


1Department of Dermatology and Allergy, Herlev and Gentofte Hospital, University of Copenhagen, Hellerup, 2Copenhagen Research Group for Inflammatory Skin, Herlev and Gentofte Hospital, Hellerup, Departments of Dermatology, 3Aarhus University Hospital, Aarhus, 4Zealand University Hospital, Roskilde and 5Bispebjerg Hospital, Copenhagen, and 6Dermatology Clinic, Nykoebing Falster, Denmark
The initiation and evaluation of treatment with biologics for psoriasis is based on the Psoriasis Area Severity Index (PASI) and/or Dermatological Life Quality Index (DLQI). However, these indices do not always correlate well, and changes in the DLQI do not always follow changes in the PASI. Based on data from the Danish national registry (DERMBIO), this study investigated the correlation between changes in PASI and DLQI in a cohort of patients with moderate-to-severe psoriasis treated with biologics or apremilast using Spearman’s rank correlation analyses. The correlation analysis of 1,677 patients, of whom 276 had available data after 5 years, showed weak-to-moderate correlation between PASI and DLQI during a 5-year period and between changes in PASI and DLQI: 0.58 (p < 0.0001) for baseline to 3 months and 0.42 (p < 0.0001) for 3 to 12 months. The first question on “Symptoms and feelings” made up the largest proportion of the overall DLQI. The correlation between PASI and DLQI is weak-to-moderate and varies over time. Changes in PASI correlate weak-to-moderately with changes in DLQI during the first 12 months of treatment, with symptoms being the most important factor contributing to impaired quality of life.
Key words: psoriasis; patient-reported outcomes; Psoriasis Area and Severity Index; Dermatology Life Quality Index; biologics.
Accepted Oct 3, 2019; E-published Oct 3, 2019
Acta Derm Venereol 2019; XX: XX–XX.
Corr: Nikolai Dyrberg Loft, Department of Dermatology and Allergy, Herlev and Gentofte Hospital, University of Copenhagen, Hellerup, Denmark. E-mail: nikolai.dyrberg.loft@regionh.dk
The Danish clinical database DERMBIO collects routine information during the treatment of psoriasis with biologics or small molecules. These include physicians’ evalua-tion of severity, with the Psoriasis Area Severity Index, and the influence on patients’ lives, with the Dermatology Life Quality Index. Among 1,677 patients the correlation between Psoriasis Area Severity Index and Dermatology Life Quality Index was weak-to-moderate during a 5-year treatment period. The changes in Psoriasis Area Severity Index correlated weak-to-moderately with changes in Dermatology Life Quality Index during the first 12 months of treatment, with the strongest correlation seen during the first 3 months. Symptoms were the most important factor in the Dermatology Life Quality Index. Measuring and monitoring of patients’ symptoms are important, and additional measures to capture symptoms might be beneficial in daily practice.
Psoriasis is a common chronic immune-mediated inflammatory skin disease, which confers an increased psychosocial burden (1) and impaired quality of life (2), often in a disease-severity dependent manner (3). Short-term assessment of treatment efficacy is mostly based on physician evaluation, whereby a 75% reduction in the Psoriasis Area and Severity Index (PASI75) remains the current treatment goal in most guidelines for patients with moderate-to-severe psoriasis (4–7). How-ever, some patients are not satisfied with this reduction, and a 90% improvement (PASI90) has been suggested as a clinically important endpoint, and a treatment goal (8–10). Indeed, patients achieving PASI90 report lower Dermatology Life Quality Index (DLQI) than patients achieving PASI75–89 (11) and patients with clear skin based on Physicians Global Assessment (PGA) report lower DLQI compared with those with almost clear skin (12). However, in smaller studies, changes in PASI during the first 3 months of treatment do not correlate fully with changes in DLQI (13, 14) and reported correlations between PASI and DLQI range from negligible (13, 15) to strong (16, 17). This apparent dissociation between PASI and DLQI is not yet fully elucidated, but pruritus has been shown to affect this relationship (18). We therefore investigated the relationship between changes in PASI and DLQI in a nationwide cohort of all Danish patients with psoriasis treated with biologics or novel small molecule therapies.
Data sources
The study was approved by the Danish Data Protection Agency (ref. HGH-2016-048, I-Suite: 04520). In Denmark, approval of an ethics committee is not required for register studies. The study was carried out in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) recommendations (19).
