


1Department of Dermatology, Addenbrooke’s Hospital, Hills Road, Cambridge, Cambridgeshire, 2Department of Plastic Surgery, Lister Hospital, Coreys Mill Lane, Stevenage, Hertfordshire, UK, and 3Department of Otorhinolaryngology and Head & Neck Surgery, Bielefeld University Hospital, Bielefeld, Germany
#Co-senior author.
Basal cell carcinomas are the commonest solid malignancy in humans and thought to grow faster in the periocular region. We measured growth rates between periocular and non-periocular nodular basal cell carci-nomas in the head and neck region from high-resolution digital photos and operative notes. The non-periocular basal cell carcinomas (head and neck) showed a mean tumour volume doubling time of 129.8 ± 21.74 (n = 79) days, and the periocular basal cell carcinoma a mean of 177.5 ± 37.21 (n = 47) days. The unpaired t-test with Welch correction showed that this difference was not significant (p = 0.2719). The mean tumour volume doubling time was 147.59 ± 37.75 days for head and neck basal cell carcinomas overall. For the first time, tumour volume doubling times for nodular basal cell carcinomas in the periocular versus non-periocular regions for the head and neck area were analysed, with no significant differences demonstrated. Further, comparison of basal cell carcinoma growth rates with other common solid tumours confirmed that basal cell carcinomas are slow growing malignancies.
Key words: periocular; non-periocular head and neck basal cell carcinoma; BCCs; tumour volume doubling time; growth rates.
Accepted Sep 25, 2019; E-published Sep 25, 2019
Acta Derm Venereol
Corr: Dr Peter Goon, Department of Dermatology, Addenbrooke’s Hospital, Hills Road, Cambridge CB2 2QQ, Cambridgeshire, UK. E-mail: peter.goon@nhs.net
Basal cell carcinomas are very common skin tumours which are locally destructive. It was thought that basal cell carcinomas around the eyes grow faster than those elsewhere based on one previous paper. We demonstrate that there is no evidence for this and also calculate tumour growth rates to show the position of basal cell carcinomas in a growth rate figure, compared to more malignant tumours. Our new data can guide clinicians as to how much time there is avail-able for removal or treatment before crucial parts of our anatomy could be affected.
Basal cell carcinomas (BCCs) are the most common malignant tumour in humans, especially among fair skinned humans in the developed world (1–4). Indeed the prevalence rate of BCCs far surpasses all other malignancies (1–3) but since mortality from BCCs is very rare, it has long been considered more of an inconvenient nuisance, and most countries do not include them in their cancer registries.
Despite the rapidly increasing incidence rates being reported and the increasing burden on healthcare systems, BCCs have not been extensively researched and the amassed knowledge about the natural history of this common tumour is patchy at best.
In this study, we have tested the hypotheses that there are no significant differences between the growth rates of periocular nodular BCCs compared to other head and neck BCCs, and also derived tumour volume doubling times (TVDT) for comparison with those of other malignancies. Only BCCs of the nodular histological subtype were selected as it is likely that other subtypes such as the morphoeic, infiltrative or micronodular subtypes would not be visually well represented on the skin surface for measurement, plus these other subtypes of BCC may grow in a more diffuse or tendril-like pattern rather than a generally spherical pattern. Whether these other types of BCC are biologically distinct or have different growth rates is not known. BCCs have long been classified among the slower growing solid tumours of the skin (non-melanoma skin cancers) in contrast to the highly malignant skin tumours such as melanoma or Merkel cell carcinoma.
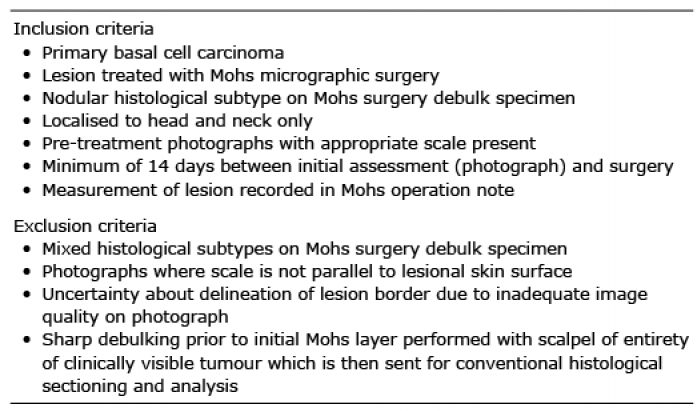
A retrospective cohort study to study growth rates in BCCs in the periocular region (upper and lower eyelids, within the nasojugal fold, medial/lateral canthi) and non-periocular BCCs (defined as all other regions of the head and neck). The patient cohort was defined as those individuals who underwent Mohs micrographic surgery (MMS) between 1st January 2016 and 31st January 2018. Inclusion/exclusion criteria are detailed in Table I.
