


1Lund University, Department of Occupational and Environmental Dermatology, Skåne University Hospital, Malmö, 2Department of Public Health and Clinical Medicine, Dermatology & Venereology, Umeå University, Umeå, 3Department of Dermatology, Sahlgrenska Academy at the University of Gothenburg, Gothenburg, 4Division of Dermatology and Venereology, Ryhov County Hospital, Jönköping, and 5Occupational and Environmental Dermatology, CAMM, Stockholm County Council and Institute of Environmental Medicine, Karolinska Institute, Stockholm, Sweden
This study investigated whether more patients with contact allergies were detected by patch testing with mercapto mix with a higher concentration of 2-mercaptobenzothiazolinone (MBT) than the commonly used mercapto mix. A total of 3,143 dermatitis patients in 5 Swedish dermatology departments were patch- tested with 3 mercapto test preparations: MBT 2.0% petrolatum (pet.); mercapto mix 2.0% pet.; and mercapto mix 3.5% pet. Positive reactions to these mercapto mixes varied between 0–0.50%, 0–0.93%, and 0–1.4%, respectively, in the 5 centres. Numerically, mercapto mix 3.5% pet. detected all positive patients and more patch-test positive patients than did the 2 other substances, but the difference was not statistically significant. The authors recommend replacing mercapto mix 2.0% pet. in the Swedish baseline series with mercapto mix 3.5% pet., since the latter also detected those patients who would have been missed because MBT 2.0% is not included in the Swedish baseline series.
Key words: allergic contact dermatitis; contact allergy; 2-mercaptobenzothiazole; mercapto mix; rubber; delayed hypersensitivity.
Accepted Jun 25, 2019; E-published Jun 26, 2019
Acta Derm Venereol 2019; XX: XX–XX.
Corr: Marléne Isaksson, Department of Occupational and Environmental Dermatology, Jan Waldenströms gata 18, level 6, SE-205 02 Malmö, Sweden. E-mail: marlene.isaksson@skane.se
Mercaptobenzothiazole compounds are used as accelerators in rubber products. These compounds are associated with causing allergic contact dermatitis. Various mercaptobenzothiazole compounds have been tested to find the optimal test substance, both single substances and mixes of mercaptobenzothiazole compounds, for use in patch testing patients. This study compared the results of patch testing 3,143 patients with mercaptobenzothiazole mix 3.5%, mercaptobenzothiazole 2% and mercaptobenzothiazole mix 2% to find out what proportion of allergic individuals were detected with the 3 different mercapto test preparations. Mercaptobenzothiazole mix 3.5% detected all positive patients and detected more patch test positive patients than did the 2 other substances. The authors therefore recommend replacing mercaptobenzothiazole mix 2.0% in the Swedish baseline series with mercaptobenzothiazole mix 3.5%.
Mercaptobenzothiazole (MBT) compounds are primarily used as accelerators in rubber products. These compounds are associated with causing allergic contact dermatitis. MBT are also used as fungicides and in machine coolants. In order to investigate possible rubber dermatitis, 2-mercaptobenzothiazole in 2% petrolatum (pet.) was included in the very first baseline series for patch testing proposed by the International Contact Dermatitis Research Group (ICDRG) in 1968 (1, 2). As the use of other MBT derivatives as accelerators increased, new screening substances were introduced for patch testing and, in the 1970s, MBT was replaced in the ICDRG baseline series by a mix which, in addition to MBT, consisted of N-cyclohexyl-2-benzothiazyl sulphenamide, 2,2’-dibenzothiazyl disulphide and 2-(4-morpholinyl) MBT (3, 4). This mix, commonly known as mercapto mix, has since been used for patch testing in different compositions and concentrations in several different baseline series.
Principally, 3 different mercapto mixes have been used: (i) a 3-part mix consisting of 0.33% each of the 3 additional substances listed above, but no MBT (total concentration 1.0%); (ii) a 4-part mix consisting of 0.25% of each of the above-mentioned haptens (total concentration 1.0%); and (iii) a 4-part mix consisting of 0.50% of each of the above-mentioned haptens (total concentration 2.0%) (5). In many baseline series both the mercapto mix at 2% (w/w) pet. and MBT 2% (w/w) pet. are tested in parallel (3, 6). However, in the Swedish baseline series only mercapto mix at 2.0% pet. is tested, including MBT at 0.5%.
