


Departments of 1Dermatology and 3Hematology, Imamura General Hospital, and 2Department of Dermatology, Kagoshima University Graduate School of Medical and Dental Sciences, Kagoshima Japan
Cutaneous-type adult T-cell leukemia-lymphoma is treated with antiviral or skin-directed therapy.
Medications that are used to treat skin lesions of cutaneous T-cell lymphomas are also used for the cutaneous-type adult T-cell leukemia-lymphoma. Etretinate, a synthetic retinoid, has been used for treating cutaneous T-cell lymphomas; however, its clinical effectiveness for the treatment of cutaneous-type adult T-cell leukemia-lymphoma has not been fully studied. We conducted a retrospective assessment of the efficacy and safety of etretinate in 9 patients with cutaneous-type adult T-cell leukemia-lymphoma. Complete and partial responses to etretinate were observed in 1 and 7 patients, respectively. Among the responders, remission was maintained for more than 6 years in 2 patients. These results suggest that etretinate is a promising treatment option for cutaneous-type adult T-cell leukemia-lymphoma.
Key words: adult T-cell leukemia-lymphoma; etretinate; retinoid; cutaneous type.
Accepted Apr 16, 2019; E-published Apr 16, 2019
Acta Derm Venereol
Corr: Kentaro Yonekura, MD, PhD, Department of Dermatology, Imamura General Hospital, 11-23 Kamoikeshinmachi, Kagoshima 890-0064, Japan. E-mail: ke.yonekura@jiaikai.jp
Cutaneous-type adult T-cell leukemia-lymphoma is a peculiar subgroup of smoldering adult T-cell leukemia-lymphoma associated with cutaneous lesions. Patients with the cutaneous-type adult T-cell leukemia-lymphoma are primarily treated with skin-directed therapy, similar to those with cutaneous T-cell lymphomas. However, once they become resistant to this treatment, the subsequent treatment options are limited. In this original article, we report the results of our retrospective study: etretinate, a synthetic retinoid analogue, which is widely used for the treatment of cutaneous T-cell lymphomas, is highly effective in treating cutaneous-type adult T-cell leukemia-lymphoma.
Etretinate, a synthetic retinoid analogue, is widely used for the treatment of cutaneous T-cell lym-phomas (CTCLs) as a monotherapy or in combination with other therapies, such as ultraviolet radiation (1, 2). Cutaneous-type adult T-cell leukemia-lymphoma (cATL) is a peculiar subgroup of smoldering-type ATL in which the skin is predominantly affected (3). Patients with cATL are primarily treated with skin-directed therapy, similar to those with CTCLs (2). In Europe and the USA, a combination therapy with interferon (IFN) alpha and azidothymidine (AZT) is available. However, in Japan, it is not yet approved and clinical trials are still underway (4, 5). A few reports have demonstrated the beneficial effects of etretinate in ATL and its off-label use in clinical settings (2, 6, 7). However, its efficacy in ATL has not been systematically evaluated. We demonstrate the clinical efficacy of etretinate in the treatment of cATL in our retrospective study.
