


Department of Dermatology, Kosin University College of Medicine, Busan, South Korea
Although low-dose methotrexate (MTX) has been used widely in treatment of a variety of dermatological diseases, including multifocal primary cutaneous anaplastic large cell lymphoma (PCALCL), it has not been established for use in the treatment guidelines for solitary or localized PCALCL. Furthermore, there has been no report of long-term follow-up data in Asian patients with PCALCL treated with low-dose MTX. To investigate the effectiveness and clinical outcome of treatment with low-dose MTX, clinical and long-term follow-up data of 7 patients with solitary or localized PCALCL were analysed retrospectively. Of the 7 patients, 6 (85.7%) showed a complete response and 1 (14.3%) showed partial remission. During follow-up, mean duration of 92.1 months, 5 patients developed one or more cutaneous relapses. At the last follow-up, all of the patients with PCALCL were alive without disease. These results indicate that low-dose MTX is a highly effective and safe treatment for solitary or localized PCALCL as well as multiple relapsed lesions.
Key words: CD30-positive T-cell lymphoproliferative disorder; low-dose methotrexate; long-term follow-up; primary cutaneous anaplastic large cell lymphoma; solitary or localized lesions.
Accepted Jan 27, 2020; Epub ahead of print Jan 30, 2020
Acta Derm Venereol 2020; 100: adv00069.
Corr: Min Soo Jang, Department of Dermatology, Kosin University College of Medicine, 262 Gamcheon-ro, Seo-gu, Busan, 602-702, Korea. E-mail: ksderm77@unitel.co.kr
Primary cutaneous CD30+ lymphoproliferative disorders are the second most common cutaneous T-cell lymphoma. In the case of solitary or localized primary cutaneous anaplastic large cell lymphoma (PCALCL), surgical excision or radiotherapy are the first-line treatments. However, those options can lead to significant functional or cosmetic morbidities. Low-dose methotrexate has not been established in treatment for solitary or localized PCALCL. Furthermore, even in multifocal PCALCL, low-dose methotrexate has been proposed as first-line therapy based on only a limited number of studies. There has been no report of long-term follow-up data focused specifically on Asian patients with PCALCL treated with low-dose methotrexate. This study suggests that low-dose MTX treatment should be established as an effective alternative in the treatment guidelines for solitary or localized PCALCL, in which surgical excision and/or radiotherapy is not feasible.
According to the newly revised 2018 World Health Organization–European Organization for Research and Treatment of Cancer (WHO-EORTC) classification, primary cutaneous CD30+ lymphoproliferative disorders are the second most common cutaneous T-cell lymphoma (CTCL) after mycosis fungoides, accounting for approximately 25% of CTCL (1). Primary cutaneous CD30+ lymphoproliferative disorders denote a heterogeneous group of primary CTCL characterized by the expression of CD30 antigen and a favourable prognosis. Relapses are not uncommon in primary cutaneous anaplastic large cell lymphoma (PCALCL), occurring in approximately 40% of patients (2). The choice of treatment depends on the size, extent, and clinical behaviour of the skin lesions. Current treatment guidelines for PCALCL generally recommend the administration of low-dose methotrexate (MTX) or radiotherapy for patients with multifocal skin lesions (3, 4). Multi-agent chemotherapy has often been described as a first-line treatment for multifocal PCALCL, but is no longer recommended due to its high rate of relapse. In general, this treatment is reserved for patients developing extracutaneous involvement (3). Recently, brentuximab vedotin, an anti-CD30 monoclonal antibody, was introduced as an effective therapeutic option for patients with extracutaneous involvement or multifocal lesions in PCALCL (5). Retinoid, interferon-α, thalidomide, and topical imiquimod have been described in anecdotal reports of treatment of patients who were not responsive to other therapy (6–10).