The DERMBIO registry (20–28) is a Danish nationwide registry wherein all treatment series with biologics, biosimilars, and novel small-molecule agents for psoriasis are registered. Registration and prospective data collection in DERMBIO have been mandatory since 2007. Data are reported from all academic hospital centres (85% of all treatments) with an estimated coverage of 100% of the treatment series and a small proportion of patients are seen in clinical practices, with an estimated coverage of 88% of treatment series (27). To maximize data integrity only patients treated in hospital clinics were included (28).
Patient selection
Patients treated for at least 30 days with available data on PASI and DLQI at baseline and at a minimum of one subsequent visit were included. The patients were only included the first time they met the inclusion criteria, i.e. at the time of their first treatment in DERMBIO.
Statistical analysis
For continuous data, means with standard deviations (SD) and medians with range were reported, and for categorical outcomes numbers with percentages were presented. The correlation between changes in PASI and DLQI were assessed for the periods: baseline to 3 months, 3 to 12 months, and baseline to 12 months. The correlations were evaluated based on absolute changes in PASI and DLQI relative changes in both PASI and DLQI, and for relative change in PASI and absolute change in DLQI, as all outcomes have been used in prior studies (13, 14, 29). We then investigated the correlation between changes in PASI and changes in the newly proposed DLQI-R (30). Correlation analyses were performed between PASI and DLQI at baseline, after 3, 6 and 12 months of treatment, and then for each subsequent year until 5 years of treatment. In addition, correlation analyses were performed between PASI and DLQI-R at the same time-points (30). Patients were stratified based on PASI (PASI < 5 and PASI ≥ 5; PASI < 10 and PASI ≥ 10) to assess the importance of different disease severities on impact on quality of life. Patient-reported outcomes were assessed for different response categories: PASI < 50, PASI50–< 75, PASI75–< 90, PASI90–< 100, and PASI100. For patients for whom the single questions in the DLQI were available, descriptive analysis for the percentage each question contributed to the overall DLQI, the correlation between PASI and each question, and correlation between changes in PASI and the single questions were assessed. Correlation coefficients were assessed using Spearman’s rank correlation (rs). Correlation coefficients are considered negligible if rs = 0.0–< 0.30, weak if rs = 0.30–<0.50, moderate if rs = 0.50–< 0.70, strong if rs = 0.70–<0.90, and very strong if rs = 0.90–1.00 (31). Fischer’s z transformation was used to compute 95% confidence intervals (CI) and z scores were used to test for statistical differences. Wilcoxon rank-sum test was used for comparison of continuous data. All analyses were performed using SAS software version 9.4 (SAS Institute Inc., Cary, NC, USA).
Dermatology Life Quality Index
The DLQI consists of 10 individual questions, which are scored from 0 to 3, resulting in a total score of 0–30 (32). In question 3–10 it is possible to answer the question “Not relevant”, which is then scored 0. The DLQI can be divided into 6 domains, which each consist of 1 or 2 questions (32).
Psoriasis Area and Severity Index
In PASI, the body is divided in 4 regions, which are evaluated on erythema, induration, and scaling multiplied by the area affected of the body part, resulting in a total score of 0–72 (33).
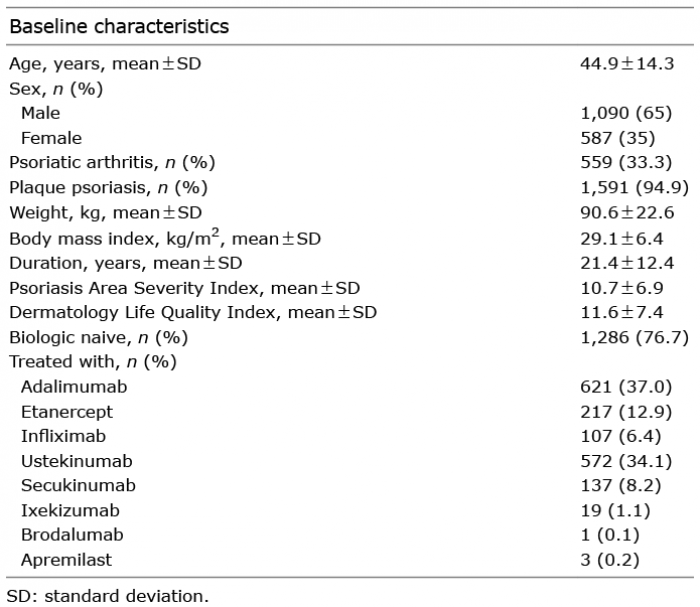
The study population consisted of 1,677 unique patients, with a strong predominance of male patients (65%) and bio-naïve patients (76.7%, Table I). After 3 months of treatment 1,308 patients had available data, 1,090 after 6 months, 1,069 after 12 months, 744 after 24 months, 553 after 36 months, 382 after 48 months, and 276 after 5 years of treatment.
