


1Department of Clinical Sciences, Lund University, and Department of Dermatology, Skåne University Hospital, 2Division of Cancer Epidemiology, Department of Clinical Sciences, Lund University, 3Department of Oncology and Pathology, Skåne University Hospital, 4Department of Clinical Sciences, Lund University, and Department of Surgery, Skåne University Hospital, and 5Department of Clinical Sciences, Lund University, and Division of Dermatology, Helsingborg Hospital, Lund, Sweden
Prospective observational studies have shown previously that study participants have lower morbidity and mortality than non-participants. The aim of the current study was to determine whether participants in a prospective cohort study on melanoma have a different incidence and mortality of melanoma compared with non-participants and the background population. Information was collected from Swedish National Registers on participants (n = 30,501) and non-participants (n = 10,499) in the “Melanoma In Southern Sweden” (MISS) study and the background population (n = 243,032). Hazard ratios were calculated for overall incidence of cancer and melanoma, and all-cause and melanoma-specific mortality, using Cox regression. Participants had a lower overall incidence of cancer and all-cause mortality than non-participants and the background population. There was no difference in incidence of melanoma or melanoma-specific characteristics between participants and the background population. In conclusion, participants in the MISS study have a slightly better general health, but are a representative sample of the population with regard to studies of melanoma risk factors.
Key words: malignant melanoma; incidence; mortality; cohort study.
Accepted Oct 28, 2019; E-published Oct 30, 2019
Acta Derm Venereol 2020; 100: XX–XX.
Corr: Åsa Ingvar, Department of Clinical Sciences, Cancerepidemiology, SE-22100 Lund, Sweden. E-mail: asa.ingvar@skane.se
People who agree to participate in research studies have been shown to have a lower incidence of cancer and lower mortality compared with people who are non-participants. It is not clear whether the incidence of the disease that is being studied is different in participants. We wanted to find out if this was the case in our melanoma cohort study, which was initiated in 1990. The results showed that there was no difference in melanoma incidence or mortality between participants, non-participants and the background population. In conclusion, our study sample is a representative sample of the background population with regard to studies on risk factors for melanoma.
Previous studies have shown that there is often a baseline difference between people who agree to participate in research studies and people who decline to participate (1–7). In general, participants have better psychiatric and somatic health and lower mortality rates (1, 3, 4, 6, 8–14). Indirect measures of health have revealed that participants have a higher socioeconomic status (SES) and are less often smokers (1, 3, 6, 9). Several studies have also found a lower incidence of cancer in participants (7–10, 15). Whether participants in prospective observational research studies also change their behaviour due to the awareness of being studied has been discussed previously (16–19). This reactivity in behaviour has been termed the observer effect or the “Hawthorne effect” and emanates from a series of workforce studies conducted at the Hawthorne Plant of the Western Electric Company, Chicago, USA, in the 1920s and 1930s (20). From these studies, the investigators concluded that the workers changed their behaviour due to attention from the study personnel, although this conclusion was subsequently questioned (20). The presence of the Hawthorne effect in observational clinical studies has been suggested many times as a possible bias, but attempts have seldom been made to quantify it. Studies that have examined the impact of the Hawthorne effect have produced conflicting results, which are probably dependent on several factors, such as the time from becoming aware of being studied until the time of measurement of behaviour change (16–19, 21).
Since the 1990s we have prospectively followed a cohort of approximately 30,000 women residing in southern Sweden. These women have received a questionnaire every 10th year, with questions about lifestyle factors and possible risk exposures, with special attention to risk factors for melanoma. The aim of the current study was to investigate whether participants in this study differ regarding melanoma incidence and mortality compared with non-participants and the eligible background population. To estimate whether a potential difference in incidence and mortality of melanoma in the participants was confined to the studied disease (i.e. melanoma) in our cohort, we also compared the overall incidence of cancer and all-cause mortality between participants, non-participants and the background population.
