


1Dermatology Unit, Department of Biotechnological and Applied Clinical Science, 2Department of Pathology, 4Department of Biotechnology and Applied Clinical Sciences and 5Medical Oncology, St Salvatore Hospital, Department of Biotechnological and Applied Clinical Science, University of L’Aquila, L’Aquila, and 3Institute of Dermatology, Catholic University, Rome, Italy
#These authors contributed equally.
Mutations in MAPK signalling genes are driver events in melanoma, and have therapeutic relevance in the metastatic and adjuvant setting. This study evaluated the intra-patient heterogeneity of BRAF, NRAS and c-KIT mutational status between 30 primary melanomas and 39 related metastases, using molecular analysis and immunohistochemistry. BRAF mutations were identified in 46.7% of primary melanomas and 48.7% of metastases and NRAS mutations in 20% and 25.6%, respectively. Intra-patient heterogeneity was detected in 13.3% of patients for both BRAF and NRAS genes and was not associated with clinico-pathological characteristics of melanomas or metastases. High consistency was observed between immunostaining and molecular methods for BRAFV600E (k = 0.90; p < 0.001) and NRASQ61R (k = 0.87; p < 0.001). These findings demonstrate a relevant intra-patient heterogeneity between primary and metastatic lesions that is independent of clinical variables and methodological approach.
Key words: melanoma; metastases; BRAF; NRAS; c-KIT; heterogeneity.
Accepted Nov 27, 2019; Epub ahead of print Nov 27, 2019
Acta Derm Venereol 2020; 100: adv00040.
Corr: Maria Concetta Fargnoli, Dermatology Unit, Department of Biotechnological and Applied Clinical Science, University of L’Aquila, Via Vetoio, Coppito, IT-67100 L’Aquila, Italy. E-mail: mariaconcetta.fargnoli@univaq.it
Cutaneous melanoma is one of the most aggressive and treatment-resistant tumours. Intra-patient concordance of mutations in genes, such as BRAF, NRAS and c-KIT, between primary melanoma and related metastases is a critical aspect that has become even more relevant with the introduction of therapies targeting specific mutations. This study evaluated the intra-patient heterogeneity of BRAF, NRAS and c-KIT mutational status in 30 primary melanomas and 39 related metastases, using molecular analysis and immunohistochemistry. Clinically meaningful intra-patient heterogeneity was found between primary melanoma and related metastases, independent of the technical approach, thus supporting the polyclonal model of melanoma progression.
Melanoma is considered one of the most aggressive cancers, with an increasing incidence worldwide over recent decades (1). The treatment of metastatic disease has been a challenge in the recent past, with a low survival rate of approximately 20% at 5 years for stage IV patients (2–5). Nevertheless, the introduction of new therapeutic approaches, such as targeted therapy and immunotherapy, based on a growing understanding of molecular alterations involved in melanoma pathogenesis, has significantly improved outcomes for patients (6).
The most relevant molecular pathway implicated in melanoma pathogenesis is the mitogen-activated protein kinase (MAPK) cascade, which is dysregulated in approximately 80% of melanomas (7). Within this pathway, mutations in BRAF, NRAS and c-KIT are considered driver events and have a strong clinical relevance for melanoma treatment (8–10). Activating BRAF mutations occur in approximately 50% of cutaneous melanomas, mainly at codon 600 in exon 15, with the most common mutation being the V600E change (identified in approximately 80% of cases) (8). Oncogenic NRAS mutations are found in 15–25% of cutaneous melanomas and are usually detected at codon 61, mainly with a glutamine to arginine/lysine/leucine substitution (Q61R/K/L) (8). Finally, approximately 3% of all melanomas carry somatic mutations in exons 11 (L576P) and 13 (K642E) of the c-KIT gene, but additional c-KIT aberrations might include mutations in exon 17 and gene amplifications (8). Mutations of BRAF, NRAS and c-KIT are usually identified by molecular methods (11), but immunohistochemical (IHC) analysis represents a useful option, being widely available, less labour-intensive and less expensive (11–14). However, there is no consensus so far on the best testing method (11).
Mutational concordance between primary melanoma and related metastases is a critical aspect that has become even more relevant with the introduction of therapies targeting specific mutations of driver genes (15). Intra-patient molecular heterogeneity between primary and metastatic lesions may exist, and changes in mutational pattern might occur during progression (16). Data on heterogeneity have been reported mainly for the BRAF gene (17–26) and found in 13–15% of patients in 2 recent meta-analyses, with different rates depending on the type of tested metastatic tissue (16, 27). However, differences across the studies could also reflect technical issues, since higher heterogeneity rates have been reported for molecular approaches than for IHC-based methods (28). Few studies have focused on the intra-patient concordance of NRAS mutations between primary and metastatic lesions, with percentages of discordance ranging from 0 to 9% (17, 24, 26, 29). No data are available on c-KIT mutational heterogeneity in cutaneous melanoma.
