


1Central Laboratory of Pathology, Nice University Hospital, 30, Avenue Voie Romaine- CS 51069, FR-06001 Nice, Cedex 1, France, 2Department of Dermatology, Imperia Hospital, Imperia, Italy, and 3Laboratory of Solid Tumors Genetics, Institute for Research on Cancer and Aging of Nice (IRCAN) CNRS UMR 7284/INSERM U1081, Université Côte d’Azur, Nice University Hospital, Nice, France. E-mail: xst.perrin@bbox.fr
#These authors contributed equally to this work.
Accepted Feb 26, 2019; E-published Feb 27, 2019
Cellular angiofibroma (CAF) is an uncommon benign mesenchymal tumour that occurs in both sexes, mainly in the genital region. Extragenital CAF is rare, with fewer than 10 cases reported to date (1–3) and, to the best of our knowledge, there has been no report of CAF occurring in the subungual or periungual region. We describe here the first case of CAF of the subungual region of the toe. Immunohistochemical features and fluorescence in situ hybridization (FISH) ruled out more aggressive neoplasms, such as low-grade fibromyxoid sarcoma (LGFMS) and myxoid dermatofibrosarcoma protuberans (DFSP).
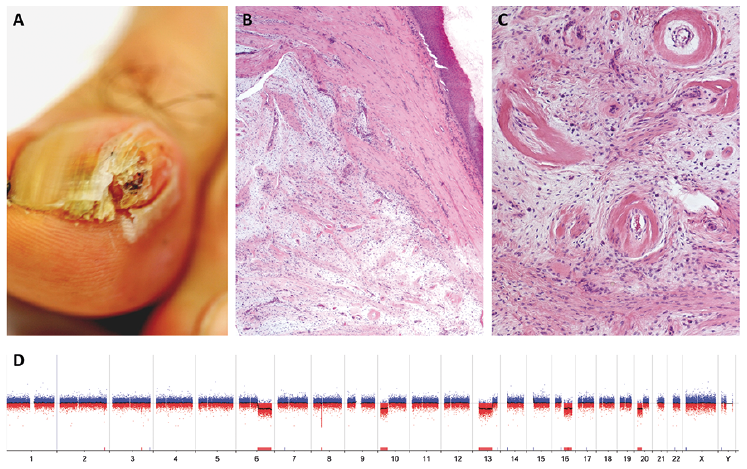
A 46-year-old man presented with a 2-year history of onychodystrophy of the radial aspect of his right big toe. Physical examination revealed a longitudinal area of yellow discoloration extending most of the length of the nail. Head-on view of the nail unit revealed a focal overcurvature of the nail plate and a localized subungual hyperkeratosis, mimicking thickening of the nail plate. However, the distinct honeycomb pattern typical of onychomatricoma was absent. On closer examination, the head of a red nodule was visible with a distal horny cap, which had lifted the nail plate with destruction of the nail plate distally (Fig. 1A). The lesion was tender to pressure. The other nails appeared normal, and palpation revealed no regional lymphadenopathy. Radiography showed a soft-tissue swelling without periostitis or bone erosion. The plaque measured grossly 2 × 1.3 × 1 cm and extended from the matrix to the hyponychium. Removal of the lesion was performed with a longitudinal incision.
Histopathologically, the tumour was superficially relatively well-demarcated, with pushing margins separated from the nail epithelium by a thick dermis (Fig. 1B). The deeper borders of the tumour were irregular, with short fascicles infiltrating the sub-nail region. The tumour was composed of bland-looking spindle cells arranged in a vague storiform pattern within a myxoid stroma interspersed with wispy collagen bundles (Fig. 1B, C). The abundant vessels were small-to-medium size with thick hyalinized walls (Fig. 1C). There was no cellular atypia and no mitotic figures were found. Numerous mast cells were seen scattered within the myxoid stroma. Nodule of adipose tissue was not observed. Tumour cells displayed strong positivity for CD34, CD10, and focal staining for bcl2 (B-cell lymphoma 2) and p16 (a protein coded by the cyclin-dependent kinase inhibitor 2A gene (CDKN2A), but were negative for nestin, CD99, EMA (epithelial membrane antigen), MUC4 (mucin 4), smooth muscle actin, desmin, oestrogen/progesterone receptors and androgen receptors. Most of the tumour cells were positive for mouse double minute 2 (MDM2) but negative for cyclin dependent kinase 4 (CDK4).
FISH analysis ruled out myxoid dermatofibrosarcoma protuberans (DFSP). Array-comparative genomic hybridization (aCGH) analysis (Fig. 1D) showed only losses of chromosomal segments, notably losses of the long arms of chromosome 13 (including the RB transcriptional corepressor 1 gene, RB1) and chromosome 16. Notably, there was no MDM2 amplification, despite positivity for MDM2 in immunohistochemistry.