Table I. Baseline characteristics of included patients (n = 1,677)
Correlation between changes in disease severity and changes in quality of life over time
Correlation analysis between changes in PASI and DLQI during the first year of treatment yielded Spearman’s rhos in the range 0.34–0.58 (Table II). The highest correlation was observed for relative changes in PASI and DLQI from baseline to 3 months. Significantly stronger correlations were seen for the period: baseline to 3 months compared with 3–12 months (p = 0.0001). There were no differences between the correlation coefficients obtained with DLQI-R (data available on request). Patients were stratified on their biological exposure, where patients with a previous biological treatment showed significantly higher correlation coefficients for all periods for absolute changes in both PASI and DLQI (Table SI). For the biologic-exposed patients, those with 2 or more prior treatments showed significantly higher correlation coefficients for baseline to 3 months in absolute changes in both PASI and DLQI than those with only one prior treatment (Table SII). No differences were seen for patients with psoriatic arthritis compared with those without psoriatic arthritis (data available on request). Likewise, no difference was seen when patients with other forms of psoriasis were excluded (data available on request).
Table II. Spearman’s rho (rs) for changes in Psoriasis Area Severity Index (PASI) and Dermatology Life Quality Index (DLQI) after treatment with biologics
Correlation between disease severity and quality of life
A weak correlation was observed at baseline (rs = 0.33), and after 3 and 6 months of treatment the correlation between PASI and DLQI was moderate (Fig. 1). At the subsequent time-points a decrease in correlation between PASI and DLQI was observed, and after 5 years of treatment, based on 276 observations, the correlation between PASI and DLQI was similar to that observed at baseline (rs = 0.35). The same correlations were seen for DLQI-R (data available on request).
Fig. 1. Correlation between Psoriasis Area Severity Index (PASI) and Dermatology Life Quality Index (DLQI) during treatment with biologics or apremilast assessed at baseline (month 0, number of patients with available data, n = 1,677), month 3 (n = 1,308), month 6 (n = 1,090), month 12 (n = 1,069), month 24 (n = 744), month 36 (n = 553), month 48 (n = 382), and month 60 (n = 276). Correlation coefficients (rs) were assessed using Spearman’s rho, and confidence intervals (CI) were computed with Fisher’s z transformation.
In 11,450 visits a PASI < 5 was reported and in 2,586 visits a PASI ≥ 5; no difference between correlation coefficients was observed between these 2 groups (PASI < 5, rs = 0,41; PASI ≥ 5, rs = 0.38). When visits were divided into PASI<10 (n = 12836) vs. PASI ≥ 10 (n = 1,190) a substantial difference in correlations was observed: a negligible correlation (rs = 0.13) between PASI and DLQI for patients with PASI ≥ 10 and a weak-to-moderate correlation (rs = 0.47) for patients with PASI < 10. In addition, a steady increment of mean DLQI with increasing PASI until PASI ≥ 15 was observed; hereafter an increase in disease severity was followed by a small or no increase in impact on quality of life (Fig. 2).
Fig. 2. Mean Dermatology Life Quality Index (DLQI) for patients with a Psoriasis Area Severity Index (PASI) of 0–<5 (n = 11,450), PASI 5–<10 (n = 1,386), PASI10–PASI<15 (n = 730), PASI15–<20 (n = 278), PASI20–<25 (n = 103), PASI25–<30 (n = 44), and PASI≥30 (n = 35).The red dotted line represents the linear increment in DLQI for PASI groups from PASI0–<15. The grey dotted line represents the linear increment in DLQI for PASI groups from PASI≥15.
Stratified based on response criteria
Statistically significant lower DLQIs were observed for patients with a higher delta PASI after 3, 6 and 12 months and statistically significant larger reduction in DLQIs, except for PASI90–< 100 vs. PASI100, where no difference between changes in DLQI was observed (Table III).