This study aimed to investigate the mutational status of BRAF, NRAS and c-KIT genes in patients with metastatic melanoma in order to evaluate the intra-patient molecular heterogeneity between primary tumour and related metastases and to compare the consistency of mutational findings obtained by molecular and IHC analyses.
Patients’ and tissue samples
Patients with a histopathologically confirmed diagnosis of metastatic melanoma were recruited between January 2012 and December 2017 at the Department of Dermatology, University of L’Aquila, Italy. For each patient, tissues were retrieved from the primary melanoma and at least one metastasis. Patient’s clinical information including sex, age at diagnosis, anatomical site of primary melanoma and related metastases and AJCC stage 8th edition (30) were collected.
Haematoxylin-eosin-stained sections of primary and metastatic tissues were reviewed by 2 experienced pathologists (MDP and GC) to confirm the diagnosis. The following clinico-pathological features of primary tumours and/or metastasis were collected: anatomical location, histopathological variant, Breslow thickness, presence of ulceration, number of mitoses/mm2, presence of melanoma-associated naevus and CSD (histologically defined according to the degree of solar elastosis).
Approval for this study was obtained from the Ethics Committee of the ASL-01 Avezzano, Sulmona, L’Aquila (protocol number 0012038/11). Written informed consent was provided by all patients. The study was performed according to the principles of the Declaration of Helsinki.
Molecular analysis
Somatic DNA was extracted from 5 formalin-fixed paraffin-embedded (FFPE) tissue sections (each 10-micron in thickness) obtained from the same tissue block used for IHC, by microdissection of marked tumour-rich areas from primary melanoma and metastases using a QIAmp DNA Micro tissue kit (Qiagen, Hilden, Germany) according to the manufacturer’s instructions.
Exon 15 of BRAF, exon 2 of NRAS, and exons 11, 13 and 17 of c-KIT were screened by Sanger sequencing. Briefly, PCR amplification of the regions of interest was performed in a Simply-Amp PCR-System (Thermo-Fisher, Foster City, CA, USA) using primers listed in Table SI. PCR experiments were performed as described previously (14). Amplicons were sequenced on 3500 Genetic-Analyzer (Thermo-Fisher). The variants were detected using the Applied Biosystems Minor Variant Q11 Finder software version 1.0 (Thermo Fisher), specific to calling low-frequency somatic variants. Competitive allele-specific TaqMan™ PCR (castPCR™ Technology) assays were used to confirm sequencing results in BRAF and NRAS wild-type samples and if discrepancies were found between molecular analysis and IHC. PCRs containing 20 ng DNA, 1X TaqMan™ Mutation Detection Assays (BRAFV600E, Hs00000111_mu; BRAFV600K, Hs000000002_rm; NRASQ61R, Hs00000808_mu; NRASQ61L, Hs00000807_mu; NRASQ61K, Hs00000804_mu; NRAsQ61H, Hs00000809_mu), 1X TaqMan™ Genotyping Master Mix (Thermo-Fisher) and water to reach a final volume of 20 µl were performed using the standard TaqMan protocol on a 7500 Fast Real Time-PCR System (Thermo-Fisher). Positive and negative controls were used for experiments of mutation detection.
c-KIT copy number was assessed by quantitative real-time PCR for exon 13 and compared with GAPDH as an internal control, as described previously (29). Briefly, PCR reactions were performed using PowerUP™ SYBR™ Green Master Mix (Thermo-Fisher), with a 20 µl total volume and 50 ng genomic DNA on a 7500 Fast Real Time-PCR System. Primers for c-KIT exon 13 and GAPDH are listed in Table SI. The thermal cycling conditions were as follows: 2 min at 50°C and 10 min at 95°C, followed by 45 cycles of 95°C for 15 s and 60°C for 1 min. Each gene was analysed in triplicate. Samples that did not amplify by 35 cycles were considered to be of insufficient quality and were excluded from the analysis. For each sample, ΔCt for c-KIT vs. GAPDH was calculated as ΔCt = Ct (c-KIT) – Ct (GAPDH) and then calibrated to individual reference genomic DNAs from 3 normal skin tissue samples and confirmed by calibration to a commercial human genomic reference DNA (Thermo-Fisher). Relative copy number evaluation was performed by the comparative 2-ΔΔCt method and converted to absolute copy number by assigning a value of 2 to the reference DNA.