Table I. Inclusion and exclusion criteria
Nodular BCCs selected for the study, using the above criteria, allows narrowing and focus of the study on clinically very similar lesions. This is to decrease the expected biological variation found amongst different types of BCCs, and consequently their growth rates as well.
The patient details were retrieved from our hospital electronic patient record system and clinical image record. We were able to utilise the unique search parameters of the electronic database and hospital administration system to find patients with BCCs from 2016 onwards.
Photographs of lesions were captured by the hospital clinical photography department following standardised local protocols (5) with a Nikon D800 full frame DSLR (Digital Single Lens Reflex) camera with a 105 mm macro lens with a fixed focal length. Lesions were photographed perpendicular to the skin surface at a 1:1 reproduction ratio with a F-stop of 25. This gives a depth of field of approximately 1 mm. Digital scales included in images were constructed in Adobe Photoshop by photographing a ruler at the same reproduction ratio. These are used instead of physical rulers as our experience suggests that these are equal if not superior to physical rulers (6) particularly in difficult to reach anatomic locations and hair bearing areas.
Final lesion sizes were obtained from the Mohs operation notes. Initial lesion sizes were measured on digital photographs taken at the outpatient clinic assessment of the patients by a single observer (AK) using the digital scale included with the image. Lesions were measured across their largest single dimension, d. Tumours were assumed to be spherical and their volume was calculated according to the following formula: (Fig. 1).
Fig. 1. Gompertzian Tumour Growth Curve.
Growth rates of solid tumours can be easily estimated along the linear section of the Gompertzian growth curve (7–10). Visible and detectable tumours usually contain between 106 to 109 cells. Multiple examples of different solid tumours have demonstrated linearity of growth on a logarithmic scale during the early detectable phase (11–14).
Doubling times can be calculated from 2 observed time points, simply using the following equations:
A selection of histological specimens were examined and the diameter of individual BCC cells was measured a micrometer. Assuming these cells are spherical, an estimated volume of a BCC cell and the number of cells for a tumour of a given diameter can be derived from the following equations:
A further equation can then be used to estimate the age of the tumour assuming a single precursor cell.
Table II shows the patient demographics and lesion characteristics. Continuous variables are expressed as mean ± standard deviation (SD). Table III shows actual sites of lesions. Fig. 2 shows the doubling times for both periocular and non-periocular head and neck BCCs.
Table II. Patient demographics and lesion characteristics
Table III. Actual sites of lesions
Fig. 2. Tumour volume doubling times for nodular basal cell carcinomas (periocular (PO) vs head & neck (HN) (non-periocular).
However, total overall mean doubling time can be assumed to be accurately reflect the true overall mean, which is 147.59 days (SEM ± 19.47). The SD is 218.6 days for the total cohort of head and neck (periocular and non-periocular) BCCs.
Fig. 3 shows the estimated position of BCC growth rates in comparison to other solid tumours. Data extracted for analyses from Friberg & Mattson 1997 (12).
The measured diameters of BCC cells histologically range from 2.5 to 10 microns. Assuming the minimum diameter of a clinically detectable tumour is 1 mm, this gives us a detection threshold of approximately 1 to 60 (× 106) cells and an estimated tumour age of approximately 8–11 years. [These calculations are based on cellular size and volume only].
Fig. 3. Growth rates (estimated) for different solid tumours in comparison to nodular basal cell carcinomas (BCCs).
Table IV shows the number of cells in a tumour of a given diameter and the estimated tumour age ranges for tumour cells sized between 2.5–10 microns.
There are significant overlaps between the ranges seen above and this illustrates the wide individual variation seen in BCCs in terms of size of cells, and does not allow for necrosis within tumour bodies, non-basal cellular components, connective tissue, etc.
