


1Hyperhidrosis Clinic, Empano, Copenhagen, Denmark, 2Department of Dermatology and Allergy Centre, Odense University Hospital, Odense, Denmark, and 3Svettmottagningen, Stockholm, Sweden. E-mail: johannes.kristensen@dadlnet.dk
Accepted Dec 10, 2019; Epub ahead of print Dec 10, 2019
Acta Derm Venereol 2020; 100: adv00044
Primary hyperhidrosis has been associated with anxiety and depression, but the magnitude of the alleged association is largely unknown. The aim of this study was to perform a systematic review of the association between primary hyperhidrosis, depression and anxiety.
The medical databases PubMed, Embase and PsycINFO were searched using the following terms: primary hyperhidrosis AND depression OR suicide OR suicidal ideation OR antidepressants OR anxiety OR anxious OR panic attacks OR worry OR anxiolytic. All studies in English examining the relationship between patients with primary hyperhidrosis and either depression or anxiety were reviewed according to title and abstract. Furthermore, studies were identified by screening reference lists and citations lists of key articles and review articles.
The aim of this review was to include controlled studies examining the association between primary hyperhidrosis and depression and/or anxiety. Therefore the databases were searched for studies that employed validated screening instruments.
A total of 842 articles were identified. After screening titles and abstracts, 815 articles were excluded and 27 were obtained for full-text review. Of the 27 screened articles 20 were excluded due to a lack of relevant control groups or screening instruments. A final total of 7 studies were analysed further.
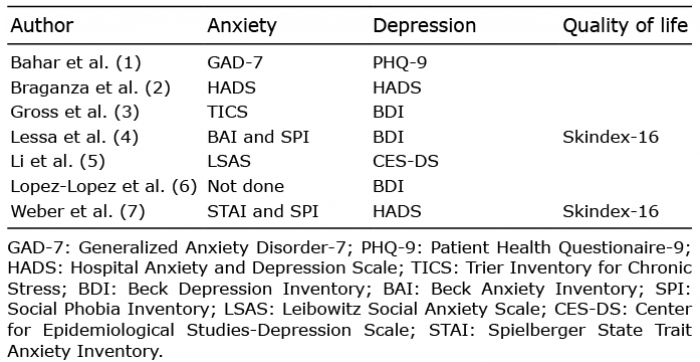
The anxiety screening instruments used were: Generalized Anxiety Disorder-7 (GAD), Hospital Anxiety and Depression Scale (HADS), Trier Inventory for Chronic Stress (TIC), Beck Anxiety Inventory (BAI), Social Phobia Inventory (SPI), Leibowitz Social Anxiety Scale (LSAS), and Spielberger State Trait Anxiety Inventory (STAI) (Table I).
The depression screening instruments used were: Patient Health Questionaire-9 (PHQ), HADS, Beck Depression Inventory (BDI), and Center for Epidemiological Studies-Depression Scale (CES-DS) (Table I).
Bahar et al. (1), in Canada and China, examined dermatology patients in Vancouver and Shanghai. They selected patients with primary hyperhidrosis and “late onset hyperhidrosis” and stratified these into groups according to the type of hyperhidrosis (axillary, palmar, plantar, facial, etc.). They found that patients with hyperhidrosis were significantly more anxious and depressed than any other group of dermatology patients (21.3% and 27.2% vs. 7.5% and 9.7%, respectively) (p < 0.001 for both). Patients with generalized or facial hyperhidrosis were most severely affected. A total of 2,017 dermatology patients (437 with hyperhidrosis) was examined.
Braganza and co-workers (2), from Brazil, found significantly more anxiety (49.6%) but not depression (11.2%) in 197 patients with primary hyperhidrosis. They stated that patients with either axillary or facial hyperhidrosis were most anxious, but that even patients with plantar or palmar hyperhidrosis were anxious.
Gross et al. (3), in Germany, compared 40 patients with primary hyperhidrosis (axillary, palmar and plantar) with 40 age- and sex-matched normal control subjects. Twenty-four out of 40 (60%) vs. 4 out of 40 scored over the cut-off in BDI-II (p < 0.002).
Lessa et al. (4), in Brazil, compared 17 patients with primary focal hyperhidrosis (areas not stated) with 29 dermatology patients. As symmetrical sweating was an inclusion criterion it might have been palmar, plantar or axillary. Normal results were found with the BDI and BAI. Significantly more hyperhidrosis patients with comorbid social phobia were found with the SPI (47%, p < 0.019). Severely decreased quality of life was found with Skindex-16.
Li et al. (5), from the USA, examined 106 patients with primary focal palmar hyperhidrosis before and after endoscopic thoracic sympathectomy and included a control group of 213 patients undergoing thoracic surgery. Of these, 17.6% had anxiety and 16.7% had depression.
López-López et al. (6), from Spain, examined 100 dermatology patients (some with known primary hyperhidrosis) and compared patients scoring HDSS 1 (n = 55) with patients scoring HDSS 2–4 (n = 45).
The areas involved were not clearly stated, but could involve the extremities as well as the torso. Twenty-one percent of patients with HDSS 2–4 were classed as depressed with the BDI (p < 0.001).
Weber et al. (7), in Germany, found elevated scores for social phobia in 31 patients with primary hyperhidrosis presenting for treatment with botulinum toxin. Only axillary, palmar and plantar hyperhidrosis were seen. The control group constituted the whole group of patients with primary hyperhidrosis (70 patients). Normal values were found for anxiety and depression using STAI and HADS. Quality of life improved after treatment, but the quality of life was rather high from the beginning, correlating inversely with anxiety and depression.
Table I. Screening instruments used
Anxiety values varied from zero to 49.6%, and depression from zero to 60%. Most studies concluded that anxiety and depression is common and should be considered by doctors when treating patients with primary hyperhidrosis. There is a paucity of publications in this field, thus it is essential that future research studies this question in detail. Interesting findings with Skindex-16 could promote this instrument and improve measurement of quality of life (8). We suggest using the HADS questionnaire (9), which has been validated in Sweden (10), Germany (11) and England (12). The HADS questionnaire is copyright, but can be used for non-commercial purposes for a nominal fee. A suggested relationship between quality of life, body image and depression or anxiety will, no doubt, soon be studied in skin diseases (13).
Do patients with hyperhidrosis need psychological care? Weber et al. (7) states that his patients improved considerably after treatment with botulinum toxin and without the help of a psychologist, but this question has not been studied further. In order to elucidate this subject, we plan to perform a controlled study using Skindex-16, HADS and body image questionnaires before and after treatment. We consider it important to start by relieving the physical symptoms of hyperhidrosis.
Limitations
Included studies used different definitions of hyperhidrosis, depression and anxiety. The selected patients differed. The sample sizes varied, as did the control groups, which were mostly not comprised of normal persons. The measuring instruments also varied considerably, but all were validated tools.


 Click to show fullsize
Click to show fullsize