Table III. Psoriasis Area Severity Index (PASI) and Dermatology Life Quality Index (DLQI) for patients divided into 5 groups based on response after 3, 6 and 12 months
Distribution and percentage of each question at different time-points
In total, for 1,045 patients the single questions in the DLQI were available at baseline, for 878 they were available after 3 months, for 712 after 6 months, for 699 after 12 months, for 503 after 24 months, for 381 after 36 months, for 252 after 48 months, and 184 patients had available single questions of the DLQI after 5 years of treatment. At baseline the first 2 questions in DLQI concerning the “Symptoms and feelings” domain made up 36% (23% + 13%) of the overall DLQI and the rest of the questions each made up between 5% and 13% of the overall DLQI (Fig. 3). After 5 years of treatment the “Symptoms and feelings” domain made up 69% (58% + 11%) of the overall DLQI (Fig. 3). The distribution of answers to each question showed that 94% of patients reported ≥1 in question 1 at baseline and 60% of the patients did so after 5 years of treatment, and 10–26% of the patients reported ≥1 for the rest of the questions after 5 years (Fig. 4). Approximately 10% of the patients answered “Not relevant” in the questions 6, 7 and 9 (Fig. 4).
Fig. 3. The percentage that each of the individual questions of the Dermatology Life Quality Index (DLQI) contributes to the overall DLQI (a) at baseline (number of patients with available individual question of DLQI, n = 1,045), (b) after 3 months of treatment (n = 878), (c) after 12 months of treatment (n = 699), and (d) after 60 months of treatment (n = 184).
Fig. 4. Distribution of answers for each of the individual questions of the Dermatology Life Quality Index (DLQI) (a) at baseline (number of patients with available individual question of DLQI, n = 1,045), (b) after 3 months of treatment (n = 878), (c) after 12 months of treatment (n = 699), and (d) after 60 months of treatment (n = 184). NR corresponds to the answer “Not relevant”, a score of 0 corresponds to the answer “Not at all” or “Question unanswered”, a score of 1 corresponds to the answer “a little”, a score of 2 corresponds to the answer “a lot”, and a score of 3 corresponds to the answer “very much”.
Correlation between PASI and each question in Dermatology Life Quality Index at different time-points.
The correlation between PASI and each of the individual questions in the DLQI was assessed for the same time-points. The first question on “Symptoms and feelings” was weak-to-moderately correlated with PASI and correlation coefficients above 0.30 were observed at all time-points (Table SIII). Question 4 on “Daily activities” and question 10 on “Treatment” showed weak correlations (rs = 0.24–0.39) with PASI. The second question of “Symptoms and feelings” regarding embarrassment was weakly correlated with PASI during the first year of treatment. The rest of the individual questions showed negligible correlations with PASI during the 5-year treatment period (Table SIII). For correlation between changes in PASI and changes in the individual question in DLQI, the highest correlation was observed between changes in PASI and changes in the first question of “Symptoms and feelings” (Table SIV).
In this study of 1,677 Danish patients receiving biologics or apremilast for psoriasis, weak-to-moderate correlations coefficients were found between changes in PASI and DLQI during the first 12 months of treatment and between PASI and DLQI during a 5-year treatment period. The first question on “Symptoms and feelings” demonstrated the strongest correlation with PASI, and changes in PASI for the individual questions of DLQI, and contributed most to the overall DLQI.
Previous studies have demonstrated weak correlations between relative changes in PASI and DLQI from baseline to weeks 10–16 (13, 14), moderate correlation for percentage changes in both PASI and DLQI (29) and in a systematic review of randomized clinical trials (RCT) a strong correlation was demonstrated between mean percentage reduction in PASI and mean reduction in DLQI (34). In the same review patients achieving PASI75 showed clinically meaningful higher reductions in mean DLQI compared with those achieving PASI50–75 and PASI < 50 (34) and in RCTs, patients achieving PASI90 reported lower DLQI than those achieving PASI75–89 (11), and a higher proportion of patients achieving PASI100 report a DLQI of 0 or 1 compared with patients achieving PASI75–< 100 (35).