The aim of this study, conducted by the Swedish Contact Dermatitis Research Group (SCDRG), was to explore the possibility of patch testing with a mercapto mix in which the concentration of MBT corresponds to the one used when MBT is patch-tested on its own (Table I). Hence, the aim was to compare whether mercapto mix at 3.5% (w/w) pet. detects as many positive patients as patch testing with mercapto mix at 2.0% pet. and MBT at 2.0% pet., respectively, in parallel. If only one preparation is needed to screen for contact allergy due to MBT compounds, space would be saved on the patient’s back, enabling wider screening of other haptens.
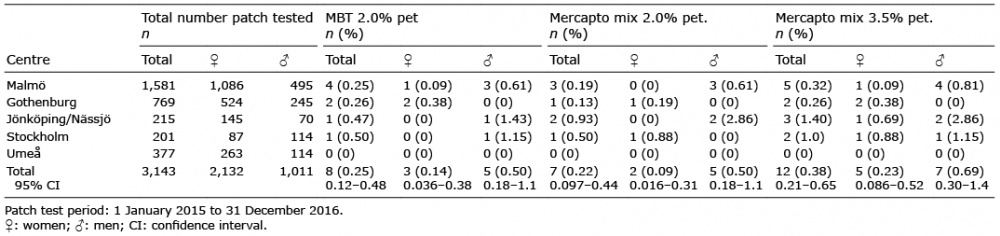
Table I. Positive patch test reactions on days 3 or 4 and/or on days 7, or 8 when patch testing with 2-mercaptobenzothiazole (MBT) 2.0% (w/w) pet., mercapto mix 2.0% (w/w) pet., and mercapto mix 3.5% (w/w) pet. in 5 different patch test centres
Study population
The study was conducted by the SCDRG. Five Swedish dermatology clinics took part during the period 1 January 2015 to 31 December 2016 (Table II). The participating clinics were located in Malmö, Gothenburg, Jönköping/Nässjö, Stockholm, and Umeå. The results are based on consecutive patch testing of 3,143 patients with suspected allergic contact dermatitis (2,132 females and 1,011 males; mean age 44.6 years; age range 7–92 years; females/males 67.8/32.2%).
Table II. Specification of petrolatum patch-test preparations used, their content of 2-mercaptobenzothiazole (MBT), and the frequency of positive patch tests in the study population
Substances
All patch-test preparations used in the study are listed in Table I and specified with regard to their content. The preparations containing MBT 2.0% (w/w) pet. and mercapto mix 2.0% (w/w) pet. were purchased from Chemotechnique Diagnostics (Vellinge, Sweden) by the Malmö department and distributed to the other participating clinics. The preparation of mercapto mix 3.5% (w/w) pet. was prepared by the Malmö department by spiking the commercial preparation of mercapto mix 2.0% (w/w) pet. (Chemotechnique Diagnostics) with MBT purchased from Sigma-Aldrich Chemie GmbH (Steinheim, Germany).
Patch testing
Patch testing and reading patients’ results was carried out according to the routine of the participating clinics. Finn Chambers® (8-mm diameter; SmartPractice, Phoenix, AZ, USA) on Scanpor® tape (Norgesplaster, Vennesla, Norway) were used in all centres except Gothenburg, which used IQ Ultra chambers (8×8 mm; Chemotechnique Diagnostics) on a hypoallergenic surgical tape. A dose of 20 mg was applied for the Finn Chamber (7) and 25 mg for the IQ Ultra. The chambers were applied to the patient’s back, occluded for 48 h, then discarded. Readings were classified according to ICDRG guidelines (8). All patients’ results were read twice; on day (D)3 or 4 and on D7 or 8. A dermatologist read all patch tests on both days in all centres, except Umeå, where a nurse trained in patch-test readings took the first reading and a dermatologist the second one. Any positive reaction (+, ++, +++) on D3, D4, D7 or D8 was registered as a positive reaction.
Statistical analysis
McNemar’s 2-sided test was used to compare the rates of positive reactions with: (i) mercapto mix 3.5% pet. and mercapto mix 2.0% pet.; (ii) mercapto mix 3.5% pet. and MBT 2.0% pet.; as well as (iii) mercapto mix 3.5% pet. and mercapto mix 2.0% pet. plus MBT 2.0% pet. Fisher’s exact test, 2-sided, was used to compare the number of contact allergy cases in females and males for the 3 patch test preparations. The 95% confidence intervals of frequencies of contact allergy were calculated using mid-p exact test and OpenEpi (http://openepi.com). A p-value < 0.05 was considered to be significant.