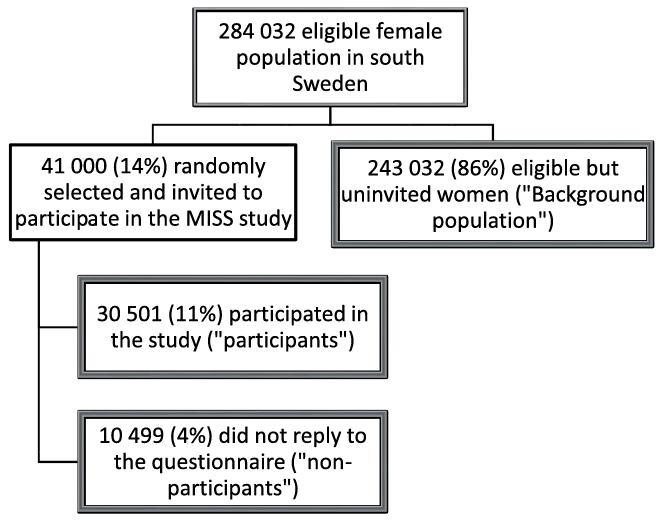
Ethical approval was granted by the ethics committee of Lund University (LU 34-92, 1992-02-12, and LU 849-06, 2006-01-21). The prospective MISS cohort study was initiated in 1990; the study methods have been described in detail previously (22–24). In short, 41,000 Swedish-born women, with no history of malignancy, were selected randomly from each year of age in the category 25-64 years, from the Population Registry in southern Sweden (Fig. 1). A baseline questionnaire was sent to the selected women at study start. A reminder letter was sent to women who did not return the baseline questionnaire within 2 months. Those who were initially invited but chose not to answer the baseline questionnaire were classified as non-participants. All other women in southern Sweden, who initially met the inclusion and exclusion criteria, but were not invited to participate in 1990, were used as the background population. For the participants only, follow-up questionnaires were sent every 10th year. The study questionnaire included questions on sun-exposure habits, marital status, educational level, smoking habits, alcohol consumption, height, weight, and physical exercise. By using the unique 12-digit personal registration number ascribed to all Swedish citizens, the participants, non-participants and the background population were linked to the Swedish Melanoma Registry (SweMR), the Swedish Cancer Registry, and the Swedish National Cause of Death Registry. Follow-up continued until emigration, death, or 31 December 2015. Incident cases of invasive melanoma and other cancers were registered during follow-up by the Cancer Registry. Only the first diagnosis of malignancy or melanoma was included in the analyses.
Since 1990, comprehensive data have been collected prospectively in the SweMR on clinical characteristics, diagnosis, histo-pathology and treatment of all invasive melanomas diagnosed in Sweden. The register has a coverage of approximately 98% (25). The current study used information on date of diagnosis, Breslow thickness, melanoma subtype, ulceration and tumour site. Breslow thickness was used as a continuous variable. Ulceration was registered as yes, or no. Melanoma subtypes were divided in superficial spreading melanoma, nodular melanoma, lentigo malignant melanoma, acral lentiginous melanoma, and undetermined subtype. Tumour site was categorized as head/neck, trunk, upper extremities, lower extremities and hands/feet/subungual.
Fig. 1. Flowchart of formation of the 3 comparison groups: participants, non-participants and background population.
Statistical analyses
Inception was defined as the date when the questionnaires were distributed to the participants and non-participants, and the same date was used for the eligible background population. Time to event analyses were performed using both Cox regression and log-rank test. The Cox regression used time since inception (or diagnosis) as time scale, and stratification with respect to age (< 34, 34–43, 44–53, > 53 years) at inception. However, in 2 cases, a test of the proportional hazard’s assumption based on Schoenfeld residuals indicated a deviation. In these cases, a change to age as time scale used in a late entry model solved the issue. The results did not alter much despite a clear indication from the residuals test. A p-value < 0.05 from a 2-sided test was considered statistically significant. All analyses were performed in R version 3.4.2 (26).
Of the 41,000 women initially invited to participate in the MISS study, 10,499 (26%) did not return the questionnaire (non-participants). This left 30,501 participants in the study. The background population consisted of 243,032 women (Fig. 1). Table I presents fundamental characteristics of the 3 groups compared in this study; participants, non-participants and background population. During a mean follow-up time of almost 22 years, 18.8% developed a cancer in the 3 groups taken together. The number of first melanoma occurring in participants, non-participants and the background population was 268, 73 and 2,111, respectively.
Table I. Descriptive charateristics of participants and non-participants in the “Melanoma in Southern Sweden” (MISS) study and the background population
All-cause mortality was significantly reduced in participants (hazard ratio (HR) 0.85, 95% confidence interval (95% CI) 0.83–0.88) and significantly increased in non-participants (HR 1.45, 95% CI 1.39–1.52), compared with the background population (Table II, Fig. 2). This effect was even more pronounced when comparing participants and non-participants, with a 40% lower mortality in participants. For melanoma-specific death the number of events was low (Table I) and these analyses could not demonstrate a significant difference between our 3 groups (Table II).