In the current study, correlations between changes in PASI and DLQI were highly dependent on how these changes were assessed; relative changes in both PASI and DLQI yielded the highest correlation coefficient, and relative changes in PASI and absolute changes in DLQI the lowest. The correlations were similar to those reported in previous studies (13, 14, 29). Patients achieving higher PASI response had lower mean DLQI and higher reductions in absolute DLQI. In contrast to previous reporting (34), the difference between each group was not considered clinically meaningful (< 3.2) (36), probably because patients had lower PASI and DLQI compared with those seen in clinical trials. Nevertheless, as in previous studies (35), patients with higher clearance were more likely to report a DLQI of 0 or 1. This emphasizes the positive effects and importance of skin clearance on patients’ quality of life. Similar distributions were observed after 3, 6 and 12 months. Interestingly, we observed a lower correlation for the 3–12-month period compared with the baseline to 3 months period. Although speculative, this may indicate that patients early in the treatment are more satisfied with relative improvements compared with later in their treatment course, and that patients might change their perception upon treatment success. This notion is supported by correlations between PASI and DLQI during treatment, which varied throughout the 5-year period and that an absolute low PASI was associated with a low DLQI. Introducing the recent proposed DLQI-R (30) did not alter the correlations between PASI and DLQI. Interestingly, once a certain disease severity was reached an additional worsening was not reflected in quality of life. This might indicate that DLQI is not comprehensive to describe impact on quality of life for patients with severe psoriasis, and possibly underestimates disease severity in these patients (37). The use of DLQI-R might overcome this problem; however, we observed similar results for DLQI-R in this study (data available on request).