Immunohistochemistry
IHC was performed on FFPE tissue sections of 4 µm thickness. The presence of BRAFV600E and NRASQ61R mutants and c-KIT expression were evaluated using the following monoclonal antibodies: BRAFV600E VE1 clone (Spring Bioscience, Pleasanton, CA, USA), NRASQ61R SP174 clone (Spring Bioscience), and CD117/c-Kit polyclonal (Spring Bioscience) at a dilution of 1:30, 1:80 and 1:100, respectively. Sections were freshly cut, dried at 60°C for 30 min, deparaffinized and rehydrated. Immunoreactions were performed on Ventana BenchMark GX automatic immune stainer (Ventana Medical Systems Inc., Tucson, AZ, USA) using the Ultra View Universal Alkalin Phosphatase Red Detection Kit, as previously reported (13). No chromogen was detected when primary antibody was omitted. Positive controls were mounted on each section subjected to immunostaining. Negative controls were included in each run.
The evaluation of IHC status was performed independently by 2 observers (MDP and GC) blinded to the molecular mutational status; disagreement was resolved by consensus. Cytoplasmic staining of BRAFV600E VE1, NRASQ61R SP174 and CD117/c-Kit polyclonal antibodies in melanoma cells was considered as positive or negative and graded for intensity, according to previously published criteria (14, 31). Staining for BRAFV600E VE1 and NRASQ61R SP174 was considered positive if the percentage of stained melanoma cells was more than 10% and classified as homogeneous (staining in > 95% of cells) or heterogeneous (staining in < 95% of cells) (14). Negative staining was defined either as absence of any cytoplasmic labelling or staining of single interspersed melanoma cells (< 10%). Intensity of staining was graded as weak, moderate or strong (14). CD117/c-Kit staining was assessed on the percentage of stained cells and strength of staining: 0, no staining; 1+, weak staining in isolated groups of melanoma cells; 2+, weak and widespread staining in <50% of melanoma cells; 3+, moderate staining in 50–75% of melanoma cells; 4+, strong staining in >75% of melanoma cells. Staining was classified as positive in the presence of moderate/strong membranous and cytoplasmic staining (3+/4+) and as negative if there was absence of cytoplasmic staining and if staining was weak and widespread (0/1+/2+).
Statistical analysis
For statistical analysis, categorical variables for primary melanoma were grouped as follows: anatomical site (head/neck, trunk, extremities, acral), histopathological subtype (superficial spreading melanoma [SSM], nodular melanoma), chronic sun damage (CSD or no CSD), presence of ulceration (yes, no), number of mitoses/mm2 and presence of melanoma-associated naevus (yes, no). Synchronicity (defined as a metastasis diagnosed at the same time as the primary melanoma) and anatomical site (skin, lymph node, visceral, brain) were recorded for metastases.
Semi-quantitative data (age at diagnosis, Breslow thickness) were analysed by means of Student’s t-test or by medians with Mann–Whitney test. Univariate analysis by χ2 test or by Fisher’s exact test was used to test the significance of mutation frequency according to clinico-pathological characteristics of melanoma patients and tumours. Molecular findings were used as the gold standard for statistical analysis. Cohen’s k coefficient test was used to measure the agreement between molecular and IHC methods in determining BRAF and NRAS mutational status. Samples harbouring the BRAFV600K mutation according to molecular analysis, that were wild-type on IHC VE1 staining, were not considered for Cohen’s k analysis. p-values less than 0.05 were considered statistically significant. Statistical analysis was performed using the statistical package SPSS 17.0 (SPSS Incorporated, Chicago, USA).