Table II. Hazard ratios (HR) and 95% confidence intervals (CI) of all-cause mortality and melanoma-specific mortality and overall cancer and melanoma incidence, in participants and non-participants in the “Melanoma in Southern Sweden” (MISS) study and the background population
Fig. 2. Kaplan–Meier plot of all-cause mortality, comparing participants (dashed green line), non-participants (dotted blue line) and background population (solid red line).
The overall cancer incidence was significantly reduced in participants compared with the background population (HR 0.95, 95% CI 0.92–0.97, Table II, Fig. 3), and this effect was consistent during follow-up (data not shown). In non-participants, the overall cancer incidence did not differ from the background population. However, by dividing the follow-up time into 2 intervals; up to, and after 5 years from inception, it was found that non-participants had an increased cancer incidence in the first 5 years (HR 1.12, 95% CI 1.02–1.24), but not thereafter (HR 0.96, 95% CI 0.92–1.01).
Fig. 3. Kaplan–Meier plot of overall cancer incidence in participants (dashed green line), non-participants (dotted blue line) and background population (solid red line) up to 25 years after initiation of the “Melanoma in Southern Sweden” (MISS) study.
In contrast to overall incidence of cancer, the incidence of melanoma did not differ in participants compared with the background population (HR 1.0, 95% CI 0.88–1.13). Non-participants had a non-significantly reduced incidence of melanoma (HR 0.83, 95% CI 0.66–1.05) (Table II).
Analysis of melanoma-specific characteristics could not detect a difference between the subgroups. Median age at diagnosis of melanoma was approximately 60 years (p = 0.9). Neither Breslow thickness (p = 0.5) nor ulceration status (p = 0.7) differed significantly between the 3 groups. However, data on ulceration was hampered by a large proportion of missing data, especially the first 10 years of the study, since at that time it was not routinely recorded, and was therefore difficult to interpret. There was also no significant difference in the site of melanoma (p = 1.0) or melanoma subtype (p = 0.8) between participants, non-participants and the background population.
By using data from the large population-based prospective MISS study, the current study aimed to clarify whether melanoma incidence and melanoma-specific mortality differed between participants, non-participants, and the background population. To determine whether a potential disparity was confined to the disease under study in our cohort (i.e. melanoma), overall incidence of cancer and all-cause mortality were also compared in these subgroups.
Decreased mortality in participants in research studies, compared with non-participants or the background population, has been well documented previously, and was confirmed in our study (1, 2, 7–15, 27–30). Many former studies have found participants to have a favourable composition of health indicators, such as a higher SES, not smoking, and fewer periods of hospitalization due to somatic or psychiatric disease (1, 3–6, 9, 10). Studies that have analysed specific causes of death have found that, in particular, death from cardiovascular diseases and smoking- and alcohol-related diseases are decreased in participants (7–9, 12, 28). In addition, death from cancer has been shown to be decreased in participants (7–10, 12, 27, 28, 30). The current study had no information on specific causes of death, with the exception of death from melanoma. One prior study that analysed melanoma-specific mortality found it to be decreased in the participants compared with the expected mortality rates extracted from the Surveillance, Epidemiology, and End Result (SEER) registers (9). In the current study, there was an indication of a lower melanoma-specific mortality in participants compared with non-participants and the background population, but the results were not statistically significant. The inability to reach statistical significance might be explained by the low numbers of deaths from melanoma in our subgroups, but it could also reflect that there is no true difference, and hence no solid conclusions can be drawn from these results.