The number of patch-tested individuals in each centre, as well as the rates of positive reactions to the investigated preparations, are shown in Table I. Overall, the rate of contact allergy to mercapto mix 2.0% pet., MBT 2.0% pet., and mercapto mix 3.5% pet. varied between 0–0.93%, 0–0.50% and 0–1.4%, respectively, in the 5 test centres. Numerically, mercapto mix 3.5% pet. detected more patch-test positive patients than did the other 2 substances, but the difference was not statistically significant (mercapto mix 2.0% pet., p = 0.074; MBT 2.0% pet., p = 0.13). If both mercapto mix 2.0% pet. and MBT 2.0% pet. are tested in parallel and both must be positive, the difference from the results for mercapto mix 3.5% is significant (p = 0.013).
The distribution of exclusive and concurrent reactions to the 3 preparations are shown in Fig. 1. Mercapto mix 3.5% pet. detected all patients who reacted to either mercapto mix 2.0% pet. or MBT 2.0% pet. If mercapto mix 2.0% pet. alone had been tested 33% (4/12) of the patients would have been missed. The corresponding figure if patch testing is performed with both mercapto mix 2.0% and MBT 2.0% 8.3% (1/12) patients would have been missed. All reactions were read twice; on both D3 or D4 and on D7 or D8. If readings had only been performed on D3 or D4 14% (1/7) of the patients positive to mercapto mix 2.0%, and 8% (1/12) of the patients positive to mercapto mix 3.5%, would have been missed. All 8 patients positive to MBT 2.0% reacted already by D3 or D4. Statistically significantly more men than women were positive to mercapto mix 2.0% pet. (p = 0.0387), whereas no statistically significant differences could be seen between the sexes for MBT 2.0% pet. (p = 0.156) or mercapto mix 3.5% pet. (p = 0.065). Doubtful reactions were seen to MBT 2.0%, mercapto mix 2.0%, and mercapto mix 3.5% in 0/3143 (0%), 9/3143 (0.3%), and 7/3143 (0.2%) dermatitis patients on D3 or D4. The corresponding figures for D7 or D8 are 1, 2, and 3/3143. No irritant reactions were registered for any of the substances investigated, and no suspected cases of patch-test sensitization were reported.
Fig. 1. Distribution of exclusive and concurrent reactions to mercapto mix 2.0% (w/w) pet., mercapto mix 3.5% (w/w) pet. and 2-mercaptobenzothiazole (MBT) 2.0% (w/w) pet. The numbers in the circles represent the number of patients with a positive test reaction to the respective test substance.
The patch test preparations in the baseline series have all been tested extensively and are optimized to cause the minimum possible disadvantageous reactions, i.e. they are tested in non-irritant and non-sensitizing concentrations. However, when a test concentration is increased there is always a risk that the new concentration will cause unwanted reactions. In order to minimize the risk of such reactions when testing with a mercapto mix with a higher content of MBT (i.e. mercapto mix 3.5%) a preliminary study was conducted at the Malmö department. This meant that the concentration of MBT was increased incrementally in the mercapto mix, up to 2%, and patch-tested in consecutively patch-tested dermatitis patients in a step-wise manner, ensuring that no adverse effects were seen before proceeding with a higher concentration. Thus, at first, 232 patients were tested with only one preparation, consisting of 1% MBT and 0.5% of the other 3 constituents of the regular mercapto mix 2.0% (mercapto mix 2.5%), thereafter 655 patients were tested with mercapto mix 2.5% pet. and an additional preparation consisting of 2.0% MBT and 0.5% of the other 3 constituents of the regular mercapto mix 2.0% (mercapto mix 3.5%). Since no signs of adverse effects were observed in the pre-study it was concluded that mercapto mix 3.5% pet. could be used in the larger multicentre study.
In a recent publication on how to improve the quality of multicentre patch test studies, 16 factors of possible significance for the patch-test result in multicentre patch-test studies were discussed (9). In addition to listing the 16 factors, a scoring system was also suggested, with various scores based on the relative importance of each factor for the quality of the multicentre patch-test study. In the current study, the highest scores were obtained for all factors, except for different patch-test techniques, lack of control of occlusion after 48 h, no calibration of the test-reading, and no monitoring. Despite this, the total score classified the current study as a multicentre patch-test study of high quality (9).