In the case of solitary or localized PCALCL, surgical excision or radiotherapy are the first-line treatments; however, those options can lead to a large scar, fibrosis, atrophy of skin adnexa, and loss of normal range of motion, depending on the size and location of the disease (11). Although low-dose MTX has been used widely in a variety of dermatological diseases, including multifocal PCALCL, it has not been established in the treatment guidelines for solitary or localized PCALCL. Furthermore, even in cases of multifocal PCALCL, low-dose MTX has been proposed as a first-line therapy based on only a limited number of studies (12–15). To our knowledge, there has been no report of long-term follow-up data focused specifically on Asian patients with PCALCL treated with low-dose MTX. Thus, this study evaluated the treatment results and assessed the long-term follow-up data of 7 patients who initially presented with solitary or localized PCALCL, in order to investigate the efficacy of treatment with low-dose MTX.
Patients
This study included 7 outpatients diagnosed with PCALCL who received low-dose MTX treatment at the dermatology clinic of Kosin University Gospel Hospital, Busan, Korea, between January 1993 and June 2019. All cases fulfilled the clinicopathological criteria of the WHO-EORTC (4). Each slide from the previous skin biopsy was reviewed and clinically correlated with medical records including the follow-up data in order to confirm the diagnosis. Patients with PCALCL were evaluated using routine staging procedures, including complete blood count, biochemical analysis, bone marrow examination, computed tomography (CT) scan, and fluorodeoxyglucose positron emission tomography-CT (FDG PET-CT) scan, in order to exclude extracutaneous diseases. This study excluded patients with an inadequate clinical follow-up duration of less than one month or concurrent diagnosis of other primary or secondary CTCLs.
Methods
The following characteristics were recorded; age at time of diagnosis, sex, type and number of skin lesions, immunohistochemical finding of anaplastic lymphoma kinase (ALK), treatment result, site of occurrence, relapse, and status at time of the last follow-up. The term localized refers to a few clustered lesions restricted to a single anatomical area, generally not exceeding 15 × 15 cm.
Treatment response was classified as complete remission (CR), partial remission (PR), or no response (NR). CR and PR were defined as the complete disappearance and > 50% regression of the skin lesions, respectively. NR was defined as a < 50% regression in skin lesions. CR and PR were combined into the overall response. The first treatment response was assessed after 4–6 weeks of treatment with low-dose MTX. Low-dose MTX was discontinued when the tumours disappeared and the size of healed lesions (usually the hyperpigmentation or slightly depressed scar) stopped decreasing even after 2–3 further weeks of treatment. Relapses were counted when the new lesion appeared after oral MTX had been stopped. After the second assessment, regular follow-up examinations were performed every 3 months in the first 2 years and every 6 months during the next 3 years. Patients who had maintained a CR for 5 years were permitted annual or irregular follow-up examinations.
Clinical characteristics
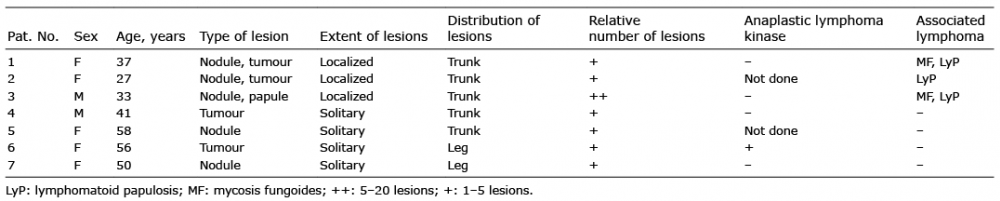
The main clinical characteristics of the 7 patients who initially presented with solitary or localized lesions are summarized in Table I. The study group included 2 men and 5 women, mean age at diagnosis 43 years (range 27–58 years). Of these 7 patients, 6 had 1–5 lesions and 1 had 5–20 lesions at first presentation. Tumours were observed in 4 patients, and papules or nodules in 5 patients. The skin lesions at first diagnosis were located on the trunk (n = 5) and legs (n = 2).
Table I. Characteristics of 7 patients with primary cutaneous anaplastic large cell lymphoma at first diagnosis
Treatment response
All 7 patients treated with low-dose MTX had presented with solitary or localized lesions. Clinical images of PCALCL before and after the treatment, are presented in Fig. 1. CR was observed in 6 patients (85.7%), while PR was observed in 1 patient (14.3%) who had undergone additional surgery. The mean initial MTX dose was 13.6 mg/week (range 5–15 mg/week). The mean time to remission was 4 weeks (range 1–7 weeks) and the mean MTX dose to achieve CR was 62.1 mg (range 15–105 mg). The mean duration of treatment was 13.2 weeks (range 5–136 weeks). More details regarding these data are presented in Table II.
