


Institute of Dermatology and Hospital of Skin Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, No.12 Jiangwangmiao Street, Xuanwu District, Nanjing, Jiangsu, China. *E-mail: yiqunjiang2017@163.com
Accepted Nov 27, 2019; Epub ahead of print Nov 27, 2019
Acta Derm Venereol 2020; 100: adv00048
Cutaneous lupus mucinosis (CLM) is an unusual skin manifestation of lupus erythematosus (LE), which commonly manifests as numerous papules or nodules on the neck or trunk (1). Since the first description of this condition in 1954, fewer than 50 cases have been reported in the English literature (2). Nearly all reported cases of CLM had a prior history or typical symptoms of systemic lupus erythematosus (SLE) before presentation. We report here a patient who experienced plaque-like CLM as the first sign of SLE.
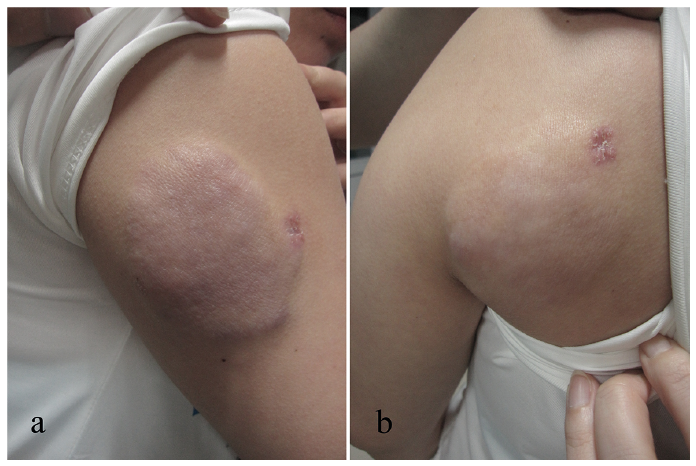
A 29-year-old Chinese woman presented with massive plaques on the left shoulder and right upper arm with no other subjective signs. The lesions had gradually increased in size over the last 2 years. She had no significant past medical history or family history of autoimmune diseases. She denied photosensitivity, fever, oral ulcer, arthralgia and other discomfort. Physical examination showed well-defined, rubbery, skin-coloured to light erythematous plaques, approximately 5 cm in diameter, on the left scapular area and the right posterior arm (Fig. 1). Biopsies were taken from both lesions, and histopathological examination revealed significantly increased mucin, highlighted by Alcian Blue stain, in-between collagen bundles involving the entire dermis. Dense perivascular and periadnexal lymphocyte infiltration was also observed. The basement membrane zone was blurred, while the overlying epidermis was unremarkable (Fig. 2). Direct immunofluorescence revealed granular deposition of immunoglobulins IgG and IgM, and complement C3 at the dermoepidermal junction. Laboratory tests showed positive antinuclear antibody (ANA) (1:160), anti-Sm and weak positive anti-dsDNA. The serum IgG level was 17.5 g/l (normal range 8.0–17.0 g/l) and the C4 level was 0.15 g/l (normal range 0.17–0.4 g/l). Complete blood count, urinalysis, blood chemistry and thyroid function were normal. The patient was diagnosed with CLM and treated with topical injection of triamcinolone and oral hydroxychloroquine with satisfactory outcomes. We then lost contact with the patient. Four years later, her primary lesions reoccurred and some erythematous plaques developed in a “butterfly” distribution on her face. Laboratory tests revealed the following abnormal values: low leukocyte count in peripheral blood (3.9 × 109/l), elevated serum IgG level (23.9 g/l), low C4 level (0.07 g/l) and positive ANA (1:640), anti-Sm, anti-dsDNA, anti-Ro/SSA, anti-RNP and anti-C1q. Urinalysis, blood chemistry, electrocardiogram and chest film showed normal results. The diagnosis was modified to SLE and the patient was treated with oral methylprednisolone and oral hydroxychloroquine. At 2-month follow-up her skin lesions had alleviated and leukocyte count returned normal.
Fig. 1. Well-defined, rubbery, skin-coloured to light erythematous plaques, approximately 5 cm in diameter, on (a) right posterior arm and (b) left scapular area.
Fig. 2. (a, b) Significantly increased mucin in-between collagen bundles, dense perivascular and periadnexal lymphocyte infiltration in the dermis. (c) The basement membrane zone was blurred, while the overlying epidermis was unremarkable. (Haematoxylin and eosin, original magnification a: ×40, b, c: ×400). (d) Mucin deposition in the dermis (Alcian blue stain, original magnification: ×40).
CLM is an uncommon variant of skin manifestations of LE, which usually presents as multiple scattered papules or nodules on the trunk and upper extremities without discomfort. Histopathologically, CLM is featured by loosening of collagen fibres with striking mucin deposition in the whole dermis. Perivascular and periadnexal infiltration of lymphocytes can also be found in CLM, while typical epidermal and interface changes in LE are rare (3).