The relatively low correlation at some time-point illustrates that DLQI might ensure other relevant information about perceived disease severity and treatment advantages than PASI alone. However, the contribution of the individual questions in DLQI was skewed, and for some questions more than half of the patients scored 0. This indicates some questions in the DLQI to be of little or no relevance to a lot of patients, whereas symptoms are important for most patients. In addition to the DLQI, a symptom scoring index, i.e. Psoriasis Symptom Inventory (38), could add to the patient’s perspective and might be beneficial in the daily clinic. Moreover, patients with healthy skin might also report high DLQI, i.e. wearing a wool sweater might itch and impact on choice of clothes; thus factors other than psoriasis can add to the overall DLQI.
Certain limitations should be considered when interpreting the present findings. Although the overall data capture was good, some patients had missing data at different time-points. While these data were considered to be missing completely at random, we cannot refute that patients with a high DLQI were more likely to be registered in the DERMBIO registry, which would have biased towards the null, i.e. no correlation. An important limitation is the fact that our study comprised a highly selected population of patients treated either with biologics or apremilast, which may differ from patients treated with, for example, conventional systemics. However, only 3 patients received apremilast, and the results might not apply for this treatment. Strengths of the study include the well-characterized nature of our population, the high number of patients, prospective data collection, the use of widely established measures, i.e. PASI and DLQI, and the high external validity owing to the routinely collected data from daily clinical practice.
In conclusion, this study found that the correlation between PASI and DLQI is weak-to-moderate and varies over time, where changes in PASI correlate weak-to-moderately with changes in DLQI during the first 12 months. The DLQI might not capture the full patient disease perspective, and additional measures to capture subjective symptoms might be beneficial in future studies and daily practice.
The study was financially supported by an unrestricted grant from DERMBIO.