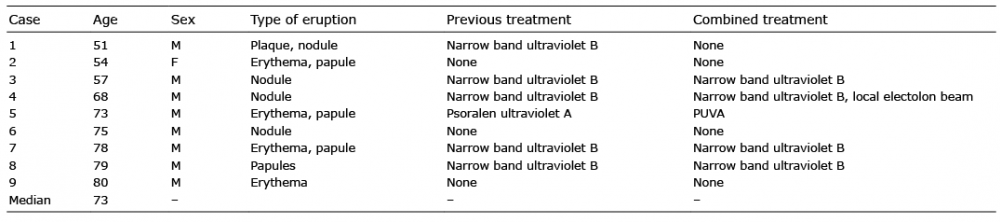
This study was approved by the human research ethics committee of our hospital and prior written informed consent was obtained from all participants. A total of 9 patients, 8 men and 1 woman, with a median age of 73 years (range 51–80 years), were enrolled into the study. They were treated with etretinate from April 2009 to July 2010. We followed-up these patients until August 2016 in our hospital (Table I). Their diagnosis, treatments, laboratory findings and therapeutic results were obtained from their clinical records. Considering that adequate consensus about the definite diagnostic criteria of cATL has not been obtained, in this study, we diagnosed cATL as the smoldering ATL, associated with cutaneous lesions. The response of cutaneous lesions to etretinate was evaluated by the modified severity weighted assessment tools (mSWAT) before and 3 months after the introduction of the treatment. There are types of ATL eruptions that cannot be assessed with mSWAT, because it was initially designed for assessment of mycosis fungoides and Sezary syndrome. We treated papules as plaques and nodules as tumors, considering the spread of the lesions vertically. Response to the treatment was recorded according to the modified response criteria for ATL (4). The long-term response of cutaneous lesions was evaluated by the physician’s global assessment (PGA), in which erythema, induration, papules, and nodules were taken into consideration. The severity of adverse reactions was evaluated according to the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE), version 3.0. Paired t-test was used for comparing the mSWAT scores before and after treatment. Progression-free survival (PFS) was defined as the time ranging from the start of etretinate treatment to disease progression. PFS was estimated using the Kaplan–Meier method. Statistical analysis was performed using Graphpad Prism 5 (Graphpad
Software, La Jolla, CA, USA) and p-values < 0.05 indicated statistical significance.
Table I. Patients characteristics
Before etretinate treatment, 6 patients received ultraviolet radiation, which was continued in 5 patients after the etretinate initiation. In one patient, local electron beam irradiation was carried out on a tumor lesion, which was excluded from the mSWAT evaluation (Table I). Treatment and observation periods were 3 to > 77 months (median > 16) and 8 to > 77 months (median > 24), respectively. The median mSWAT scores decreased significantly from 28 (ranging from 0.2 to 102.1) before treatment to 5.8 (ranging from 0 to 72) 3 months after the commencement of etretinate (Table II, Fig. 1; p = 0.0296, paired t-test,). The mSWAT score improved by more than 50% in 8 patients; after the 3-month treatment, complete response (CR) and partial response (PR) were seen in 1 and 7 patients, respectively (Table II). In the 8 responders, etretinate was discontinued due to disease progression in 2 patients and adverse events in 1 patient. Etretinate treatment was continued in the other 5 patients. CR and PR were maintained in 1 patient, each for more than 6 years, as evaluated by PGA (Table III). Median observation period was 16 months (range 8 to 77 months) and median PFS was 25 months (Fig. 2).
Table II. Clinical effect and laboratory data before and after etretinate treatment
Fig. 1. Modified severity weighted assessment tools (SWAT) score before and after 3 months treatment with etretinate. Modified SWAT scores are significantly improved after 3 months of etretinate treatment (p = 0.0296, paired t-test).
Table III. Long-term response
Fig. 2. Progression-free survival (PFS) after treatment with etretinate. Median PFS was 25 months.
Retinoids are structural and functional derivatives of vitamin A. Because they act as biological response modifiers, they are often used in cancer treatment. Retinoids bind to 2 kinds of receptors: retinoic acid receptors (RARs) and retinoid X receptors (RXRs). These are distinct families of nuclear receptors that regulate gene transcription. Each receptor comprises of 3 subtypes, α, β, and γ, which bind to specific ligands. Etretinate binds to RARs and promotes the transcription of genes, which regulate the terminal differentiation of malignant cells (8).
