


Department of Dermatology, Le Mans Hospital, Le Mans, France
Changes in the duration of efficacy of botulinum toxin A injections for primary axillary hyperhidrosis have not been studied in depth. The aim of this study was to assess such changes. In a retrospective cohort of 220 patients, seen over a 17-year period, duration of efficacy was recorded, including duration of efficacy of first and last injections. Of 220 patients, 117 fulfilled the study criteria (79 females and 38 males, age 17–79 years, mean age 38.3 years). Patients received 3–24 injections (mean 5.5). The duration of efficacy of the first injections was 3 weeks to 30 months (median 6 months), and the duration of efficacy of the final injections was 3 weeks to 66 months (median 8 months) (p < 0.001). An increase in duration of efficacy occurred in 62% of patients with repeated injections. Of the 20 patients with a follow up ≥10 years, the mean number of treatments was 8.25/patient; in 18 of these patients the duration of efficacy increased by > 50%. In conclusion, repeated botulinum toxin A injections lead to an increase in duration of efficacy without secondary decrease.
Key words: hyperhidrosis; botulinum toxin; duration of efficacy.
Accepted Aug 26, 2019; E-published Aug 27, 2019
Acta Derm Venereol 2020; 100: XX–XX.
Corr: Hervé Maillard, Department of Dermatology, Le Mans Hospital, 194 Avenue Rubillard, FR-72037 Le Mans Cedex, France. E-mail: hmaillard@ch-lemans.fr
Hyperhidrosis consists of excessive sweating, which can negatively affect quality of life. Primary axillary hyperhidrosis is one of the most frequent causes of hyperhidrosis. Its treatment requires frequently repeated injections of botulinum toxin A (BTA). There are few published data on the repetition of BTA injections and its consequences. We report here a significant increase in the efficacy duration with the repetition of injections after more than 15 years of BTA treatment: 80% of patients reported a stable or increasing efficacy duration at the end of the follow-up, without side-effects.
Sweating is a physiological mechanism of thermoregulation. Hyperhidrosis consists of excessive sweating, which can negatively affect quality of life (1–3). The reported prevalence varied from 4.8% in the USA (4) to 14.5% in Shanghai, China, in 2016 (5).
Primary focal hyperhidrosis is defined by excess sweating for more than 6 months without any apparent cause that fulfils at least 2 of the following criteria: onset of symptoms during childhood or adolescence (< 25 years), occurrence of sweating independent of temperature, unforeseeably and not consciously controllable, focal occurrence in one or more sites of predilection with bilateral symmetry, occurrence of more than once a week that interferes with daily activities, absence of night sweats, and family history of the disease (6). The exact underlying mechanism is poorly understood, but it is thought to be linked to an important genetic disorder: Higashimoto et al. (7) showed a family history of hyperhidrosis in 42% of 456 patients with primary hyperhidrosis and found predisposing loci on chromosome 14q11.2-q13.
Several treatments are currently available, but they are not curative. A recent study on hyperhidrosis treatment (6) codified the therapeutic escalation. Topical therapy, such as aluminium chloride antiperspirants, should be the first line of treatment. In the second intention, several treatments can be proposed: iontophoresis, oral medication, or injection of botulinum toxin A (BTA). Another way to control hyperhidrosis is to destroy the sudoral glands using microwaves, called Miradry®, after local anaesthesia (8). Finally, the last treatment consists of thoracic sympathectomy by endoscopy for upper limb hyperhidrosis.
BTA is a neurotoxin that is produced by the bacterium Clostridium botulinum. Treatment with BTA injections works by irreversibly blocking the release of the neuro-transmitter acetylcholine from presynaptic bulbs at the neuromuscular junction (9). This leads to degeneration of the nerve endings, which can redevelop in a few weeks. This mechanism explains the temporary efficacy of this treatment from 4 to 25 months (10). Several studies have shown that the duration of the effect increases with the number of injections (10, 11). Conversely, other studies have suggested that this treatment can lead to the production of antitoxin antibodies in some patients (12). There are several suspected risk factors: a short duration between 2 series of BTA injections (less than 4 months), higher doses of BTA if the optimal efficiency is not reached, and a high cumulative dose (13).
There are few published studies on changes in the duration of the efficacy (DE) of BTA injections over time and favouring factors (14).
The aim of this study was to assess changes in the DE of BTA injections for PAH over time, as a function of the number of injections, and to assess the settings which can affect such changes.