Patients’ and tumour samples
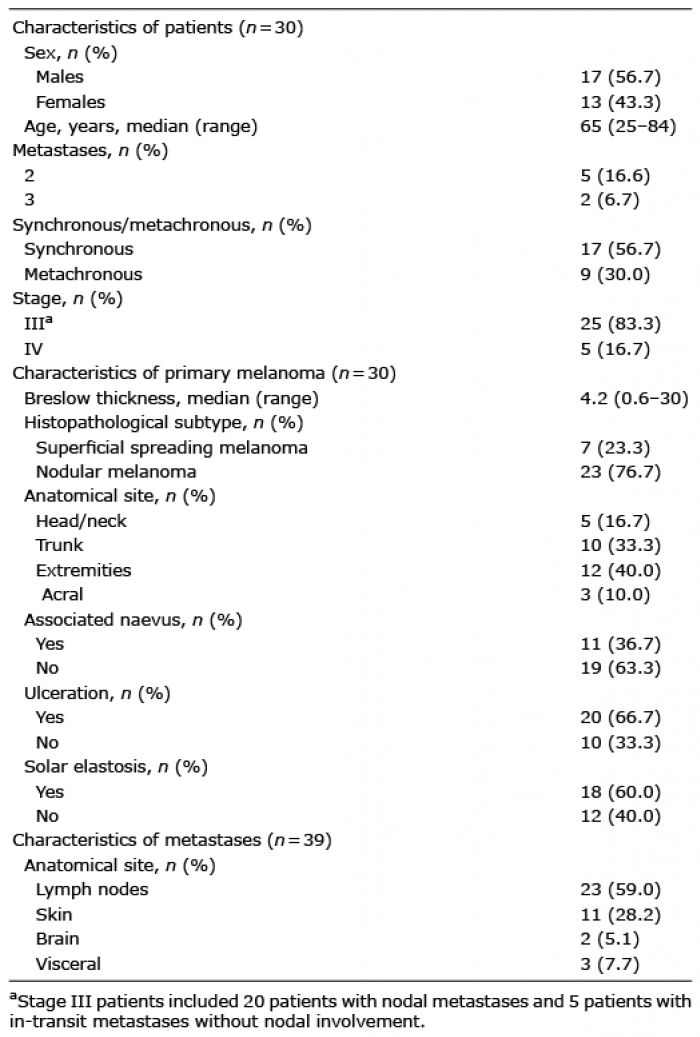
Overall, a total of 69 tumour tissues (30 primary melanomas and 39 related metastatic lesions) were collected from 30 patients with advanced melanoma (25 stage III and 5 stage IV). Enrolled patients included 17 males and 13 females, with a median age at first diagnosis of 65 years (range 25–84 years). In detail, 23 patients were diagnosed with 1 metastasis, 5 with 2 metastases and 2 with 3 metastases. Demographic and clinical characteristics of patients and tumour tissues are reported in Table I.
Table I. Demographic and clinical characteristics of melanoma patients and histopathological features of tumours and metastasis
Twelve primary melanomas (12/30, 40.0%) were located on the extremities, 10 on the trunk (10/30, 33.3%), 5 (5/30, 16.7%) on the head/neck region and 3 (3/30, 10.0%) on acral sites. The majority of tumours were of the nodular histological subtype (23/30, 76.7%) followed by SSM (7/30, 23.3%); no acral lentiginous or lentigo maligna melanomas were diagnosed in our group of patients. Median Breslow thickness was 4.2 mm (range 0.6–30 mm). A pre-existing melanocytic naevus was associated in 36.7% (11/30) of primary melanomas.
The majority of metastatic tissues were collected from lymph nodes (23/39, 59.0%), followed by skin (11/39, 28.2%), brain (2/39, 5.1%), colon (1/39, 2.6%), liver (1/39, 2.6%) and parathyroid gland (1/39, 2.6%). Median time to first metastasis was 3 months (range 0–51 months). Meta-stases were synchronous in 17 (17/30, 56.7%) patients and metachronous in 9 (9/30, 30.0%); 4 (4/30, 13.3%) patients had both synchronous and metachronous metastases.
Molecular analysis
The distribution of BRAF, NRAS and c-KIT mutations in all analysed tissues is shown in Table II. BRAF mutations at codon 600 were detected in 33 of 69 (47.8%) tumour tissues, with 23 harbouring the BRAFV600E (23/33, 69.7%) and 10 the BRAFV600K (10/33, 30.3%) mutation. Distribution of BRAF mutations was similar between primary melanomas (14/30, 46.7%) and metastatic samples (19/39, 48.7%) (p = 0.42). Sixteen of 69 tumour tissues (16/69, 23.2%) carried NRAS mutations at codon 61 with the following genotypes: NRASQ61R (8/16, 50.0%), NRASQ61L (7/16, 43.7%) and NRASQ61K (1/16, 6.3%). Among the 16 NRAS mutated tumours, 6 were primary melanomas (6/30, 20.0%) and 10 (10/39, 25.6%) metastatic samples (p = 0.61). Finally, only 1 missense c-KIT mutation, L802F mutation in exon 17, was detected in one (1/69, 1.4%) primary melanoma diagnosed on the upper extremity. A mutation in at least 1 of the 3 genes was present in 21 of 30 (70.0%) primary melanomas and 29 of 39 (74.3%) metastatic samples, for a total of 72.5% tissues (50/69). All tissues were mutually exclusive for BRAF, NRAS and c-KIT mutations (Table II). c-KIT gene amplification was carried out in 65/69 (94.2%) samples with 4 samples missing due to lack of DNA. An increased copy number (≥ 3 copies) was identified in 3 (3/69 4.3%) samples, with 2 of them being primary melanomas with a high level of chronic sun damage (CSD). All cases with c-KIT amplification carried concomitant BRAFV600 mutation (BRAFV600K in 2 cases and BRAFV600E in one case).