Fig. 1. Clinical images of primary cutaneous anaplastic large cell lymphoma. (A) A solitary, erythematous, coin-sized nodule on the lower abdomen. (B) After 6 weeks of low-dose methotrexate (MTX) therapy, the lesion was flattened and the size decreased. (C) A solitary, erythematous, walnut-sized tumour on the left axilla. (D) After 7 weeks of low-dose MTX therapy, the lesion had healed leaving a small brownish patch of scarring.
Table II. Methotrexate therapy and follow-up data of 7 patients with primary cutaneous large cell lymphoma
Follow-up
During follow-up, 5 of the 7 patients (71.4%) developed one or more cutaneous relapses, with a mean time to relapse from each CR of 25.2 months (range 1–124 months) (Table II). After the mean follow-up duration of 92.1 months (range 4–206 months), all 7 patients were alive without disease. None of the patients had died of the lymphoma or other causes. Among the patients diagnosed with PCALCL during follow-up, stage IA (T1aN0M0 and T1bN0M02) mycosis fungoides (MF) occurred in 2 patients after 2.5 and 7.5 years, respectively. Lympho-matoid papulosis (LyP) presented in 3 patients. None of the 7 patients developed extracutaneous disease. The treatment results and follow-up data are shown in Table II and Table III, respectively.
Table III. Summary of main clinical findings and follow-up data
Adverse effects of treatment
During treatment, medications that could interact with MTX were controlled. Following the end of treatment, 3 patients (patients 1, 2 and 4) reported adverse effects including nausea (n = 2, 28.6%), anorexia (n = 2, 28.6%), fatigue, diarrhoea, dysgeusia, and dizziness (n = 1, 14.3%).
Primary cutaneous CD30+ lymphoproliferative disorders represent a spectrum of diseases, including LyP, PCALCL, and borderline cases. In the current WHO classification, the hallmark of PCALCL is the expression of CD30 in more than 75% of tumour cells (1). Histopatho-logic findings of PCALCL are presented in Fig. 2. LyP and PCALCL are sometimes difficult to distinguish using histological features, and LyP may progress to PCALCL. Because there is no clear-cut boundary between LyP and PCALCL, clinicopathological correlation is mandatory to confirm a diagnosis. In the present study, 3 of the 7 patients with PCALCL presented LyP during the follow-up period (15, 16). PCALCL lesions usually presented with a large tumour or grouped (localized) firm nodules. LyP lesions presented multiple papulonodules much smaller than PCALCL and involved discrete several anatomical sites.
Fig. 2. Histopathology of primary cutaneous anaplastic large cell lymphoma. (A) Diffuse infiltrate of atypical cells in entire dermis (original magnification ×40). (B) Large, hyperchromatic, pleomorphic and anaplastic cells (arrows) (original magnification ×400). (C) Anaplastic multinucleated tumour cells (arrows) (original magnification ×400). (D) Immunohistochemically, most tumour cells express CD30 (original magnification ×40).
LyP is defined as a chronic, recurrent, self-healing eruption of papules and small nodules that can be spread widely over the entire body. The 5-year survival rate of LyP is nearly 100%. In contrast, PCALCL generally manifests as solitary or localized, rapidly-growing, and ulcerating large tumours. Only 20% of patients present with multifocal skin lesions. Despite the name “anaplastic” and “large cell lymphoma”, the prognosis of PCALCL is favourable, with a 5-year survival rate of approximately 95%. Although PCALCL can show spontaneous regression in 25% of cases and extracutaneous involvement in only 10% of cases, patients with PCALCL require evaluation for extracutaneous involvement and specific treatment rather than wait-and-see strategies (2–4). Since it is important to differentiate PCALCL and secondary involvement of systemic ALCL, physicians may use immunohistochemical staining of tissues and medical imaging. However, there is debate about the significance of ALK positivity. Although Kempf et al. (4) reported that positive finding of ALK of the lesion raises a high suspicion of underlying systemic ALCL, there have been several case reports of ALK-positive PCALCL (4, 17). Also, ALK positivity is present in 50–85% of patients of secondary involvement of systemic ALCL (18). It should be acknowledged that there is a correlation between ALK positivity and systemic involvement. However, this cannot be applied strictly to every patient. In this study, the immunohistochemical evaluation of ALK was performed in samples of 5 patients and one of them was found to be ALK-positive. To rule out systemic ALCL, more weight was given to medical imaging, such as CT, FDG PET-CT scan, and none of the patients was found to have systemic involvement.