The study retrospectively included patients with PAH from dermatology consultations of the Hospital of Le Mans, France, from May 2001 to April 2018. A clinical evaluation, consisting of a clinical examination, thyroid palpation, and determination of glycaemia and thyroid stimulating hormone levels, was carried out to exclude cases of secondary hyperhidrosis. Hyperhidrosis was detected by the Minor test. Local treatment (antiperspirants and/or iontophoresis) were unsucceful and patients had major psycho-social repercussions. All patients had a Hyperhidrosis Disease Severity Scale (HDSS) score > 2/4, meaning that hyperhidrosis interfered with daily activities. The validity and reliability of the HDSS have been proven and the use of this scale is recommended by the Canadian Hyperhidrosis Advisory Committee (15).
The inclusion criteria were at least 3 BTA injections of Dysport® (abobotulinumtoxinA) at a dose of 150 sU per axilla. The exclusion criteria were beginning the use of, or only the use of, another molecule of BTA, or the use of a non-standardized dose (> 200 sU per axilla). The contraindications were pregnancy or myasthenia gravis. The data collected consisted of age, sex, the DE of the first (FIDE) and last (LIDE) injections, number of injections received, and adjusted and non-adjusted durations of follow-up. The DE was divided into 5 categories: increase ≥ 50%, increase ≤ 50%, constant DE, decrease ≤ 50%, and decrease ≥ 50%. The non-adjusted duration of follow-up corresponded to the time between the day of the first and last BTA injections with a standardized dose of 150 sU per axilla. The adjusted duration of follow-up corresponded to the non-adjusted duration plus the DE of the last received BTA injection. Thus, the last reported DE or the duration between the day of the last injection and the day of data collection were not surpassed. Follow-up periods that included changes in treatment (an increase to a dose ≥150 sU per axilla or change of molecule) were excluded from the analysis. The non-parametric Wilcoxon test for paired samples was used to compare the DE of the first and last injections. Statistical analyses were conducted using SPSS software.
For a sample > 30 patients, a normal distribution is generally a good approximation of the actual distribution. However, the current study examined durations, for which the distribution is often asymmetrical. A Shapiro–Wilk standardization test was performed to observe the distribution of values in the current study. The hypothesis that the sample came from a normally distributed population was rejected according to the Shapiro–Wilk normality test (< 0.001), with a significance level of 5%. The distribution of the sample followed a non-normal law. The non-parametric median-based matched Wilcoxon matched test with a significance threshold of 5% was used to compare the FIDE and LIDE.
A total of 220 patients were treated for PAH from May 2001 to April 2018, of whom 97 (43.4%) were excluded: 84 received fewer than 3 BTA injections with Dysport®, 8 were treated with Botox® (onabotulinum toxin A), and 5 received a non-standardized dose of Dysport® (> 150 sU per axilla) (Fig. 1). Therefore 123 patients were included. Data for 6 patients were missing; thus a total of 117 patients were analysed (79 women and 38 men; mean age 38.3 years, age range 17–79 years). A total of 101 patients received the same dose of Dysport® until the end of the follow-up. Sixteen patients received the standardized dose of BTA before an increase in the dose and 6 received the standardized dose of BTA before a switch of molecule. For these 22 patients, only the follow-up period with a standardized dose of BTA (150 sU per axilla) was analysed: the follow-up periods with changes of dose or molecule were thus excluded from the analysis.
Fig. 1. Study flowchart.
Patients received a mean of 5.5 BTA injections, with extrema from 3 to 24 and a median of 4. The mean FIDE was 5.9 months and the median 6 months. The minimum was 3 weeks and the maximum 30 months. The mean LIDE was 10.2 months and the median 8 months. The minimum was 3 weeks and the maximum 66 months. The difference between the FIDE and LIDE was statistically significant (p < 0.001).
At the end of the follow-up, 56 patients (48%) reported an increase in DE of ≥ 50%, 16 patients (14%) an increase in DE of ≤ 50%, and 21 patients (18%) a stable DE. Eighteen patients (15%) reported a decrease in DE of ≤ 50% and only 6 (5%) reported a decrease in DE of ≥ 50% (Fig. 2).
Among these 6 patients, the largest reported change was a decrease from 18 months of efficacy to 9 months after 10 injections. A single patient received the first 2 injections within 4 months of each other. None received a booster dose after the first injection. The mean number of injections per patient for this group was 6.8 vs. 5.5 for the entire group.
Fig. 2. Change in duration of efficacy of botulinum toxin A treatment at the end of follow-up.
Long-term follow-up
The mean non-adjusted duration of follow-up was 4.8 years. The mean adjusted duration of follow-up was 5.5 years, with a minimum of 9 months and a maximum of 15 years and 3 months. Fifty patients (44%) were followed for more than 5 years, of whom 20 (17%) were followed for more than 10 years.
Among the 20 patients with a follow-up of more than 10 years, the mean number of injections received was 8.25 per patient. Eighteen of these patients reported an increase in DE of > 50%. Only one patient reported a decrease in DE of > 50% between the first and last injections. None had a decrease in DE of < 50%.
Cumulative dose
The mean cumulative received dose was 823 U/armpit; the minimum was 450 U/armpit and the maximum 3,600 U/armpit. The received cumulative dose of the patients with an increase in the DE was 871 U/armpit. The received cumulative dose of the patients with a decrease in the DE was 838 U/armpit.
This study showed a significant increase in the DE of BTA injections during a retrospective follow-up of 117 patients with severe PAH, treated at the Le Mans Medical Center, between May 2001 and April 2018. The current study confirms the results from our first study (10) and reaffirms the efficacy of Dysport® BTA treatment for PAH. It also highlights the absence of adverse effects with the increase in cumulative dose and the absence of a secondary diminution of efficacy.
The major strength of the current study was its duration, as it reports the longest follow-up of treatment with BTA injections. Indeed, our data collection extended over 17 years, from 2001 to 2018, with a maximum duration of monitoring of 15 years and 3 months. The mean follow-up in our study was 5.5 years vs.2.73 years in our previous study, with a duration of data collection of 11 years (10). Another study in Australia lasted 10 years (9). The duration of our study allowed us to confirm the effectiveness of this treatment over a very long period. Indeed, 80% of patients reported a stable or increasing DE at the end of follow-up. No side-effects were reported during the entire follow-up.
Any variations in treatment were excluded, creating a condition of maximal bias. The analysis was thus freed from any residual effect of an increase in dose or change in molecule. The analysis was performed in paired groups. The study also excluded patients who received fewer than 3 BTA injections, in order to gain sufficient perspective on the actual effectiveness of the treatment. The current study retained a large number of patients, despite the restriction of therapeutic variation. In addition, most of the patients in the study cohort (82%) had no change in treatment.
This study is in agreement with the published data. The DE varies depending on the study, ranging from 2 to 24 months (1, 16, 17). In one study, the relationship between the dose of toxin injected and the DE was analysed: among 47 patients followed for axillary hyperhidrosis for 29 months, Wollina et al. (18) demonstrated a longer DE with a higher dose of botulinum toxin (200 U Botox® per armpit), but the comparison was made with data from the literature and not with that of a matched group.
Five percent of patients in the current study reported a large decrease in their DE. It has been suggested that such a decrease may be due to the formation of anti-botulinum toxin antibodies (19). The repetition of BTA injections did not appear to influence the decrease in the DE observed in some patients. Indeed, the values for the cumulative dose were similar between patients who showed an increase in DE and those who showed a decrease. Thus, the cumulative dose is not as relevant to the study as the number of injections received, which inevitably correlates with the cumulative dose.
A tendency towards an increase or decrease in DE was clearly visible from the first injections. This trend thus appears early, although the cumulative dose was very low. No patients with an increase in DE reported a secondary decrease.
The short interval between 2 injections did not appear to influence the DE among the patients who reported a marked decrease. Indeed, only one of the 6 concerned patients received 2 injections within the space of 3 months.
No patient showed complete disappearance of the effects of BTA. All continued to respond to treatment, with a DE of at least one month. Although we did not search for the presence of anti-botulinum toxin antibodies, the preservation of at least a short DE does not favour their development in these patients.
The main limitation of the current study was its retrospective nature and thus the memory bias inherent in this type of study. This bias was partially mitigated by the disabling nature of PAH, prompting the patient to consult after the recurrence of symptoms.
Future studies could focus on patients with a decrease in DE, in order to identify the risk factors for the type of this evolution or the differences between responder and non-responder patients.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize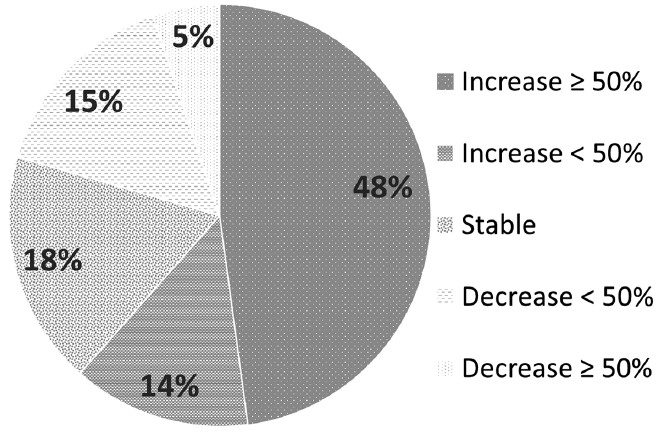 Click to show fullsize
Click to show fullsize