Table II. Summary of mutational patterns in primary and metastatic melanoma samples according to immunohistochemical and molecular analyses
A significant association between mutational status and clinical characteristics of the primary melanoma was observed only for median age at melanoma onset (Table III). Patients with BRAFV600 mutated melanomas were younger than those with BRAF wild-type melanomas (57 vs. 74 years, p < 0.01), while NRAS mutations were more prevalent in older patients (77 vs. 60 years, p < 0.01). A higher trend of NRAS mutations were found in primary melanomas showing CDS, as evaluated by histological solar elastosis (p = 0.06).
Table III. Frequency of BRAF and NRAS mutations according to clinical and histopathological characteristics of patients and tumours
An intra-patient concordance of BRAF mutational status between primary melanoma and related metastases was detected in 86.7% (26/30) of patients, with 9 (9/26, 34.7%) concordant for BRAFV600E, 3 (3/26, %) for BRAFV600K, and 14 (14/26, 53.8%) for the wild-type genotype (Table II and Fig. 1). Intra-patient BRAF molecular heterogeneity was observed in 13.3% (4/30) of patients. Notably, all patients (7/30, 23.3%) with multiple metastases showed a consistent BRAF mutational status between primary melanoma and all analysed metastatic tissues. Concerning NRAS mutational profile, a concordant NRAS mutational status was observed in 26 of 30 (86.7%) patients, with the majority (21/30, 70.0%) a wild-type genotype (Fig. 1). Among the 4 discordant cases (4/30, 13.3%), 3 (3/4, 75%) showed wild-type primaries and mutated metastases with the following genotypes Q61R, Q61L and Q61K (Table II). Concordance rate of BRAF and NRAS mutational status did not differ by sex, timing of metastases appearance or metastatic site (Table SII).
Fig. 1. Illustrative cases of BRAF and NRAS mutational status in primary melanoma and related metastasis by sequencing and immunohistochemistry. (A, B) Intra-patient NRAS concordance. (A) Primary melanoma and (B) cutaneous metastasis: positive NRASQ61R SP174 immunostaining and NRASQ61R mutation sequencing in both lesions. Magnification ×10. (C, D) Intra-patient BRAF and NRAS heterogeneity. (C) Primary melanoma: negative BRAFV600E VE1 immunostaining and BRAF wild-type on mutation sequencing. Identification of the NRASQ61K mutation. (D) Metastatic lymph node: positive BRAFV600E VE1 immunostaining and BRAFV600E mutation sequencing. Magnification ×10.
Regarding the single patient mutated for c-KIT, a discordant mutational status was observed between his primary and meta-static lesion.
Considering the overall somatic profile of all BRAF/NRAS/c-KIT genes, intra-patient heterogeneity was present in 23.3% (7/30) of patients (6 with 1 metastasis and 1 with 2 metastases). Discordance rates were not associated with sex, synchronicity or anatomical sites of metastasis (Table SII).
Immunohistochemistry
A total of 26 (26/69, 37.7%) samples showed positive immunostaining with anti-BRAFV600E VE1 antibody with homogenous staining in 19 of 26 (73.1%) tissues. Staining intensity was strong in 22 tumours (22/26, 84.6%), moderate in 3 (11.5%) and weak in 1 (1/26, 3.9%). Overall, primary melanomas (12/30, 40.0%) and metastatic lesions (14/39, 35.9%) showed similar frequency of BRAFV600E staining (p = 0.46). Regarding NRAS, 10 tumour tissues (10/69, 14.5%) were positive for NRASQ61R SP174 immunostaining and 59 were negative (59/69, 85.5%). Staining intensity was strong in 8 tumours (8/10, 80.0%), and moderate or weak in 1 (1/10, 10.0%) each. No significant difference was observed in the frequency of NRASQ61R positive staining between the groups of primary melanomas (5/30, 16.7%) and metastatic lesions (5/39, 12.8%) (p = 0.45).
All 11 melanomas arising in association with a melanocytic naevus showed concordance for BRAF and NRAS between melanoma cells and naevus cells, with 5 of them (5/11, 45.4%) showing positive immunostaining for BRAFV600E and 3 (3/11, 27.3%) for NRASQ61R; the remaining cases were negative for both mutations (Fig. 2).
Sixteen tumours tissues (16/69, 23.2%) showed positive CD117/c-KIT expression, with 13 cases presenting a moderate and 3 cases a strong immunostaining. A trend for a higher prevalence of positivity was observed in the group of primary melanomas (9/30, 30.0%) than in metastatic samples (7/39, 17.9%), although not statistically significant (p = 0.06).
Fig. 2. BRAFV600E VE1 staining in naevus-associated melanoma. Concordant positive BRAFV600E in melanoma and naevus. (A) Haematoxylin and eosin staining, (B) BRAFV600E VE1 staining. Magnification ×20.