Conflicts of interest. The DERMBIO registry has entered into agreements with Abbvie, Eli Lilly, MSD, Novartis, Pfizer, Janssen, and Leo Pharma. They receive post marketing data and had no influence on the data collection, statistical analyses, manuscript preparation or decision to submit. NDL has been an honorary speaker for Eli Lilly. AE has received research funding from Pfizer, Eli Lilly, the Danish National Psoriasis Foundation, and the Kgl Hofbundtmager Aage Bang Foundation, and honoraria as consultant and/or speaker from AbbVie, Almirall, Bristol-Meyers Squibb, Leo Pharma, Samsung Bioepis Co., Ltd, Pfizer, Eli Lilly, Novartis, Galderma, and Janssen Pharmaceuticals. MKR has been a consultant or served on Advisory Boards with Janssen Cilag, Abbvie and Novartis, and has had paid consultancies and lectures from Abbvie, Eli Lilly, Novartis and LEO Pharma. He reports carrying out clinical trials for Eli Lilly. RG has severed on advisory boards and/or received lecture honorariums from: Novartis, Janssen, Eli Lilly, Mallincrodt, Abbvie, Leo Pharma, Amgen, Celgene, Merck. TND has received compensation as a speaker and member of an advisory board for Janssen-Cilag and Abbvie. LI has served as a consultant and/or paid speaker for and/or participated in clinical trials sponsored by: AbbVie, Almirall, Amgen, Astra Zeneca, BMS, Boehringer Ingelheim, Celgene, Centocor, Eli Lilly, Janssen Cilag, Kyowa, Leo Pharma, MSD, Novartis, Pfizer, UCB. LS has been a paid speaker for Pfizer, AbbVie, Eli Lilly, Novartis and LEO Pharma, and has been a consultant or served on Advisory Boards with Pfizer, AbbVie, Janssen Pharmaceuticals, Almirall, Celgene, UCB, Novartis, Eli Lilly, LEO Pharma and Sanofi. She has served as an investigator for Pfizer, AbbVie, Eli Lilly, Novartis, Regeneron and LEO Pharma and received research and educational grants from Pfizer, AbbVie, Novartis, Sanofi, Janssen Pharmaceuticals and Leo Pharma. LEB has no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize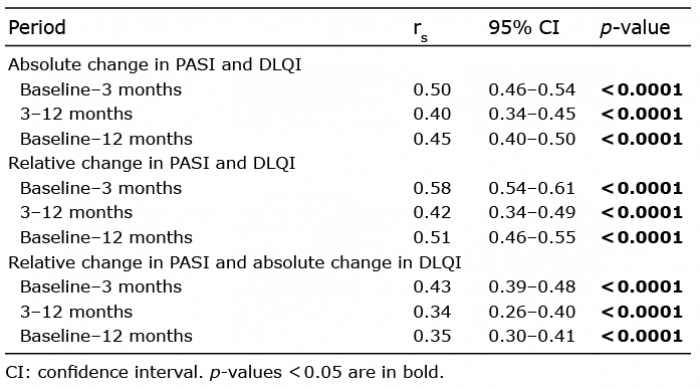 Click to show fullsize
Click to show fullsize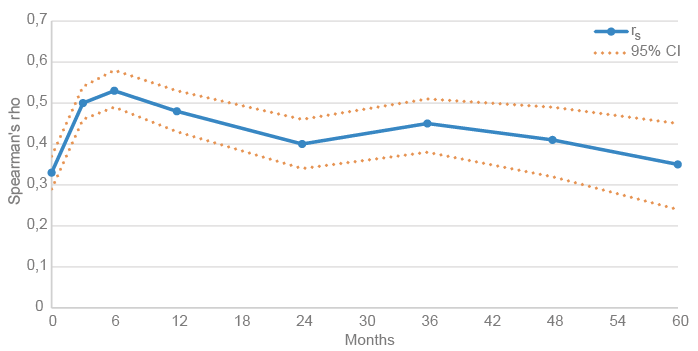 Click to show fullsize
Click to show fullsize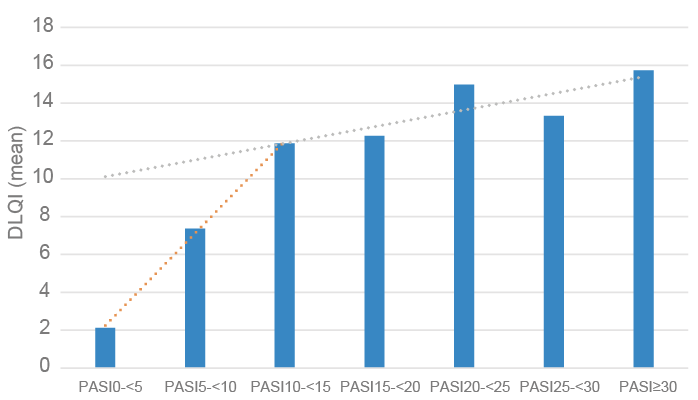 Click to show fullsize
Click to show fullsize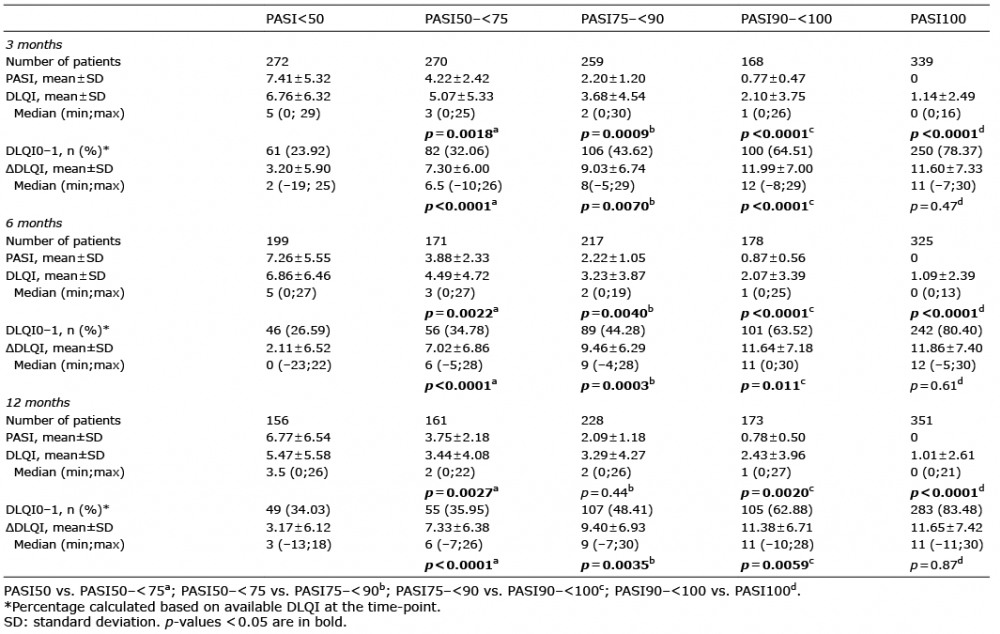 Click to show fullsize
Click to show fullsize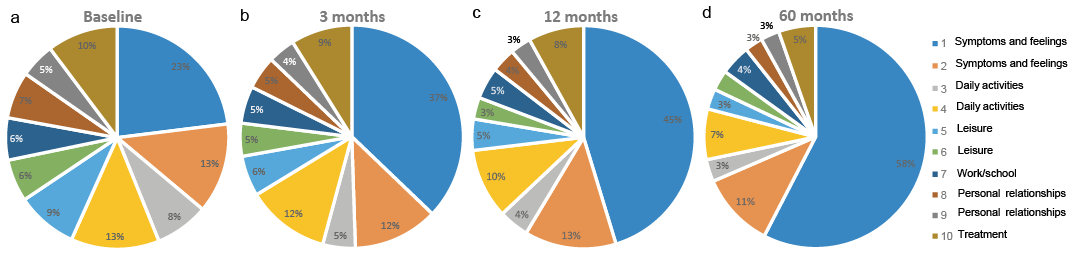 Click to show fullsize
Click to show fullsize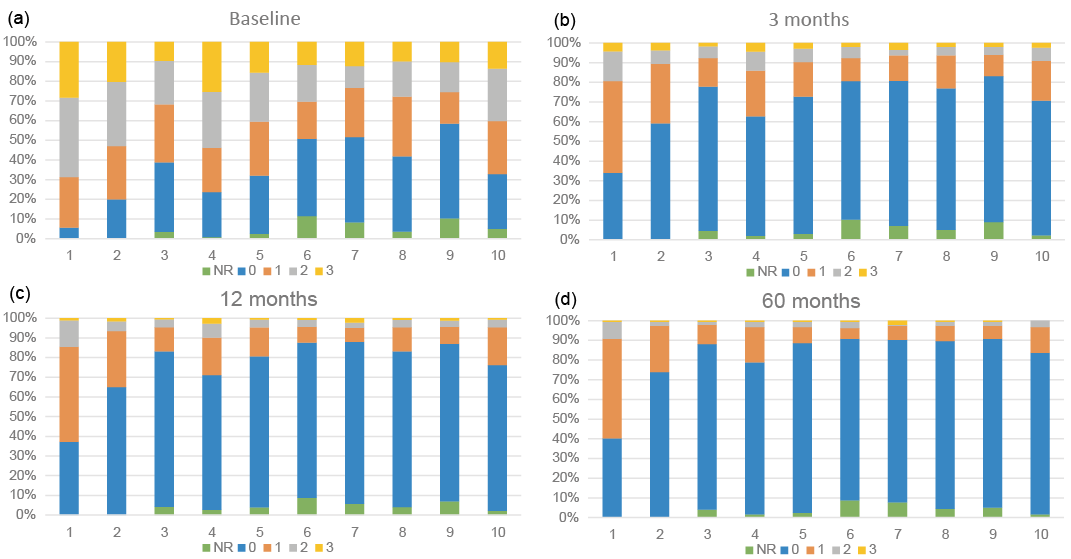 Click to show fullsize
Click to show fullsize