Our data confirm that BCC growth rates can be considered slow growing compared to other malignant solid tumours. The fact that BCC are essentially non-metastasising solid tumours is almost undoubtedly the reason for the negligible mortality associated with this tumour as it means that the tumour can be removed en bloc or destroyed in the vast majority of cases without damage to vital internal organs that would threaten life.
Table IV. Number of cells in a tumour of a given diameter and the estimated tumour age ranges for tumour cells sized between 2.5–10 microns
TVDT have implications for patients ranging from specific life-affecting (screening programmes, prognosis, estimation of lifespan, etc.) to the legal and mundane (actuarial/risk estimations by insurance companies, court cases estimating when the primary or metastatic tumours arose, etc.).
BCCs have long had the reputation of being a slow growing and indolent tumour in humans, despite being the most frequent malignancy by far (1, 2). This is due to the fact that directly attributable mortality to BCCs is extremely rare, and most developed countries do not even include this tumor in their cancer registries.
In contrast, BCCs incidence rates are rising rapidly, in conjunction with other non-melanoma skin cancer (NMSC) such as squamous cell carcinomas, Merkel cell carcinoma and eccrine porocarcinoma (1, 15–17). The cost and burden to the UK taxpayer is also rising rapidly and NMSC costs have been estimated to reach almost half a billion pounds in 2025 for the NHS (1).
Tan et al. (18) published observational data that suggested that periocular BCCs could grow rapidly, especially recurrent tumours, larger tumours and tumours in men. There was no direct comparison of growth rates between periocular and non-periocular tumours or other control groups. In this study, we wanted to examine whether there was evidence that BCCs actually grew at different rates based on their anatomical site of origin on the skin, calculate proper TVDTs to allow comparison with other tumours, and to estimate the BCC position in the hierarchy of human cancer growth rates for the first time.
We show that BCCs from periocular sites do not demonstrate faster growth rates than other non-periocular head and neck BCCs, indeed the converse may be true as the data trend is for a faster growth rate seen for the non-periocular tumours (non-significant). However, the sample size of 126 samples is not large and does not give sufficient analytical power for small differences. For the first time, we are able to estimate the TVDT for BCCs and give an approximation of the tumour’s growth rate compared to other published data. We show that the mean TVDT for head and neck BCCs is approximately 150 days. There are no data for BCCs from non-periocular head and neck sites, therefore we cannot comment on whether those tumours grow faster or slower than the periocular head and neck ones. The wide SD from the sample seen above (218.6 days) demonstrates the wide biological variation in growth rates and even regression seen in some of these tumours in this cohort. This is consistent with the observed clinical characteristics for these BCCs, with some regressing or disappearing after punch biopsies, etc, and this phenomenon has been reported before (18).
BCCs do seem to grow slower than more malignant tumours, such as primary breast or colorectal tumours, but the insignificant mortality rate can almost certainly be attributed to their unique biological characteristic of not metastasising to distant sites. In spite of this, neglected BCCs can cause significant morbidity if present on functionally and cosmetically sensitive areas (T-zone of face) on or adjacent to structures such as the eyes and nose. A gradual, relentless tumour expansion leads to local invasion and destruction of these structures leading to disfigurement, blindness and loss of function. These locally advanced tumours are often impossible to resect completely as the deep margins are frequently involved and the resulting defect would lead to even worse morbidity. Early resection of BCCs in these areas, preferably with Mohs surgery, is therefore important. Recent developments in medical treatment such as the hedgehog signalling pathway inhibitors (vismodegib and sonidegib) (19) have offered new hope for reducing BCC tissue mass in the long-term (not available in the UK on the NHS, but available in other countries), or prior to salvage surgery.
We would like to thank our colleagues in the Department of Dermatology, especially our Mohs surgeons; also our colleagues Mark Bartley (Medical Photography), George Meligonis (Consultant Histopathologist) and our patients for their input into this study.
The authors have no conflict of interest to declare.