As in several previous studies, there was a small, but significantly lower, overall incidence of cancer in participants, compared with the background population (7–10, 15). For non-participants, the overall incidence of cancer was not different, compared with the background population, when the entire follow-up period was analysed. However, when stratifying the follow-up time into 2 intervals (up to, and after 5 years of follow-up) it was found that non-participants had a higher risk of cancer in the first 5 years after study initiation. This effect has also been observed in other studies and probably reflects an initial self-selection bias in the study, with a greater proportion of unhealthy subjects unwilling to participate (7, 30). A few studies have also analysed a selection of cancer types and shown that, in particular, the incidence of lung, oesophagus, urinary tract, and pancreatic cancer is lower in participants than in the background population (7–10, 30). Two studies included information on melanoma incidence (9, 30). In “The Malmö diet and cancer study” a decreased incidence of melanoma was found in non-participants compared with participants (relative risk 0.61; 95% CI 0.48–0.79) (30). In a study comparing participants and non-participants in a screening trial, a significantly lower than expected incidence of melanoma was found in participating men, but not in participating women, compared with the reference population (9). In the current study, no significant difference in melanoma incidence between participating women was found, compared with the background population or the non-participants. However, the results indicate (although not significantly) that the non-participants had a reduced incidence of melanoma (HR 0.83, 95% CI 0.66–1.05). It is, unfortunately, not possible to determine if there was a true difference in our groups that the study had insufficient statistical power to reveal. A lower incidence of melanoma in the non-participants could, however, be explained by the lower incidence of melanoma in people of lower socioeconomic status (expected in the non-participants), which, in turn, could be due to lifestyle differences or less frequent participation in screening activities (30–32).
The lower all-cause mortality and overall incidence of cancer in the current study is, as in other studies, probably due to self-selection bias (sometimes termed “the healthy volunteer effect”) and baseline differences in socioeconomic status, smoking status and overall somatic and psychiatric health (9). It was not possible to confirm this assumption, since information on these characteristics and exposures were available only for the participants. It was, however, interesting that the incidence of melanoma in the participants of the current study did not differ from that in the background population. This might have several explanations. First, the expected healthy behaviours of the participants in our study might not include behaviours that minimize risk of melanoma. A prior study that investigated lifestyle risk behaviours and demographics showed that people with the highest educational level and the highest income level were more likely to use sun-screen and to have had a recent examination for skin cancer (32). People with the highest income level, but not those with the highest education level, were, at the same time, less likely to wear protective clothing or seek shade. In the same study, smokers were less likely to use sun-screen or wear protective clothing, but they were as likely to seek shade or have had a recent skin examination, compared with non-smokers (32). Furthermore, in a systematic review on socioeconomic and lifestyle factors in association with melanoma, it was shown that the risk of melanoma increased with increasing body mass index and higher SES, and decreased in smokers (31). The results also indicate that the participants did not significantly change their melanoma-specific risk-behaviour in spite of becoming aware of being studied for risk factors for melanoma. Whether people change their behaviour when participating in research studies (the Hawthorne/observer effect) has been questioned previously, but there is some evidence of its existence (16–19, 21). For example, in a study of patients undergoing knee arthroscopy, the patients who were made aware of being included in a study before the operation scored significantly better on postoperative measures of psychological well-being and pain (17). In another study on faecal occult blood screening test participation, it was noted that people who, in addition to the screening test kit, also received a questionnaire regarding their views about the screening test, took up screening more rapidly (18). However, the intervention did not increase the absolute screening participation (18). Chen et al. outline important characteristics of the Hawthorne effect in a review article from 2015 (16). In summary, the Hawthorne effect follows a time-dependent curve and has a performance ceiling. Hence, the magnitude and direction of the behavioural change depend on the total time the participants are aware of being observed, and tends to first increase to a peak performance ceiling and then diminish over time. In prospective cohort studies in which participants are followed over years with a low level of postal contact with the investigators it is therefore unlikely that the awareness of being studied affects the behaviour to such an extent that it biases the results (18). Thus, no evidence of a Hawthorne/observer effect was found in the current study, which suggests that our study participants and the background population do not differ regarding behaviour or other risk factors for melanoma.
The major strengths of the current study are the population-based, prospective study design, and the use of Swedish registers, which allows for an almost complete follow-up of all study objects. Furthermore, this study included a substantial number of studied persons and a long follow-up time of more than 20 years. However, the study lacked complete information on specific cancer diagnoses, causes of death or socioeconomic status of the groups. Lastly, information on risk factors, such as sun exposure and skin type, was available only for the participants and could therefore not be controlled for in the analyses. Comparison with the background population established that the random selection of women to the MISS study was a representative sample of the population. However, we cannot exclude a possible self-selection (bias) of healthier women who agreed to participate. This would, however, not affect the internal validity of the studies in our cohort, but it might affect the generalizability of the results.
