


1First Department of Dermatology, Aristotle University, 124 Delfon Street, Thessaloniki, and 2State Department of Dermatology, Hospital for Skin and Venereal Diseases, Thessaloniki, Greece. *E-mail: emlallas@gmail.com
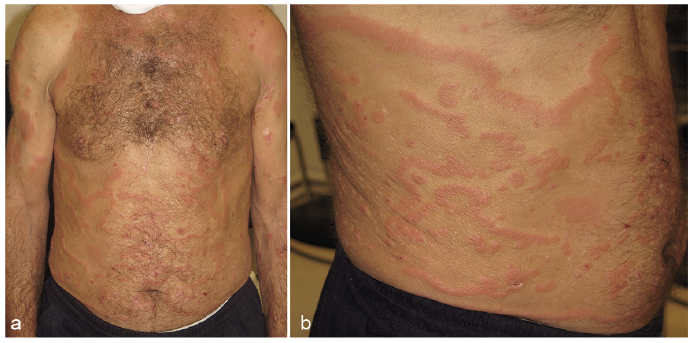
A 65-year-old man presented with a widespread skin rash on his trunk, back and proximal extremities. The patient reported that the eruption had first appeared 3 weeks earlier and had rapidly became widespread, following a migrating course with alternating zones of healing and new lesions. The eruption was mildly pruritic, but no other symptoms were reported, and the patient was in good physical health. Physical examination revealed parallel wavy bands of slightly elevated erythema, which were characteristically concentric. Fine scales were trailing the leading edge of the erythematous plaques. The eruption was spread on the trunk, back and proximal extremities, whereas the hands, feet and face were spared (Fig. 1).
Topical steroids and oral antihistamines had been administrated during recent weeks with no benefit. The patient’s history was free of similar skin eruptions or other dermatological diseases. It was also free of chronic diseases and surgical operations. He was not under any medication and had not received any medications recently. Basic laboratory evaluation did not reveal any remarkable findings.
What is your diagnosis? See next page for answer.
Fig. 1. Clinical photographs. (A) Widespread parallel, serpiginous wavy bands of slightly elevated erythema. (B) Close-up highlights concentric arrangement of the erythematous bands.
Acta Derm Venereol 2019; XX: XX–XX.
Diagnosis: Erythema gyratum repens
Serological examination for Lyme disease was negative, and IgE levels were normal. A biopsy was taken and histopathological examination revealed hyperkeratosis, parakeratosis, acanthosis and mild spongiosis. Perivascular lymphohistiocytic infiltrate was also found in the papillary dermis. Although the histopathological findings were unspecific, combined with the clinical manifestations they were assessed as compatible with erythema gyratum repens (EGR). Since the latter erythema is almost always a paraneoplastic manifestation, a search for internal malignancy was initiated immediately.
Palpation of the cervical lymph nodes revealed a slightly palpable lymph node on the left side of the patient’s neck. Lymph node biopsy was performed and was suggestive of metastatic deposits from a, previously undetected, primary tumour. Clinical examination, laboratory examination and initial imaging tests (computed tomography (CT) and magnetic resonance imaging (MRI)) did not reveal any finding that could be indicative of a malignant tumour. However, a few days later, lung scintigraphy revealed bronchial lung cancer.
The tumour stage was assessed as loco-regionally too advanced for surgery and the patient was treated with radiotherapy followed by chemotherapy. The patient responded well to treatment and after initial remission of the primary tumour, the skin lesions disappeared within the following weeks. No recurrence of the eruption was reported subsequently, although the patient died 2 years later due to widespread metastatic disease.
EGR was first described by Gammel in 1953 (1) and is considered as one of the most specific paraneoplastic syndromes, since the majority of patients (83%) reported with EGR had an associated internal malignancy (2). Bronchial carcinoma (32%) is the most commonly associated tumour, followed by oesophageal cancer (8%). Other underlying neoplasms include breast, uterus, bladder, cervix, prostate, and upper gastrointestinal tract cancer, as well as multiple myeloma (3). Rarely, EGR may be associated with pulmonary tuberculosis, drug intake or other pre-existing papulosquamous disorders.
Diagnosis of EGR is based on clinical findings. It typically presents with a serpiginous macular/papular pattern predominantly on the trunk and extremities and rarely involves the face, hands and feet. It has been reported to expand peripherally at a strikingly rapid rate, estimated at 1 cm/day. Numerous bands arranged in a parallel configuration result in the typical wood-grained appearance. Scale and pruritus are usually present. Additional skin manifestations might include palmoplantar hyperkeratosis, dystrophic nails, ichthyosis of the peripheral extremities, non-specific vesicles and bullae, and CREST syndrome (2). It remains unclear whether the latter cutaneous manifestations have a causal relationship to the primary tumour or represent manifestations associated with EGR itself. However, the fact that several of these skin manifestations have been reported also to co-exist with EGR not associated with malignancy, supports the second hypothesis (4).
Considering the very high probability of an underlying tumour, the diagnosis of EGR should warrant an exhaustive search for internal cancer. However, a recent review suggested that up to 30% of cases of EGR are not associated with underlying neoplasms (4). Antihistamines are often used to control the pruritus, but no specific treatment has been suggested as effective for EGR. The erythema typically resolves with remission of the primary tumour. The most effective therapy for EGR is therefore to identify and treat the primary cause (5).


 Click to show fullsize
Click to show fullsize