MTX has been used for the treatment of a variety of dermatological disorders, including psoriasis, collagen vascular diseases, atopic dermatitis, vasculitis, blistering disorders, and CTCL. The mechanism of MTX presumably relates to its anti-proliferative and anti-inflammatory effects (19). Along with psoralen and ultraviolet A (PUVA), low-dose oral MTX is the most commonly used and effective treatment for LyP, with response rates of up to 93% (20, 21).
According to current treatment guidelines, radio-therapy or low-dose MTX are recommended as first-line therapy for multifocal PCALCL. However, this recommendation is based on only a limited number of studies, and long-term follow-up data of PCALCL in Asian patients is scarce (14, 15). Vonderheid et al. (12) reported that low-dose MTX is an effective and safe treatment in patients with primary cutaneous CD30+ lymphoproliferative disorders including LyP and PCALCL, with high response rates and long-term control rates exceeding 80%. Bekkenk et al. (3) recommended low-dose oral MTX or radiotherapy for patients with multifocal PCALCL. Melchers et al. (13) reported that low-dose MTX is a suitable option in patients with more than 5 multifocal PCALCL lesions, although the response rate was lower than that of LyP. Furthermore, the authors reported an overall response rate of 57% in patients with more than 5 lesions. In most patients in the present study, fewer than 5 lesions were present. The CR and overall response rates here were 85% and 100%, respectively. The higher response rate can be considered relatively superior, mainly due to the solitary or localized distribution with small numbers of lesions in our patients compared with those in the previous studies.
Relapses are not uncommon in PCALCL, having been reported in approximately 40% of cases (2). However, the relapse rate was much higher in the present study, at 71.4%. Patients 1 and 2 experienced 5 and 10 episodes of relapse, respectively, during a 17-year follow-up period. All of the relapsed lesions were cleared up by low-dose MTX treatment. The mean time to relapse was 25.2 months, with 124 months as the longest, suggesting the need for long-term follow-up and observation. Despite the solitary or localized distribution of the lesions, the tumour size and location of the tumour may make radiotherapy or surgical excision difficult. Moreover, performing radiotherapy or surgical excision on every relapse has limitations and may cause a large scar, fibrosis, atrophy of skin adnexa, and loss of normal range of motion (11). Therefore, low-dose MTX can be a good alternative for patients with multiple relapses. In this study, the patients with multiple relapses showed good responses to low-dose MTX treatment for all relapses, without leaving significant scars.
PCALCL is also often associated with other cutaneous lymphomas, such as MF. In the current study, 2 patients with PCALCL developed MF during the follow-up period. Because transformed MF expresses CD30 antigen in 15.5–39% of patients and often presents with tumours, it may be difficult to distinguish PCALCL associated with MF from CD30-rich transformed MF (22). Low-dose MTX may be helpful to distinguish between the 2 diseases, as PCALCL usually shows high response rates to low-dose MTX, while CD30-rich transformed MF does not (23).
The adverse effects of MTX include malaise, nausea, anorexia, mucositis, headache, elevated liver transaminases, and leucopaenia. Rarely, systemic administration of MTX can lead to serious complications, such as pancytopaenia due to bone marrow suppression, liver fibrosis with hepatotoxicity, and pulmonary fibrosis (19). Regular monitoring is required through laboratory tests including complete blood counts, renal and liver function tests. In this study, 3 of the 7 patients experienced nausea, anorexia, diarrhoea, or epigastric discomfort. None of them had serious complications or stopped treatment because of adverse effects. Since the side-effect profile of the long-term use of MTX is well known, MTX can be used safely with the appropriate prediction of adverse events.
