


Department of Dermatology and Allergy, Charité – Universitätsmedizin Berlin, Charitéplatz 1, DE-10117 Berlin, Germany. *E-mail: martin.metz@charite.de
Accepted Jun 18, 2019; E-published Jun 24, 2019
Chronic prurigo (CPG) is a common and distinct skin disease defined by the presence of chronic pruritus, signs of repeated scratching and multiple pruriginous skin lesions (1). A large proportion of patients with CPG have dramatically impaired quality of life and are largely resistant to available therapy.
The pathophysiological mechanisms leading to CPG are currently unknown. Atopy is thought to play an important role, with approximately half of all patients with CPG having an atopic disposition (1). Furthermore, atopic dermatitis (AD) is the most frequent skin disease associated with CPG (2). It is important to note, however, that CPG is a distinct disease, which can evolve on the basis of an AD or other inflammatory skin disease, as well as various systemic disorders, and then co-exist or continue after their cessation (3). In most cases, CPG is thought to have a multifactorial or undetermined origin (4). Currently, there are no approved therapies available. Most patients receive insufficient therapies, consisting of topical anti-inflammatory treatments and systemic H1 antihistamines. Some patients are treated by specialist centres with off-label drugs, such as cyclosporine, anticonvulsants, μ-opioid- or neurokinin-1-receptor antagonists (5).
In many patients with CPG an atopic disposition can be observed, leading to a Th2-driven immune dysregulation. Furthermore, in many patients with CPG a pronounced superficial, perivascular and/or interstitial inflammatory infiltrate, composed mainly of lymphocytes, macrophages, and eosinophils, can be identified in lesional skin (6). The human mAb dupilumab, a monoclonal anti-IL-4Rα antibody, acts on both features. In AD, dupilumab has been shown to lead to a significant reduction in disease activity, as well as to a rapid, significant and clinically relevant improvement in pruritus (7). Based on these findings, dupilumab may be a beneficial treatment option for patients with CPG.
We report here 3 patients with CPG who were treated with dupilumab in our department within the last 12 months.
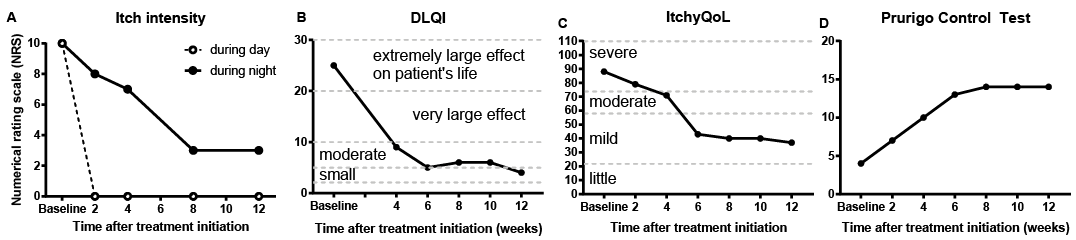
Patient 1. A 41-year-old man was diagnosed with nodular type CPG in 2016. The patient had a history of allergic asthma and multiple type I allergies, highly elevated total IgE of 14,778 kU/I and, at the time of first consultation, generalized eczema. At this time, the patient was diagnosed with AD, which was well controlled by ultraviolet B (UVB) 311 nm phototherapy and topical steroids. However, the patient continued to report extremely troublesome pruritus, along with continuous development of new CPG nodules. Different therapeutic approaches (see Table SI1) were unsuccessful, and the patient continued to experience severe pruritus. In December 2017, the patient reported constant pruritus with a maximum intensity of 10 on a numerical rating scale (NRS, 0–10), a major impairment in quality of life (Dermatology Life Quality Index (DLQI) score of 25, ItchyQoL Score of 88), and presented with numerous highly pruritic nodules and plaques. As cyclosporine treatment was not possible due to poorly controlled hypertension, treatment with dupilumab was initiated. The patient reported a significant improvement in symptoms 2 weeks after receiving the loading dose of 600 mg (Fig. 1). His condition continued to improve, and from week 6 after the start of dupilumab the patient reported a dramatic improvement in pruritus and prurigo control (Fig. 1A, D), only mild impairment in quality of life (Fig. 1B, C), and a slow, but steady, improvement in CPG lesions.