The overall findings were consistent with a diagnosis of CAF. The tumour was completely excised with free margins. No evidence of recurrence with 8 months of follow-up was observed.
Fig. 1. (A) Subungual lesion deforming the nail plate of the right big toe. (B) Scanning power (×40) showing a relatively well circumscribed subdermal nodule separated from the nail bed epithelium by a thick nail-bed dermis. The lesion was composed of fascicles of spindled cells embedded in myxoid stroma. (C) Higher magnification (×200) of the prominent vascularization with thick-walled, concentrically, hyalinized vessels. (D) Comparative genomic hybridization on array (aCGH) results: quantitative whole-genome profile showing partial losses of chromosomes 6q, 10p, 13q, 16q and 20p (log ratio –0.50). Black line represents the ratio of intensity of cyanine 5 and cyanine 3, corresponding to the tumour DNA and to the human reference DNA, respectively.
We describe here the first case of subungual CAF as a single-digit longitudinal overcurved xanthonychia with destruction of the nail plate distally. The differential diagnosis was broad, including onychomatricoma and squamous cell carcinoma. CAF is a rare soft-tissue tumour characterized by 2 main components: bland spindle cells and small-to-medium-sized vessels with mural hyalinization (1, 2). Similar to CAF, LGFMS and myxoid DFSP are composed of monomorphous spindle cells without atypia embedded in alternating collagenous and myxoid stroma. However, the vessels with thick walls seen in CAF are not typical of LGFMS and DFSP.
By far the most difficult clinical and histopathological diagnosis of CAF is acral myxoid DFSP. Location of DFSP on the toe is not uncommon (4) and the immuno-phenotyping profile of CAF and myxoid DFSP are similar (5, 6). In our case, a diagnosis of DFSP was ruled out because we did not observe the characteristic collagen type I alpha 1 chain (COL1A1)-platelet derived growth factor subunit B (PDGFB) fusion gene using FISH analysis with a COL1A1-PDGFB fusion probe. MUC4 is a highly sensitive and quite specific marker for LGFMS (7). In our case, the lack of expression of MUC 4 permitted this diagnosis to be eliminated.
Recently Chen & Fletcher have proposed using overexpression of p16 as a helpful tool to detect atypical or sarcomatous component in CAF (1). In contrast, usual cellular angiofibroma shows a scattered or negative expression of p16 (1), as in our case.
Histological differential diagnosis of CAF should also include those tumours that typically arise on digits and have clinical and histopathological features that overlap with those of CAF, such as superficial acral fibromyxoma (SAF), cellular digital fibroma (CDF) and acquired reactive digital fibroma (ADF) (8). SAF does not show a homogeneous vascular pattern of hyalinized vessels through the tumour (8, 9).
In contrast to CAF, SAF shows, beside CD34 expression, a homogeneous reactivity for nestin, CD99 and a focal reactivity for EMA, whereas bcl2 is negative (8). Homogeneous reactivity for CD99 is a nearly consistent finding and nestin is the most sensitive marker for SAF (8).
CDF and ADF were ruled out because of the presence of alternating hypercellular and hypocellular areas, and mammary-type myofibroblastoma, angiomyofibroblastoma based on negative staining for desmin (1, 2).
CAF belongs to the RB1-deficient benign mesenchymal lesions (2), which usually include spindle cells/pleomorphic lipoma and mammary-type myofibroblastoma. Notably, these 3 entities share the same quantitative genomic profile with partial monosomies 13q and 16q (10). Recently, some cases of SAF have been described harbouring RB1 gene deletion (9). In the present case, the genomic profile was similar to those observed in RB1-deficient benign mesenchymal tumours, allowing a definitive diagnosis of CAF to be made. To the best of our knowledge, this is the first genomic study of a CAF (from all locations) using aCGH analysis. Thus far, cytogenetic or molecular studies of cellular angiofibroma have been limited to karyotyping and/or FISH analyses (10, 11).
In summary, we present here a case of CAF showing typical histological, immunohistochemical and genetic features. The extragenital location is classically rare and, indeed, a subungual location is exceedingly uncommon.
CAF is a unique entity, which must be distinguished from SAF and other CD34 positive, RB1-deficient fibrous neoplasms, as CAF can present discrete microscopic nodules showing atypical cellular features of pleomorphic liposarcoma or pleomorphic spindle cell sarcoma. Therefore, for CAF, the literature suggests radical excision with free margins (1). In contrast, for SAF and other CD34-positive, RB1-deficient fibrous neoplasms, simple local excision or “shelling out” of the lesion appears to be adequate and effective to avoid recurrences and injuries to surrounding tissue (2, 8, 9).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize