.3%), or strongly disagreed (20.3%) (Table IV). When these outcomes were specified for respondents prescribing gabapentin or pregabalin, more respondents reported feeling comfortable (30.1% vs. 11.8%; p = 0.000). The same was true for prescription of antidepressants, as the majority of respondents also disagreed about feeling comfortable prescribing these drugs (34.2%), and more respondents felt comfortable if they were actually prescribing these treatments (27.7% vs. 11.0%; p = 0.000).
Table IV. Respondents feeling comfortable prescribing antiepileptic treatment and antidepressants for the treatment of itch
When asked about other treatment options used by respondents in daily clinical practice for the treatment of CP, the majority of respondents reported oral immuno-suppressants, such as methotrexate or cyclosporine A, and opioid antagonists, such as naltrexone. Other suggestions were haloperidol, ondansetron and thalidomide.
This survey was conducted to investigate the current practice of dermatologists and dermatology residents in the Netherlands regarding systemic treatment in patients with CP. More than 40% of respondents reported having seen patients with CP and a possible indication for systemic treatment at least once per day or once per week, and another 30% reported seeing such patients at least once every month. As this is even more than the estimated point prevalence of CP described earlier in a cross-sectional study in dermatological practice (1), a large group of patients demands an effective and safe treatment for their symptoms.
In our study, more than half of the physicians surveyed (52.6%) have prescribed antidepressants in patients with CP. The most commonly prescribed antidepressant was amitriptyline (81.2%). However, evidence for the use of amitriptyline in the treatment of CP is limited, as it was described in only one observational study, 2 case series and 3 case reports, mainly describing patients with pruritus of neuropathic origin (e.g. brachioradial pruritus or notalgia paraesthetica) (40–45). The other frequently prescribed antidepressants, doxepin (29.7%), mirtazapine (12.9%) and paroxetine (11.9%), have been described more frequently, mostly for paraneoplastic pruritus, uremic pruritus or pruritus of unknown origin (21, 23, 24, 28, 46–50), and were recommended in guidelines for various forms of CP not responsive to conventional treatment options (2, 9, 51). This discrepancy could be explained as amitriptyline is an established pharmacological intervention for neuropathic pain (52), and is therefore well known by most dermatologists.
According to the respondents in our survey, gabapentinoids are prescribed less frequently in daily practice compared with antidepressants (38.3% vs. 52.6%). Of these 2 treatments, gabapentin is prescribed more often compared with pregabalin (65.0% vs. 35.0%), probably as pregabalin is a relatively new drug with fewer studies examining its use in patients with CP (10). In addition, evidence comparing the efficacy of gabapentin and pregabalin is limited, with only one open-label trial in haemodialysis patients with neuropathic pruritus (n=40), showing no significant difference between the 2 pharmaceuticals (53).
Almost all respondents not prescribing antiepileptics or antidepressants (86.5% and 87.9%, respectively), stated they had limited knowledge or experience to initiate these treatments. In addition, 2 respondents stated that they never heard of the option of gabapentin or pregabalin treatment in patients with CP. Lack of experience and knowledge was also shown by the low rates of respondents feeling comfortable prescribing these drugs. For example, more than half of respondents prescribed antidepressants, with only 23.8% feeling comfortable or very comfortable prescribing them. These results are similar to a previous survey evaluating the use of psychotropic treatment among dermatologists (n = 59), showing that only a few dermatologists felt comfortable (11%) or very comfortable (3%) prescribing antidepressants for psychocutaneous disorders (39). Interestingly, in the same population far more dermatologists felt comfortable (66%) or very comfortable (18%) starting treatment for neuropathic pain, including gabapentin and pregabalin. It is important to acknowledge dermatologists’ lack of knowledge and experience on prescription of these drugs, especially as not all patients can be seen in specialized centres due to the high prevalence of this symptom. Use of guidelines, education on effective and safe dosing, and close cooperation with specialized centres can be helpful to improve care of CP.
In a recent survey conducted in Germany, patients with CP reported finding a clear diagnosis and therapy, being free of itch and having confidence in the therapy as their most important treatment goals (54). However, effective treatment of CP remains a challenge for clinicians, often using gabapentinoids and antidepressants as a last resort (37, 38). As these pharmaceuticals might have substantial side-effects, especially in geriatric patients or patients with multiple comorbidities or concomitant medications, and are not registered for treatment of CP, there is still an unmet need for an effective and safe treatment (10, 11).
A limitation of our survey is the response rate of approximately 30%, and therefore a risk of selection bias. However, no significant differences in age, sex, profession and practice setting were found between our response population and the target population.