 Click to show fullsize
Click to show fullsize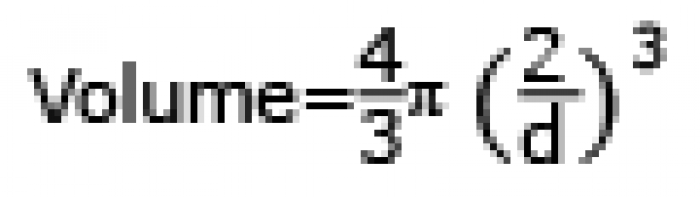 Click to show fullsize
Click to show fullsize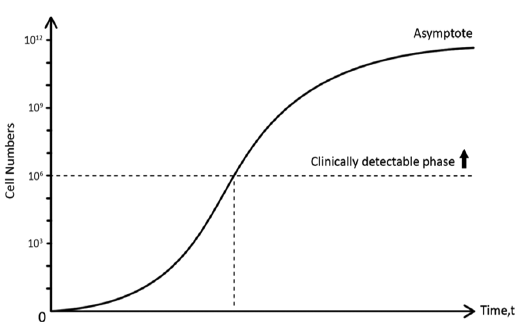 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize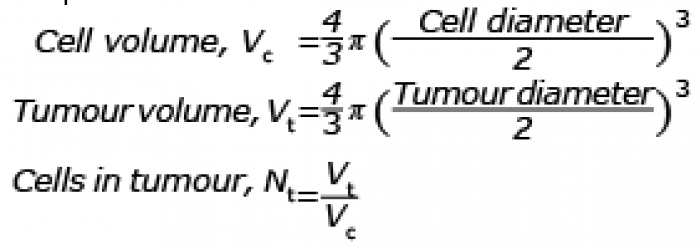 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize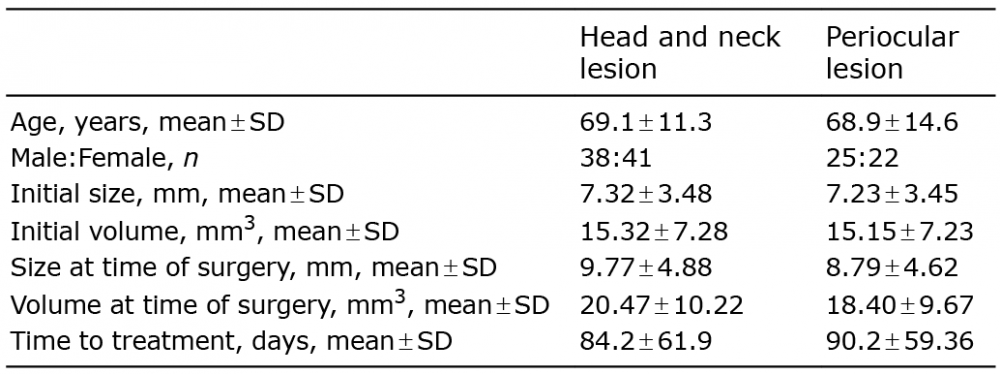 Click to show fullsize
