


Department of Dermatology, The Second Affiliated Hospital, School of Medicine, Xi’an Jiaotong University, Xi’an 710004, China. *E-mail: gsm312@yahoo.com
A 28-year-old man presented with multiple asymptomatic papules and plaques on his face for 3 months. He denied any drug intake, allergy or trauma history. A dermatological examination revealed clusters of yellowish-erythematous papules and plaques on his face and scalp (Fig. 1). No lymph-adenopathy or visceromegalies were found. Routine laboratory tests, chest radiography and abdominal ultrasound revealed no obvious abnormalities. Biopsy of a lesion from his cheek showed a nodular mixed inflammatory infiltrate throughout the dermis (Fig. 2a). The infiltration consisted of clustered large foamy-appearing histiocytes, numerous lymphocytes, plasma cells and few neutrophils. Emperipolesis in histiocytes was noted (Fig. 2b). Immunohistochemical studies showed that the pale cells were positive for S100 (Fig. 2c) and CD68, but negative for CD1a. Specific stainings for microbial infections were negative.
What is your diagnosis? See next page for answer.
Fig. 1. Clusters of yellowish-erythematous papules, which partially coalesced into verrucous plaques on the patient’s face and nearby scalp. Written permission from the patient is given.
Fig. 2. (a) A dense nodular mixed inflammatory infiltrate in the dermis and subcutaneous tissue (haematoxylin and eosin; HE ×100). (B) The infiltration consisted of mainly large histiocytes with emperipolesis (black arrow), lymphocytes, and few neutrophils (HE ×400). (C) S100-protein was positive and confirmed emperipolesis (white arrow) (immunohistochemistry; IHC ×400).
Acta Derm Venereol
Diagnosis: Cutaneous Rosai-Dorfman disease
The patient was given oral methotrexate, 15 mg once weekly, and significant improvement was noted after the subsequent 10-month follow-up with a tapered dose (Fig. 3).
Rosai-Dorfman disease (RDD), or sinus histiocytosis with massive lymphadenopathy (SHML), is a benign proliferative disorder of histiocytes (1). Skin is the most common site of extranodal involvement (2). In approximately 3% of patients only the skin is involved with no lymphadenopathy or systemic symptoms, termed cutaneous Rosai-Dorfman disease (CRDD) (3, 4). CRDD tends to affect older people (mean age 46 years) with a slight female preponderance (12:9), and it has more morbility in Asian patients (4, 5). Although the exact cause of CRDD remains unknown, some infectious agents and other immunological factors were associated with CRDD. One patient developed CRDD at the injection site after vaccination. This suggests that CRDD probably represents an immunological reaction pattern that can be triggered by various agents (4, 6).
CRDD lacks a constant clinical appearance. Skin lesions range from patches, papules, plaques, and pustules, to nodules with erythematous (most commonly), brownish, grey-blue, violaceous, or yellowish discoloration. The most common features are an infiltrated central noduloplaque with surrounding satellite papules (4, 7). Due to its variable appearance, several different descriptions have been used to portray the skin lesions, including psoriasiform, xanthomatous, acneiform, rosacea-like, vasculitis-like, granuloma annulare-like and pseudotumour-like lesions (4, 8). However, rosacea-like and acneiform lesions together with asymptomatic, yellow-erythematous coalesced papules, as in our case, were rarely reported. To the best of our knowledge, only 2 cases have reported such lesions (8, 9).
The most characteristic histological features of CRDD are nodular/diffuse infiltration of histiocytes with sparse lymphocytes, plasma cells, neutrophils, and eosinophils throughout dermis or subcutaneous tissue with minimal epidermal changes (4, 7). Immunohistochemically, histiocytes are positive for S100, and CD68, but negative for CD1a. The presence of emperipolesis (engulfment of intact lymphocytes, rarely plasmocytes, neutrophils, or erythrocytes within histiocytes) can be stressed by positive S100 protein (4). Histiocytic emperipolesis is a characteristic, although not unique, feature, as it can also be observed in other conditions, such as reticulohistiocytoma, malignant histiocytosis, and Langerhans cell histiocytosis, which should be differentiated from CRDD (10).
CRDD generally follows a benign clinical course with a tendency to spontaneous regression, thus treatment is not usually required. For solitary or localized lesions, surgical excision is the most effective treatment (7). Other diverse treatment options, including corticosteroids, dapsone, thalidomide, isotretinoin, and methotrexate, have been reported to control the extensive cutaneous disease (6, 7, 11). Al-Khateeb (12) found that corticosteroids were the least effective treatment for CRDD. However, low-dose methotrexate has been found to be an effective treatment (11, 13). The current patient initially demonstrated resistance to prednisone but then responded well to methotrexate.
Fig. 3. Ten months after initiation of treatment with methotrexate. Written permission is given.


 Click to show fullsize
Click to show fullsize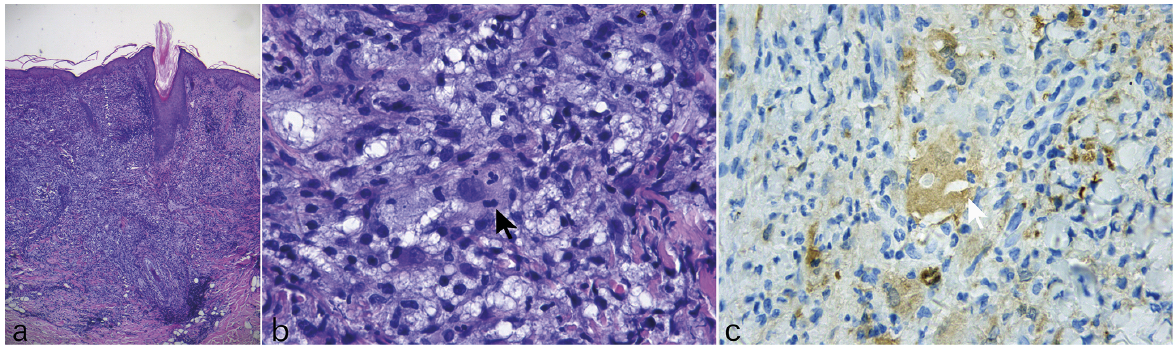 Click to show fullsize
Click to show fullsize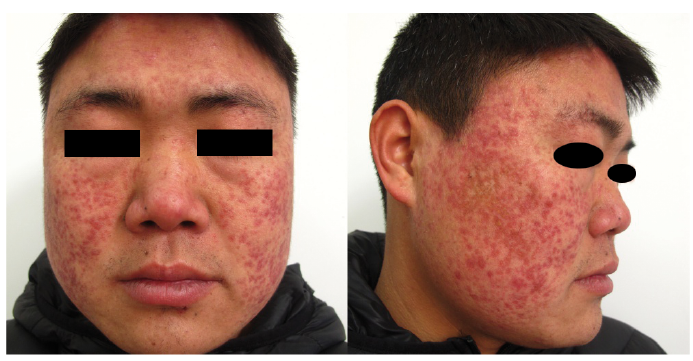 Click to show fullsize
Click to show fullsize