Considering the mutational findings obtained by IHC, the intra-patient BRAFV600E concordance between primary lesions and related metastases was present in 27/30 (90.0%) patients, including 10 (10/30, 33.3%) with BRAFV600E-positive lesions and 17 (17/30, 56.7%) negative. Intra-patient BRAFV600E heterogeneity was observed in 10.0% (3/30) of patients (Fig. 2). For NRASQ61R, the majority of patients (29/30, 96.6%) showed an intra-patient concordant immunostaining between the primary lesion and related metastases, being 4 (4/30, 13.3%) consistent for NRASQ61R positivity and 25 (25/30, 83.3%) for negative staining. A discrepant NRASQ61R staining was observed in 1 patient (3.3%). Finally, intra-patient concordance of CD117/c-KIT expression between primary lesions and related metastases was present in 22/30 (73.3%) patients, including 3 (3/30, 10.0%) with positive and 19 (18/30, 63.3%) with negative tissues (Table II). Three patients with multiple metastases showed heterogeneity among their tumour tissues.
Correlation between molecular analysis and immunohistochemistry
BRAFV600E VE1 immunostaining was consistent with BRAF molecular findings in 56 of 59 (94.9%) tissues, with 23 (23/56, 41.1%) BRAFV600E mutated and 33 (34/56, 60.7%) wild-type (Table III). The 10 (10/69, 14.5%) samples harbouring a BRAFV600K mutation were indeed negative on IHC VE1 staining and were not included in this analysis. Discrepant findings were found in 3 of 59 (5.1%) samples: all cases were positive for immunostaining, but wild-type on molecular testing (both Sanger sequencing and competitive allele TaqMan™ PCR). Two discordant (2/3, 66.7%) cases (1 primary melanoma and 1 metastasis) had a moderate and heterogeneous BRAFV600E VE1 staining pattern, while the remaining sample (1 primary melanoma) presented a strong positive and homogeneous staining. BRAFV600E VE1 antibody sensitivity was 100.0%, specificity 91.7%, accuracy 94.9%. Overall, the agreement between molecular testing and IHC was “almost perfect” (Cohen’s kappa = 0.90; p < 0.001).
SP174 NRASQ61R immunostaining and NRAS molecular analysis showed a high rate of consistency (60 of 61 cases, 98.4%), with 8 (8/60, 13.3%) tissues carrying the NRASQ61R mutation and 52 (52/60, 86.7%) the wild-type genotype. Cases carrying other NRASQ61 mutations showed no IHC SP174 staining and were not included in the analysis. Only one primary melanoma resulted positive for IHC NRASQ61R with weak and heterogeneous staining pattern, but wild-type at the molecular analysis. The sensitivity of the SP174 NRASQ61R antibody was 100.0%, specificity 96.2%, and accuracy 96.7%. Overall, the agreement between molecular testing and IHC was “almost perfect” (Cohen’s kappa = 0.87; p < 0.001).
Regarding c-KIT gene, no mutation was found in all 16 samples with a high level of CD117/c-KIT by IHC, while 2 of the 3 (66.7%) cases with c-KIT gene amplification showed increased expression of CD117/c-KIT.
This study identified BRAF mutations in 46.7% of primary melanomas and in 48.7% of metastases and NRAS mutations in 20% and in 25.6%, respectively. The intra-patient molecular heterogeneity between primary melanoma and related metastases was detected in 13.3% of patients for both BRAF and NRAS genes and was not associated with clinico-pathological characteristics of melanoma or metastases. We demonstrated consistency of BRAFV600E and NRASQ61R mutational findings obtained by molecular analysis and IHC immunostaining for both overall mutation frequencies and intra-patient heterogeneity with an “almost perfect” agreement.
Recently, 4 different molecular melanoma subtypes were proposed based on the type of driver MAPK activating gene mutation, i.e. BRAF (35–50% of cases), NRAS (10–25%), NF1 (~ 15%) mutated and triple-wild-type melanomas (~10%) including c-KIT mutated lesions (32). These oncogenic alterations have been associated with different clinico-pathological aspects of patients or tumours, such as age, anatomical site and degree of cumulative sun exposure (CSD or not CSD) (7).
Intra-patient molecular heterogeneity between primary melanoma and related metastases has important implications in clinical practice when metastatic patients with discordant lesions need to be treated with targeted therapy. In addition, comparison between primary lesions and related metastases can provide insights into the processes involved in metastatic progression. We observed an intra-patient discrepancy in BRAF mutations between primary and metastatic lesions in 13.3% of patients, as evaluated by molecular methods, in line with the discordance rate of 13.4% and 15.5% reported in 2 recent meta-analyses (16, 27). A true biological manifestation of tumour heterogeneity, but also technical issues (molecular-based methods compared with IHC-based) have been hypothesized to explain these discrepancies (16, 27, 28). A higher mutational discordance rate has been reported with the increasing number of metastases, i.e. 8% in patients with one metastasis, 18% in patients with 2 metastases, and 20% in patients with 3 metastases (16). All our patients with multiple metastases (23.3%) showed a consistent BRAF status between primary melanoma and all metastatic tissues.