Several studies have compared patch test results with MBT 2.0% pet. and mercapto mix 2.0% pet. In 2006, Diepgen et al. (3) recommended that both MBT 2.0% and mercapto mix 2.0% should be included in the European baseline series when they presented data from a multicentre study in which 11 European centres participated. In that study, a total of 32,475 patients were tested; 0.22% (73/32475) were positive only to mercapto mix, 0.20% (66/32475) were positive only to MBT 2.0%, and 0.58% (188/32475) were positive to both preparations (3). In 2014, the North American Contact Dermatitis Research group presented concomitant reactions between MBT 2.0% pet. and mercapto mix 2.0% pet. for a total of 30,880 patients. They reported that 0.31% (98/30.882) were positive only to mercapto mix, 0.62% (192/30882) were positive only to MBT 2.0% and 0.76% (235/30882) were positive to both preparations, and concluded that MBT ought to be the preferential screening hapten for mercapto compounds (5). In the current study the same comparison results in 0.10% (3/3143) being positive only to mercapto mix 2.0%, 0.13% (4/3143) being positive only to MBT 2.0%, and 0.13% (4/3143) being positive to both preparations. Thus, in our material it is not evident that either MBT 2.0% or mercapto mix 2.0% is the preferred patch-test hapten. On the other hand, the high mercapto mix, i.e. 3.5%, detected all the patients who reacted to either of the 2 other preparations.
Although the high mercapto mix at 3.5% detected all the patients who reacted to either of the 2 other preparations, MBT 2.0% and mercapto mix 2.0%, the rate of allergic patients detected was 0.38% of all tested patients. The general recommendation is that a sensitizer should be included in a baseline series when the contact allergy rate in routinely tested dermatitis patients is 0.5% or higher (10). Although our rate is below 0.5%, this does not necessarily mean that the high mix should not be present in a baseline series. When comparing the pick-up rate of positive reactions to mercapto mix 2.0% with that of mercapto mix 3.5%, the p-value was 0.074, strongly indicating that the high mix is better in detecting allergic individuals, also taking into consideration the small number of such individuals. Since no allergic individuals were missed with the high mix, the authors recommend making changes to the baseline series in a step-wise manner and retaining use of the high mix for a few years. It should subsequently be considered whether mercapto chemicals have a place in the baseline series at all.
There is also a sex difference in the rate of contact allergy, with 3 times more males testing positively (0.69% vs. 0.23%, Table II). This may be due to men being more likely to have been exposed to non-rubber products containing MBT, such as cutting oils, greases, coolants, and fungicides (11). Until sufficient evidence is avai-able of better markers for this type of rubber allergy, the authors consider it is warranted to replace the mercapto mix 2.0% pet. with mercapto mix 3.5% pet., since the latter also detected those patients who would have been missed because MBT 2.0% is not tested in the Swedish baseline series. The frequency of doubtful reactions to MBT 2.0%, mercapto mix 2.0%, and mercapto mix 3.5% was low on D3 or D4, and even lower on later readings, and no irritant reactions were recorded for any of the 3 haptens. Consequently, the SCDRG will recommend the replacement of mercapto mix 2.0% pet. by mercapto mix 3.5% pet. in the Swedish baseline series from 2020.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize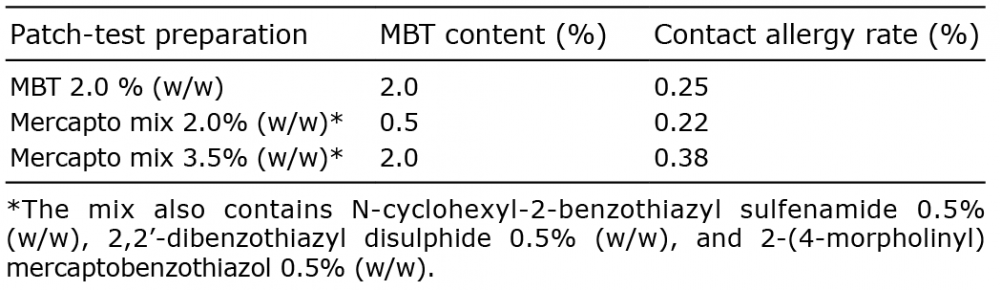 Click to show fullsize
Click to show fullsize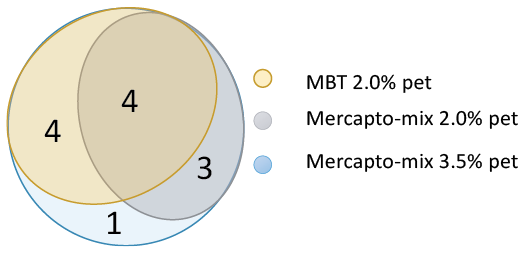 Click to show fullsize
Click to show fullsize