Fig. 1. Improvement in pruritus and quality of life during dupilumab treatment in a patient with chronic prurigo. (A) Maximum itch intensity during day and night. Dermatological and itch-specific quality of life impairment (DLQI, B; ItchyQoL, C), and level of disease control of chronic prurigo (Prurigo Control Test, D) were assessed during the patients’ visits every 2–4 weeks for up to 12 weeks. The patient has now been under treatment for > 9 months and shows a sustained response to dupilumab.
Patient 2. A 45-year-old woman was diagnosed with CPG of nodular type in 2015, with multiple chronic and extremely itchy excoriated nodules on her legs, buttocks and arms. The patient had an atopic history, including multiple type 1 allergies, dyshidrotic hand eczema, and allergic asthma. Despite numerous therapeutic attempts (Table SI), the patient reported constant pruritus, with a maximum intensity of 10 (NRS), and a major impairment in quality of life (DLQI score 29). Previous treatment with cyclosporine had to be discontinued twice due to elevations in serum creatinine, and we therefore initiated dupilumab therapy. In her first follow-up visit after 4 doses (8 weeks later), the patient reported a significant improvement in pruritus with a maximum itch intensity of 0 on the NRS and a DLQI score of 10, which further decreased to a score of 2 after a further 3 months (Table SI).
Patient 3. A 52-year-old man with an atopic history including multiple type 1 allergies, dyshidrotic foot eczema and AD, had first presented to our clinic in 2017 with multiple extremely itchy excoriated nodules on both legs. Despite a 3-year treatment with cyclosporine and the addition of gabapentin, the patient had severe pruritus and a major impairment in quality of life with a DLQI score of 19, an ItchyQoL score of 91 and a maximum itch intensity of 10 (NRS). Both cyclosporine and gabapentin were then discontinued and we initiated treatment with dupilumab. Two weeks after initiation of treatment, the DLQI decreased to 14 points and the ItchyQol to 74. Three months later, the patient reported a mild improvement in the pruritus and a further slow, but continuous, improvement over the next 3 months, with a 6-point reduction in maximum itch intensity to 4 in the NRS and a DLQI score of 12 (Table SI).
In order to better assess the efficacy of dupilumab in CPG, a newly developed tool, the Prurigo Control Test (PCT), was used in all 3 patients. The PCT is a patient-reported outcome instrument for monitoring disease control in patients with CPG, which works similarly to the well-established Urticaria Control Test (8, 9). The PCT comprises 5 questions pertaining to skin lesions, frequency of scratching, impairment of sleep and quality of life, and the general efficacy of the current treatment within the last 2 weeks. The answer to each question is scored 0–4 points, so that the final score of the PCT ranges from 0 (no disease control) to 20 (complete control of the disease). To date, the PCT is not a validated instrument, but the manuscript on the validation process, including a validation study with 100 patients with prurigo, is currently in preparation. Prior to the initiation of dupilumab treatment, the patients had PCT scores of 4, 0 and 2, respectively, indicating uncontrolled CPG. During the course of dupilumab treatment the PCT score increased gradually and reached 14, 17 and 10, respectively (Table SI).
In recent months, 3 other reports of successful treatment of patients with CPG using dupilumab have been published (10–12). All case reports (totalling 11 patients with CPG) have in common that most patients have had chronic prurigo for many years and that numerous different therapies have previously been carried out without success (Table SI). Overall, the onset of improvement after initiation of dupilumab treatment appears to vary. In most patients, a clinically significant reduction in pruritus occurred within 4 weeks, with further improvement in both pruritus and skin lesions over subsequent months.
The observed improvement in signs and symptoms during anti-IL4Rα therapy in our patients and those reported in the literature, indicates that pruritus in CPG is mediated, at least in part, by IL-4 and/or IL-13. This is in line with the observation of increased expression of IL-4 mRNA in the skin of patients with prurigo, although the clinical relevance of this is, as yet, unclear (13). Recently, Oetjen et al. have shown that IL-4Rα, as well as IL-13Rα and IL-31Rα, are expressed in human dorsal root ganglia (DRG) and that stimulation with IL-4 and IL-13 can lead to the direct activation of DRG neurones (14). Further clinical trials should investigate whether anti-IL4Rα treatment is, in general, of benefit for patients with CPG, regardless of their atopic background. Such investigations might also help to better understand the pathogenic mechanisms of CPG. In conclusion, the cases presented here and the published case reports suggest that CPG can be treated successfully with dupilumab at the dosage recommended for patients with AD.


 Click to show fullsize
Click to show fullsize