Regarding NRAS, the intra-patient discordance rate was reported to range from 3% to 14.3% of cases in few small studies (24, 26, 29), while no discrepancy was found in one study (17). A 13.3% discordant rate was observed in our patients, with the majority of them acquiring the NRAS mutation over time as part of disease progression.
Controversial results were reported for the rate of intra-patient BRAF or NRAS discrepancies according to the site of metastasis, with a suggested, but not confirmed, higher rate of discordance between primary melanoma and visceral metastases compared with lymph node metastases (17). The discrepancy rate for locoregional lymphatic metastases was indeed reported to range from 9.2% to 38% across 4 previous studies (19, 21, 26, 33), while for visceral metastases, including brain, from 13% to 50% (26, 33, 34). In the current study no differences were observed in the heterogeneity rate between primary melanoma and lymph node or visceral metastatic sites.
The intra-patient heterogeneity between primary melanoma and related metastases has been hypothesized to be due to the specific detection method, with a higher rate of heterogeneity for molecular methods than for IHC approaches (12, 19, 23, 25, 27, 28). Therefore, we compared BRAFV600E and NRASQ61R mutations using molecular methods (Sanger sequencing and allele-specific Taqman™ assays) and IHC. We observed very consistent findings between immunostaining and molecular methods for BRAFV600E mutation, as detected in 95% of our samples, and for NRASQ61R found in 98% of cases. Interpretation issues have been reported for weak and moderately stained lesions, as in 3 of our 4 discordant cases, since they have been considered either positive or negative in the literature, thus suggesting that caution is necessary in case of unclear staining (13, 35). In addition, a rare VE1 antibody cross-reactivity with an unknown epitope may also be a possible explanation for false-positive staining (36, 37). Overall, in our cases the intra-patient heterogeneity between primary melanoma and metastatic tissues does not seem to be attributable to methodological aspects, since it was similar for IHC and molecular methods, thus possibly reflecting the true biological heterogeneity during melanoma progression.
Few small studies have investigated the concordance rate of BRAFV600E and NRASQ61R mutations between naevus and melanoma in naevus-associated melanomas (14, 38–40). For BRAF gene, a concordance rate varying from 75% to 100% was reported in 4 studies (14, 38–40) and for NRAS, 91% of melanomas and associated naevi were concordant in one study (39). All 11 naevus-associated melanomas in our series showed a concordant of BRAFV600E and NRASQ61R status between melanoma and naevus cells by immunostaining.
This study has a few limitations. NF1 mutational analysis was not performed, since the clinical significance of NF1 mutations in melanoma is unknown and the interest as a potential therapeutic target is currently scarce. In addition, this study did not have adequate statistical power to evaluate intra-patient heterogeneity of c-KIT mutations, probably due to the low prevalence of acral lentiginous and mucosal melanoma subtypes. Finally, our results on intra-patient heterogeneity are mainly referred to lymph node metastasis due to the low number of visceral metastasis in our sample that might have underestimated the overall discordance rate. However, the evaluation of the discordance rate between primary melanoma and nodal metastases in disease-free patients is nowadays important for administration of targeted therapies in the adjuvant setting.