Patients with cATL require effective treatment because their quality of life (QoL) is impaired due to the visible cutaneous lesions. Treatments for CTCL have been applied for cATL due to their clinical and pathological similarities. Patients with cATL are managed with watchful waiting, antiviral therapy, using drugs such as AZT and IFN, skin-directed therapy such as ultraviolet radiation, local radiation with an electron beam, oral retinoid, or single-agent chemotherapy, using methotrexate, etoposide, or sobuzoxane (2). The use of antiviral agents in Japan is limited to clinical trials so far. A few clinical trials that used retinoids to treat ATL have recently been reported. Inozume et al. reported a case of cATL that was treated with etretinate. In this case, etretinate was started at a daily dose of 60 mg. The dose was gradually decreased and discontinued 34 months after achieving remission, which lasted 47 months (6). Senba-Nakata et al. reported a case of lymphoma-type ATL that progressed from a cutaneous-type ATL in an elder patient. They used etretinate, at a daily dose of 30–40 mg, in combination with 20 mg/day prednisolone, and observed a good response. This patient’s ATL was controlled well for one year (7). In a case series study, another synthetic retinoid, all-trans retinoic acid (ATRA), was administered to 6 patients with smoldering-type ATL that predominantly affected the skin. Two of the patients obtained PR without serious adverse events (9).
In the present study, etretinate was administered at a daily dose of 10–40 mg to 9 cATL patients. A high response rate was observed, as evidenced by the mSWAT scores and the modified response criteria for ATL, and remission was obtained in 8 patients. As this was a retrospective study with the limitations of the lack of controls, there may be biases owing to the compliance or case selection. However, these results reveal that etretinate is highly effective in treating cATL, as a monotherapy or in combination with phototherapy. We propose that oral retinoids are a safe treatment option for cATL patients. It improves their QoL by relieving the skin symptoms. To evaluate, whether etretinate contributes to an improved prognosis for cATL patients, further studies with a larger sample population are needed.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize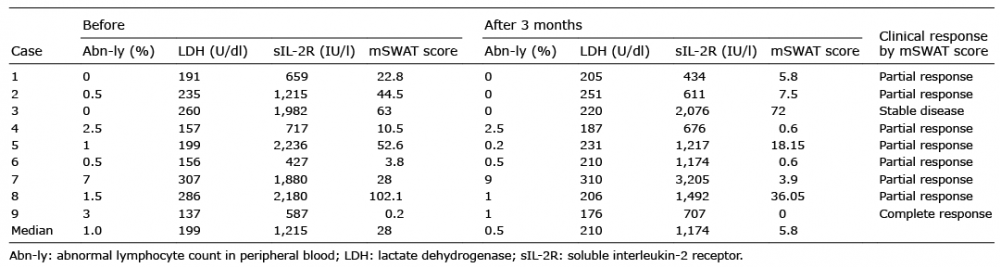 Click to show fullsize
Click to show fullsize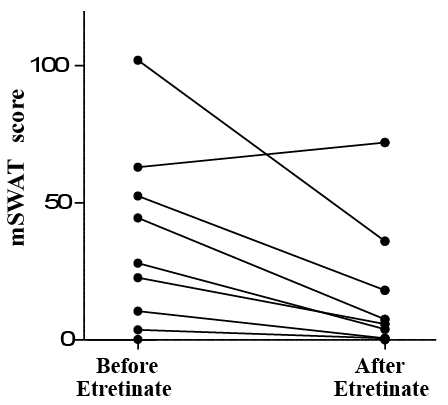 Click to show fullsize
Click to show fullsize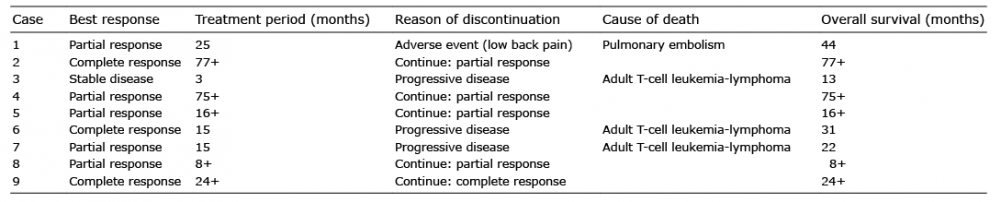 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize