


Department of Dermatology, Toho University Sakura Medical Center, 564-1 Shimosizu, Sakura, Chiba 285-8741, Japan. E-mail: fumihito.abe@med.toho-u.ac.jp
Accepted Sep 25, 2019; E-published Sep 25, 2019
Various skin manifestations, such as psoriasiform eruption, palmoplantar pustulosis, and lupus-like syndrome, have been reported to be induced by tumour necrosis factor alpha (TNF-α) inhibitors (1). Recently, skin manifestations associated with administration of interleukin (IL)-17 inhibitors have also been reported (2). We report here our experience with a patient with psoriatic arthritis who developed atopic dermatitis-like eruptions caused by the separate administration of 2 types of biologics, infliximab and ixekizumab.
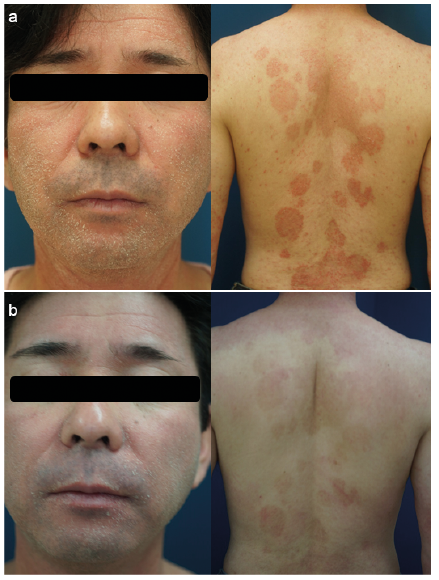
The patient was a 46-year-old man with no history of atopic dermatitis. At approximately 30 years of age, he developed plaque psoriasis and received outpatient treatment at a neighbourhood dermatology clinic. His skin manifestations were stabilized by topical application of betamethasone butyrate propionate ointment and maxacalcitol ointment. One month before his visit to our department, he experienced severe pain in his wrist and finger joints, causing difficulty writing. He was thus referred to our department. He was diagnosed with psoriatic arthritis, and administration of infliximab was initiated. Several days after the initial administration of infliximab, amelioration of arthralgia and erythema was observed. One week later, he developed generalized erythema and papules on the trunk and extremities (Fig. 1). Erythema with scales was observed on his entire face, and he reported severe pruritus. Skin biopsy from a newly developed erythema on the forearm revealed epidermal spongiosis and lymphocyte perivascular infiltration in the upper dermis (Fig. 2). As pruritus and eczematous eruptions persisted, infliximab was discontinued, followed by gradual resolution of eruptions. However, as the joint symptoms relapsed, ixekizumab was introduced. One week after the introduction of ixekizumab, the eczematous eruptions relapsed, as was observed after treatment with infliximab. His eosinophil count, which was initially within the normal range, increased (830/µl; pretreatment level, 126/µl). Serum IgE (560 IU/l; normal < 250 IU/l) and thymus and activation-regulated chemokine (980 pg/ml; normal < 449 pg/ml) levels were also high. As the joint symptoms were relieved, administration of ixekizumab was continued, whereas atopic dermatitis-like eruptions were treated with topical application of steroids and moisturizers, after which they were gradually relieved. Fourteen months after initiation of administration of ixekizumab, the eruptions on the patient’s extremities resolved. However, residual ery-thema with desquamation was still observed on his face.
Fig. 1. Clinical pictures. (a) Erythema with scales on the face and back at the time of administration of infliximab. (b) Erythema with scales on the face and back at the time of administration of ixekizumab. Permission from the patient is given to publish these photos.
Fig. 2. The epidermis appears spongiform, and lymphocytic infiltration to the superficial layer of the dermis is observed (hematoxylin-eosin, original magnification × 200).
It has been reported that of 92 patients with Crohn’s disease or rheumatoid arthritis who were treated with infliximab, 19 developed atopic dermatitis-like eruptions. Of these 19 patients, 16 had atopic predisposition (3). In patients with rheumatoid arthritis treated with other TNF-α inhibitors (i.e. adalimumab and etanercept), eczema different from psoriasiform eruptions has also been reported (4). There is also a report of atopic dermatitis-like eruptions in patients treated with infliximab for psoriasis (5). Furthermore, recent reports have indicated cases in which atopic dermatitis-like eruptions occurred in patients treated with biologic agents other than TNF-α inhibitors. There are 2 reported cases in which patients with psoriasis developed atopic dermatitis-like eruptions after administration of ustekinumab. One of the patients had a history of atopic dermatitis, and both had high levels of IgE (6). In the patient with a history of atopic dermatitis during early childhood, psoriatic eruptions were relieved by administration of ustekinumab; however, his atopic dermatitis relapsed and worsened (7). Atopic dermatitis-like eruptions have been reported to be caused by various biologics used for the treatment of psoriasis.
In our case, 2 types of biologics caused atopic dermatitis-like eruptions. This finding suggests that atopic dermatitis-like eruptions are not a skin disorder specific to a drug, but might occur in patients with psoriasis treated with any biologic agent. It has conventionally been considered that psoriasis is a T helper (Th)-1 dominant disease, and that atopic dermatitis is a Th2-dominant disease. The coexistence of psoriasis and atopic dermatitis is rare. A possible reason for the development of atopic dermatitis-like eruptions is that administration of biologics, such as TNF-α inhibitors, induces transition from Th1 to Th2 dominance.
In contrast to that in psoriasis, expression of IL-17 has been reported to be decreased in atopic dermatitis (8). Inhibition of IL-17 impairs the skin barrier function. Moreover, colonization of Staphylococcus aureus or fungi is also expected to increase because of decreased production of antimicrobial peptides by keratinocytes. Thus, inhibition of IL-17 per se may also induce atopic dermatitis-like eruptions.
In our case, the serum IgE levels of the patient were high, despite the absence of a past or family history of atopic dermatitis. In patients with psoriasis who exhibit a past history of atopic dermatitis or high levels of IgE, attention should be paid to the possibility that administration of biologic agents may cause eczematous eruptions. Furthermore, there have been 3 reported cases of psoriasis in which IL-17 inhibitors (i.e. ixekizumab, brodalumab, and secukinumab) caused dry, pruritic erythema on the face (2). In our patient, systemic eczematous eruptions, which occurred after administration of ixekizumab, have also been relieved by topical application of steroids and moisturizers to date, but dry erythema has persisted only on the face. Thus, it is likely that IL-17 inhibitors can cause eczematous eruptions on the face.


 Click to show fullsize
Click to show fullsize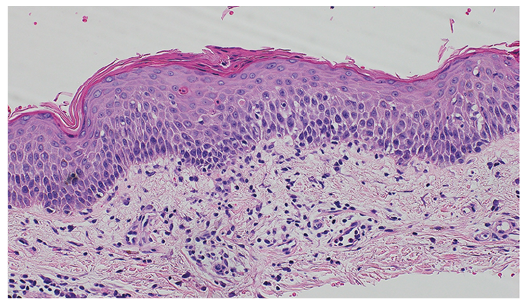 Click to show fullsize
Click to show fullsize