Click to show fullsize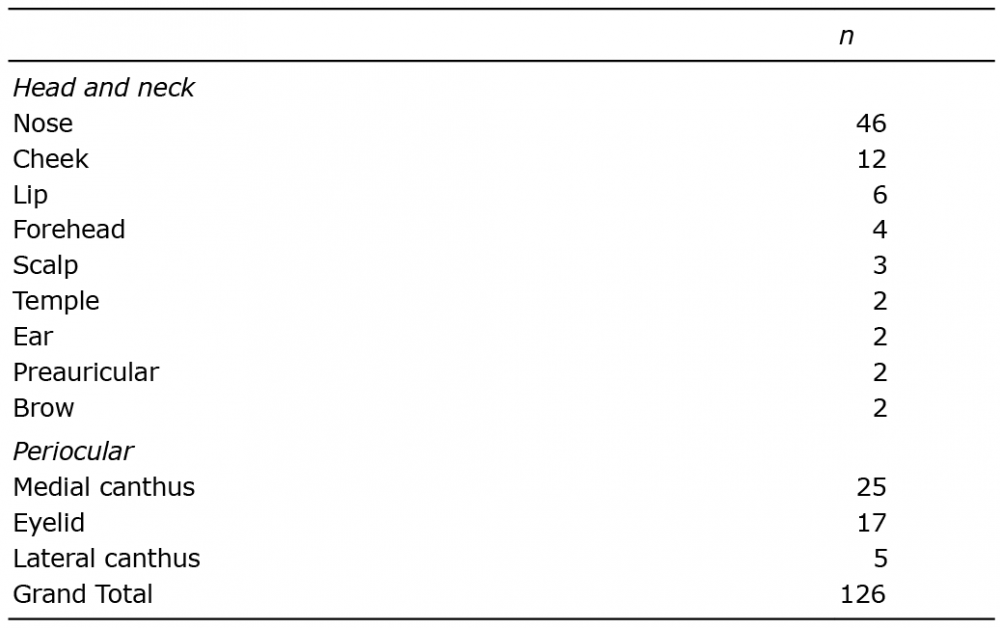 Click to show fullsize
Click to show fullsize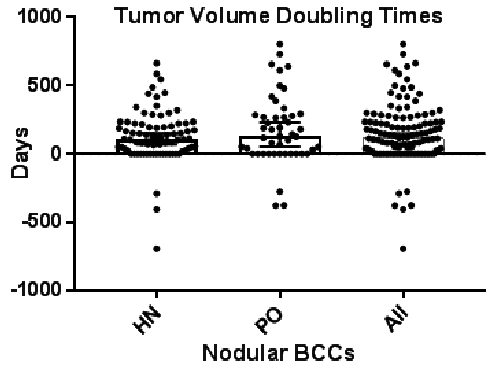 Click to show fullsize
Click to show fullsize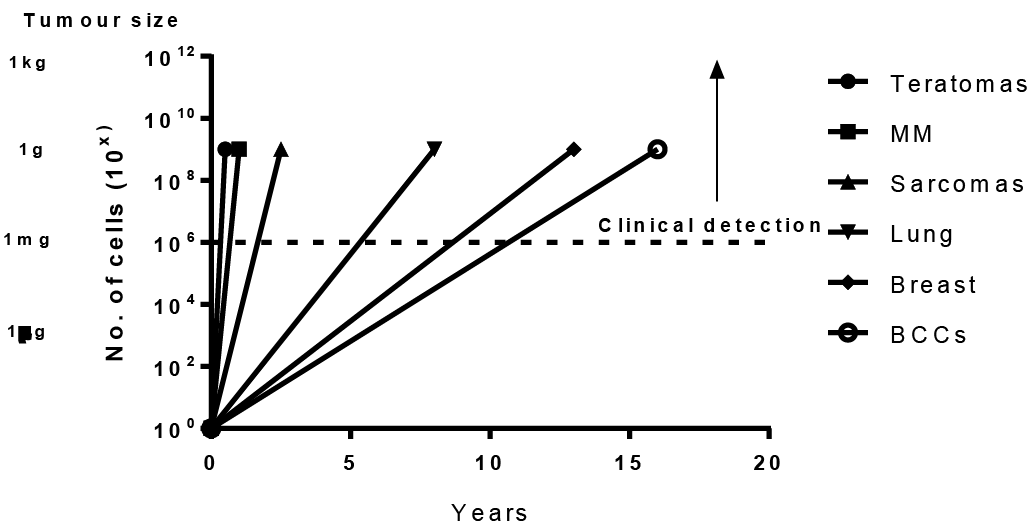 Click to show fullsize
Click to show fullsize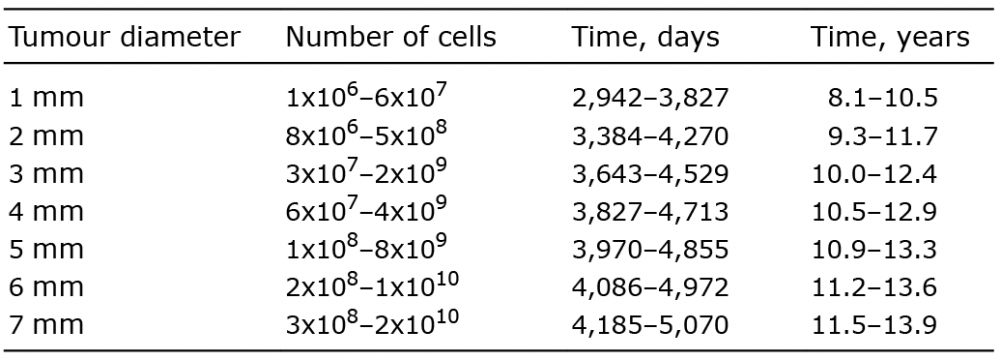 Click to show fullsize
Click to show fullsize