


Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College, 12, Jiangwangmiao Street, Nanjing 210042, Jiangsu Province, China. *E-mails: whs33@vip.sina.com, lxf3568@163.com
#These authors contributed equally to this paper.
Accepted Oct 16, 2019; E-published Oct 17, 2019
Pulmonary infection with Mycobacterium szulgai, which resembles tuberculosis, is the most common clinical presentation of this pathogen, especially in immunocompromised individuals. Extrapulmonary infections with M. szulgai are very rare. We report here a case of extrapulmonary multifocal cutaneous infections with M. szulgai and review previous cases.
A 36-year-old man with no history of tuberculosis or immuno-suppression treatment presented with multifocal asymptomatic erythematous nodules and plaques with exudate on his left hand, right ear and left elbow for 20 years (Fig. 1). He had damaged his left little finger 20 years previously in an accident with a sickle. His finger had subsequently been amputated at the local hospital due to repeated inflammation with no response to antibiotics. One year after the amputation, the same lesions were noted on the same site and spread to his right ear and left elbow. He was a heavy smoker (approximately 1 pack per day). He had no diabetes, hypertension or other comorbidities, and no family history of tuberculosis or other infections. Routine laboratory tests were normal and the patient was negative for HIV and anti-extractable nuclear antigen (anti-ENA) autoantibodies. Chest X-ray and computed tomography (CT) did not reveal any abnormal lesions. Three mycological cultures were performed with no positive results. Histopathology of a biopsied specimen from 3 sites of involvement revealed the same pathological reaction pattern; pseudoepitheliomatous hyperplasia with intraepithelial abscesses, and suppurative granuloma formations were present with peripheral mixed infiltration of lymphocytes, neutrophils, eosinophils, plasmacytes and multinuclear giant cells (Fig. 2). Neutrophil abscesses were focally formed. Löwenstein-Jensen medium was used for mycobacterial culture. Slow growth of yellow colonies occurred after 3–4 weeks of culture at 37°C. Acid-fast bacilli were positive in the tissue ?uid of skin lesion by Ziehl-Neelsen staining. The characteristics of the colonies were consistent with M. szulgai strain. Sequence analysis of hsp65 genes showed 100% similarity with M. szulgai strain. Gene sequences were analysed using BLAST V2.0 software (available from: http://www.ncbi.nlm.nih.gov/BLAST/). Gene sequencing results indicated that the strain was most likely to be M. szulgai and a diagnosis of M. szulgai infection was therefore made.
After diagnosis, the patient was treated empirically with clarithromycin (500 mg/day), ethambutol (750 mg/day) and rifampicin (450 mg/day) for 6 months. At 4-month follow-up, the patient’s skin lesions had greatly improved. Complete resolution was achieved after 6 months of antimycobacterial therapy. The patient’s skin lesions recovered completely without relapse during a 36-month follow-up.
Fig. 1. Clinical manifestations before and after treatment. Before treatment: erythematous plaque on (A) the dorsum of the left hand, (B) the left elbow, and (C) the right ear. After 3 months of treatment: lesions on: (D) the dorsum of the left hand, (E) the left elbow, and (F) the right ear. After 3 months of treatment: (G) scar and hypopigmentation on the dorsum of the left hand, (H) scar on the left elbow, and (I) scar on the right ear.
Fig. 2. (A) Suppurative granuloma formation (haematoxylin and eosin staining). Original magnification ×200. (B) Acid-fast bacilli were positive in the tissue fluid of skin lesion. Ziehl-Neelsen staining. Original magnification ×200.
M. szulgai is an atypical mycobacterium that was first discovered in 1972 (1). M. szulgai infection is very rare in humans, accounting for less than 0.5% of all non-tuberculous mycobacteria infections (2, 3). Pulmonary infection with M. szulgai, which resembles tuberculosis, is the most common clinically involved site, while extrapulmonary and multifocal infections are very rare. Only 11 cases of cutaneous infection due to M. szulgai have been reported in the literature in English, including subcutaneous nodules (4, 5), abscesses (6), cellulitis, and sinuses (7), as well as multiple inflammatory lesions (8). Sporotrichoid ulcerating lesions (9) and lichen scrofulosorum-like lesions have also been reported (10). Most cutaneous infections due to Mycobacterium occur in patients in an immunosuppressed condition, while in recent years, it has also been reported that GATA-2 deficiency (11) as well as anti-cytokine autoantibodies, including autoantibodies to interferon-γ and autoantibodies to granulocyte–macrophage colony-stimulating-factor (GM-CSF) have been proved as a predisposing factor, which could answer the unexplained disseminated NTM infections in otherwise apparently immunocompetent people, especially in Asian-born persons (12). Diagnosing this unusual infection requires a series of laboratory tests, such as culture and sequence analysis to identify and exclude diagnoses. To date, there is no standard protocol for the treatment of M. szulgai infection. M. szulgai responds well to antimycobacterial combination treatment (13). Based on clinical experience, the most recommended therapeutic regimen includes 3 or 4 antimycobacterial agents for 3–6 months or longer (14). In a report from the Netherlands, clarithromycin with ethambutol and rifampin or rifabutin was preferred as a favourable treatment regimen. Clarithromycin was a mainstay of therapy in 11 of 12 of their cases (92%), with success in 10 of 12 (83%) (15). In addition to traditional drugs, M. szulgai is also susceptible to macrolides and fluoroquinolones. In this case, the patient’s lesions obviously improved under the antimycobacterial regimens for 3 months. Thus, it is considered that traditional treatments are effective for M. szulgai infections to some degree. In conclusion, M. szulgai is a pathogenic organism that, in rare cases, causes cutaneous infection, which can be treated successfully with anti-tuberculosis drugs.
This manuscript was supported by grants from Chinese Academy of Medical Sciences: Innovation Fund for Medical Sciences (CIFMS-2017-I2M-1-017) and the Natural Science Foundation of China (81371751).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize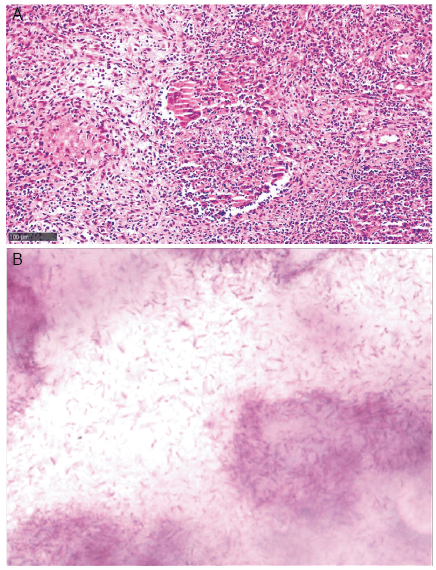 Click to show fullsize
Click to show fullsize