In conclusion, over half of respondents of our survey prescribed antidepressants for treatment of pruritus. Even though evidence is scarce, amitriptyline was prescribed most often, followed by mirtazapine, doxepin and paroxetine. Compared with antidepressants, gabapentin and pregabalin were prescribed less frequently. A minority of respondents felt comfortable prescribing these treatments, and a lack of knowledge and experience was considered the main reason not to prescribe antiepileptic of antidepressant treatment. Therefore, we recommend more education on effective and safe dosing.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize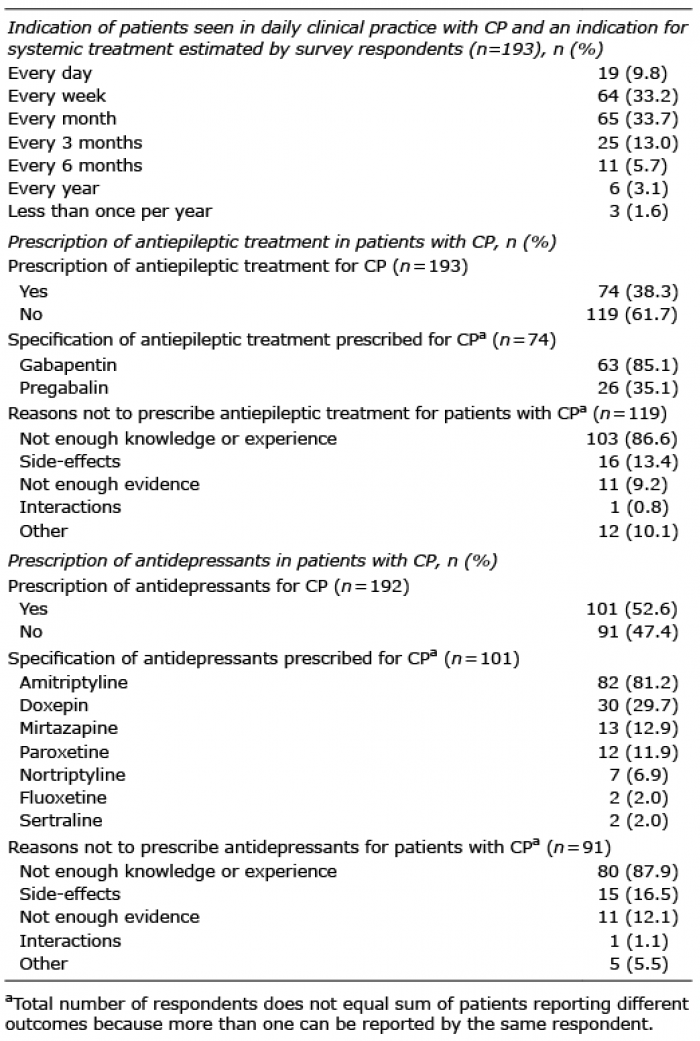 Click to show fullsize
Click to show fullsize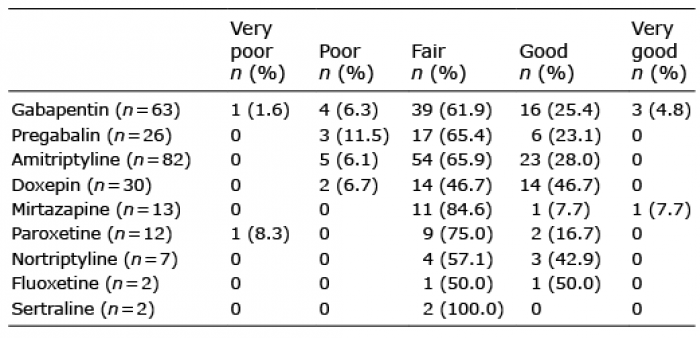 Click to show fullsize
Click to show fullsize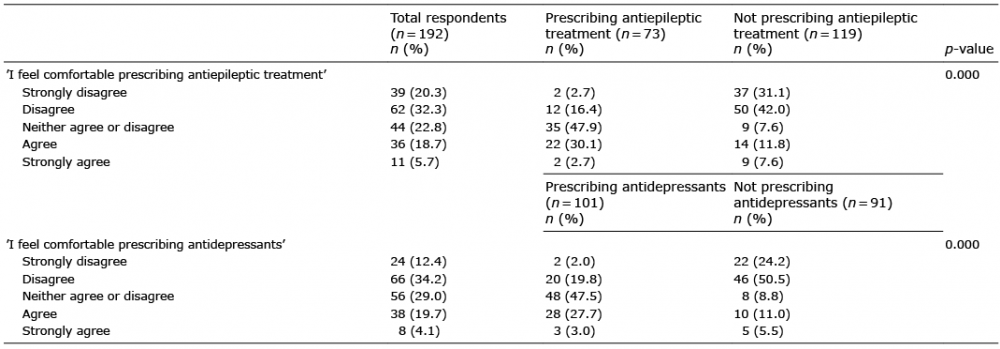 Click to show fullsize
Click to show fullsize