These findings confirm that a relevant intra-patient heterogeneity between primary melanoma and related metastases exists independently of the technical approach, thus supporting the polyclonal model of melanoma progression. In addition, IHC and molecular methods provided highly consistent results in the detection of BRAFV600E and NRASQ61R mutations, supporting IHC as a rapid and cost-effective screening method in melanoma, although a combined approach is necessary in cases with negative or doubtful immunostaining.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize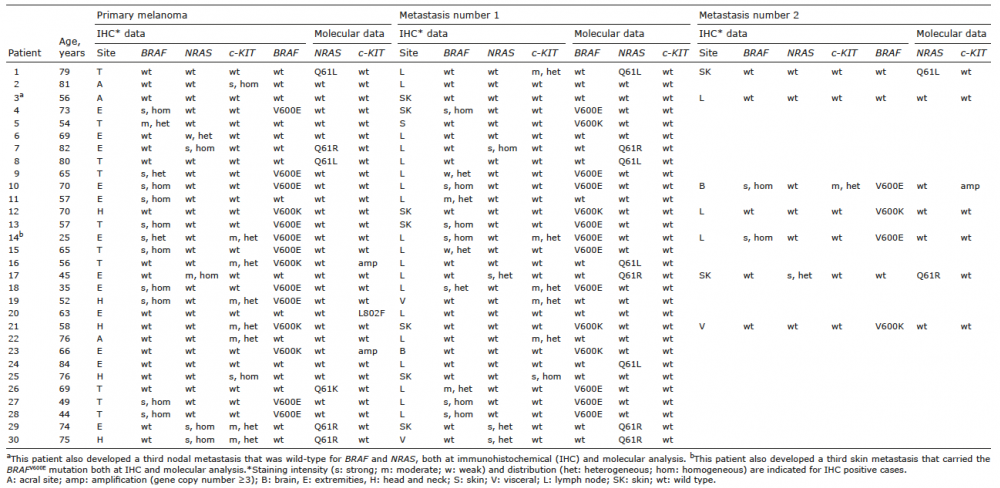 Click to show fullsize
Click to show fullsize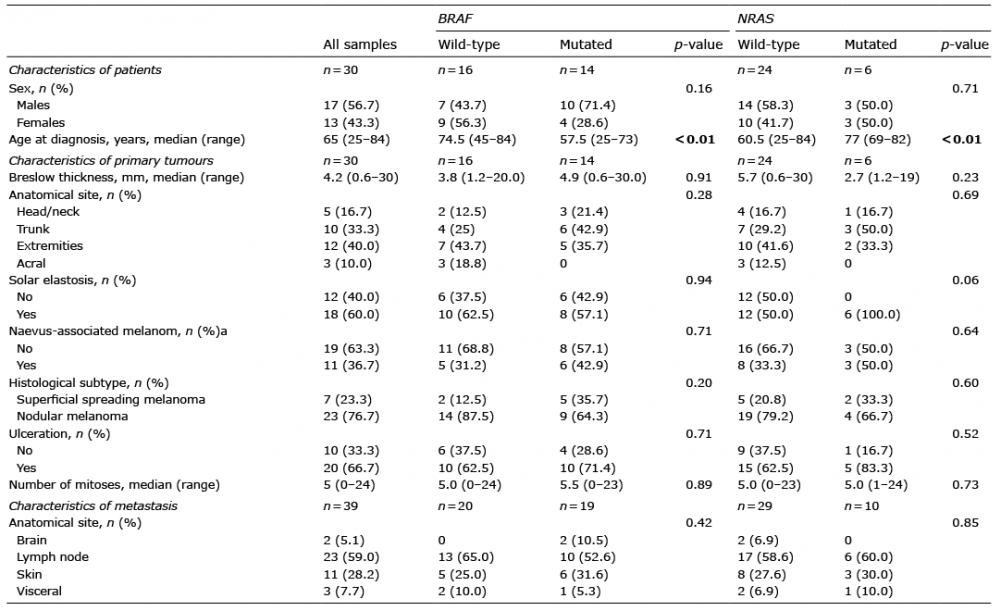 Click to show fullsize
Click to show fullsize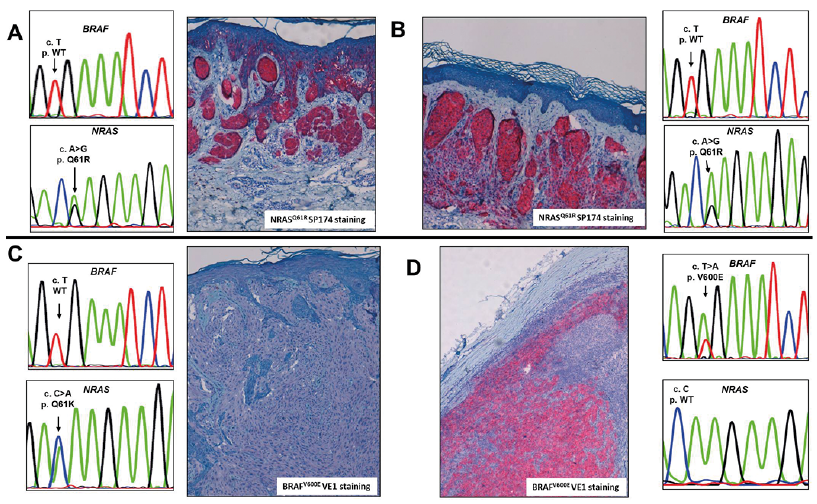 Click to show fullsize
Click to show fullsize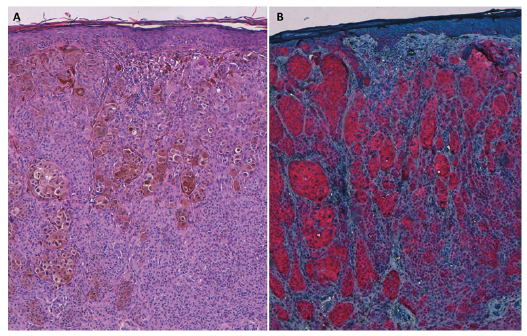 Click to show fullsize
Click to show fullsize