The atypical eruptions in the current case may cause diagnostic challenges. Clinically, it should be distingui-shed from acquired cutis laxa, connective tissue naevus, reticular erythematous mucinosis and mucinous naevus. Histopathologically, tumid lupus erythematosus (TLE) can be very similar to CLM. However, the TLE lesions usually appear as urticaria-like papules and plaques on sun-exposed areas, such as the face. Patients with TLE exhibit remarkable photosensitivity, and similar lesions can be reproduced by ultraviolet A/B (UVA/UVB) irradiation in 70% of cases. In addition, TLE is seldom related to SLE. The positive rate of serum ANA is only 10% (4).
CLM has a strong association with SLE. Of the 34 cases of CLM in the English medical literature, 26 had a history of SLE and 6 had demonstrated characteristic manifestations of LE, such as malar rash, discoid LE, and arthralgia prior to CLM presentation. The serum ANA test is positive in approximately 85% of cases (5–8). It is notable that, in the current case, CLM was the first clinical symptom of SLE. This condition indicates that CLM could be the initial manifestation of SLE. Therefore, it is important to follow up these patients for early signs or symptoms of systemic involvement. The pathogenesis of mucin accumulation in CLM remains unclear. Some studies have indicated that some serum factors in patients with SLE, such as autoantibodies and cytokines, may cause upregulation of glycosaminoglycans by fibroblasts (9, 10). In our patient, the CLM lesions reoccurred with progression of SLE, suggesting that the mucin deposition is associated with autoimmunity, which is consistent with previous research.
The most effective treatment for CLM lesions has not been confirmed. Due to the presence of SLE in most cases, systemic corticosteroid and hydroxychloroquine were administered with satisfying outcomes. Systemic corticosteroid and systemic tacrolimus combination therapy also showed efficacy in another case (11). In the current case the patient’s lesions responded well to combined therapy with corticosteroid intralesional injection and oral hydroxychloroquine in the early phase of the disease, offering another therapeutic regime for CLM.
The authors thank Dr Lin Lin of the Buffalo Medical Group PC for critical review of this manuscript.
Source(s) of support: CAMS Innovation Fund for Medical Sciences (CIFMS-2017-I2M-1-017).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize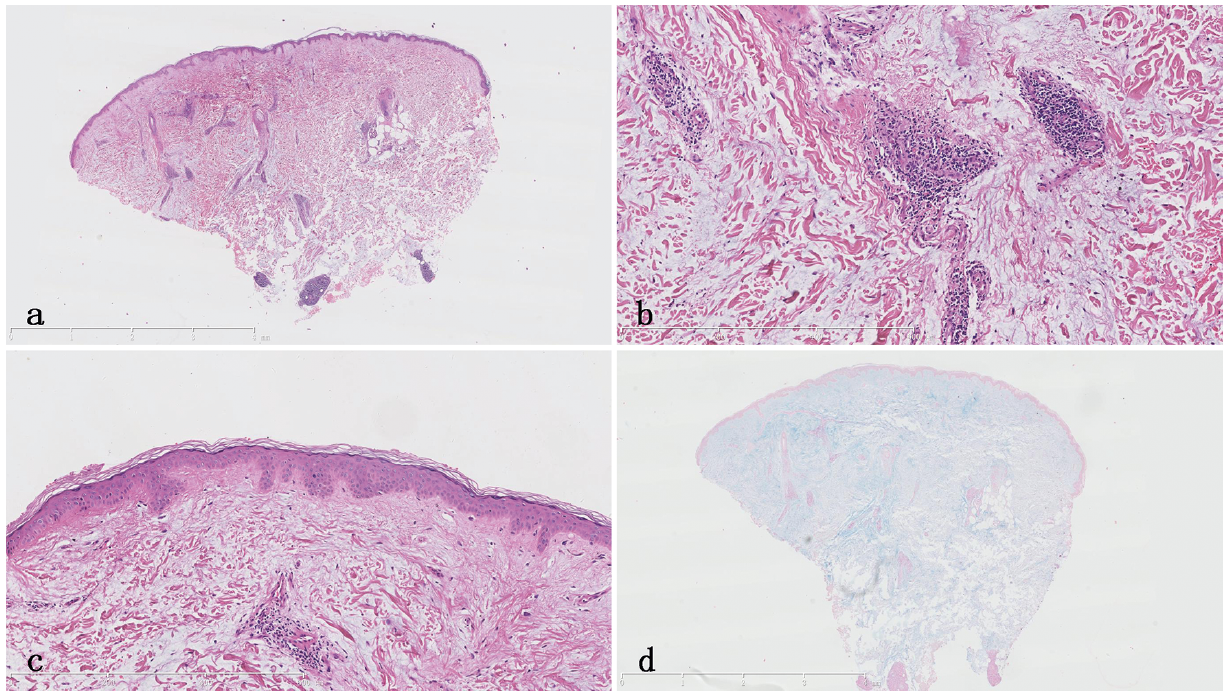 Click to show fullsize
Click to show fullsize