In conclusion, this study found that melanoma incidence did not differ between women participating in the MISS study and the background population. This finding confirms that the results were not influenced by an observer effect. The participants in the current study were found to represent a valid sample of the Swedish population, which supports the results of former studies on risk factors for melanoma in women, and can be used as a basis for future research.
This study was funded by M Paulsson Trust, S Paulsson Trust, Hudfonden, LMK Foundation, S.R. Gorthon Foundation, ALF yngre forskare (governmental funding of clinical research within the NHS (National Health Services)), Swedish Cancer Society, Local Hospital Funds, Berta Kamprad’s Foundation. The funders were not involved in the production or publication of the study.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize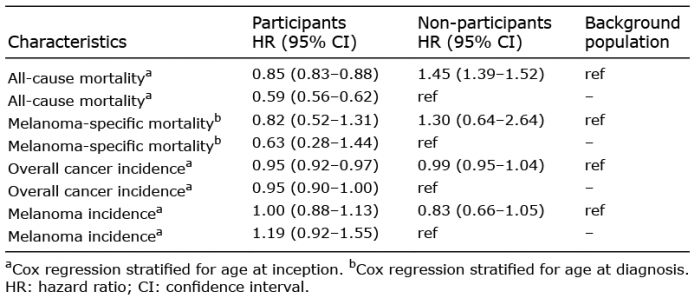 Click to show fullsize
Click to show fullsize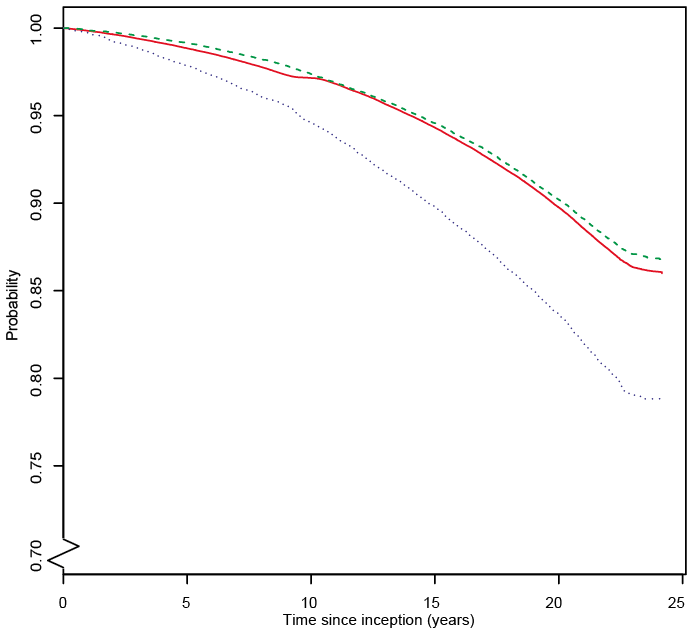 Click to show fullsize
Click to show fullsize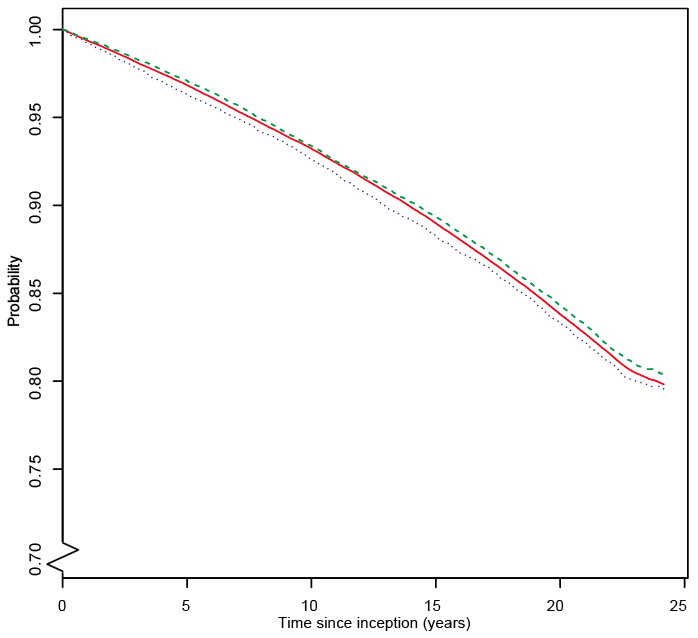 Click to show fullsize
Click to show fullsize