The main goal of this study was to determine the efficacy of low-dose MTX therapies for Asian patients with PCALCL with solitary or localized skin lesions. Low-dose MTX is usually well-tolerated and has few side-effects, even when prescribed for long-term maintenance treatment over months and years. Although it is associated with a high relapse rate, our data showed excellent response rates to low-dose MTX not only for initial treatment, but also for relapsed cases of solitary or localized PCALCL. The limitation of this study is the small number of cases due to the rarity of this disease in South Korea. However, the study is valuable as the first long-term follow-up study to investigate the effect of MTX in Asian patients with PCALCL. These results demonstrate that low-dose MTX is an effective and safe treatment for solitary or localized PCALCL. Large-scale, prospective, randomized, and comparative studies are needed to confirm the usefulness of MTX therapy. Low-dose MTX treatment should be established as an effective alternative in the treatment guidelines for solitary or localized PCALCL, in which surgical excision and/or radiotherapy is not feasible.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize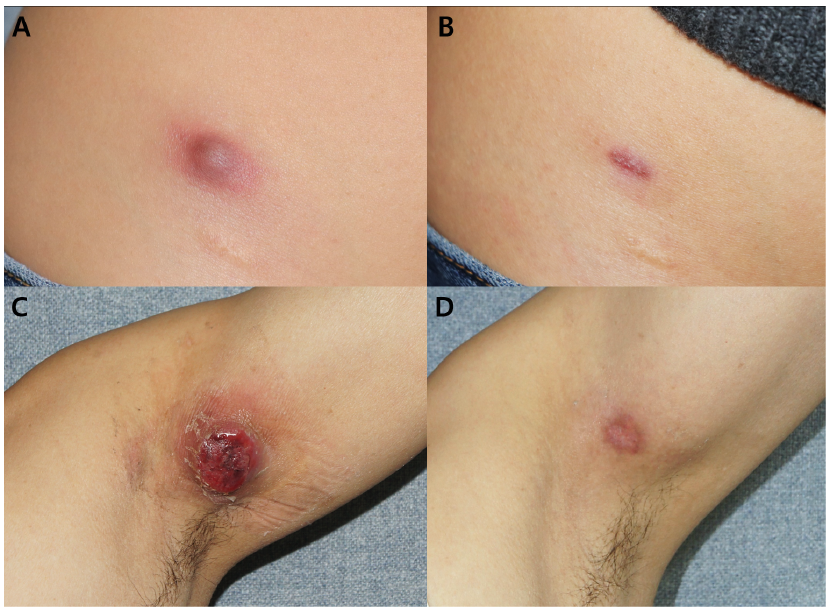 Click to show fullsize
Click to show fullsize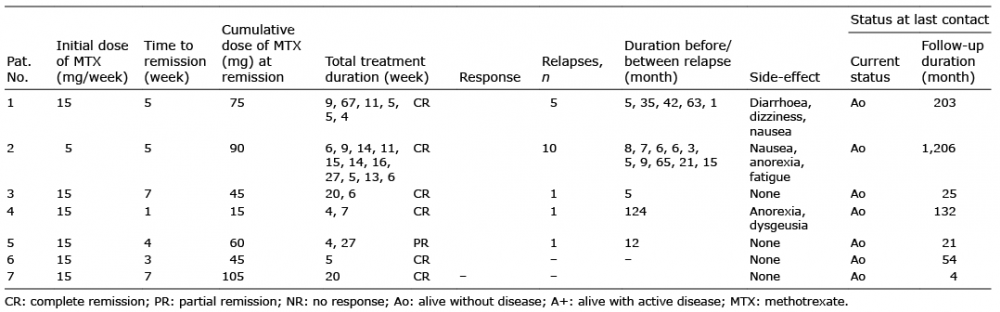 Click to show fullsize
Click to show fullsize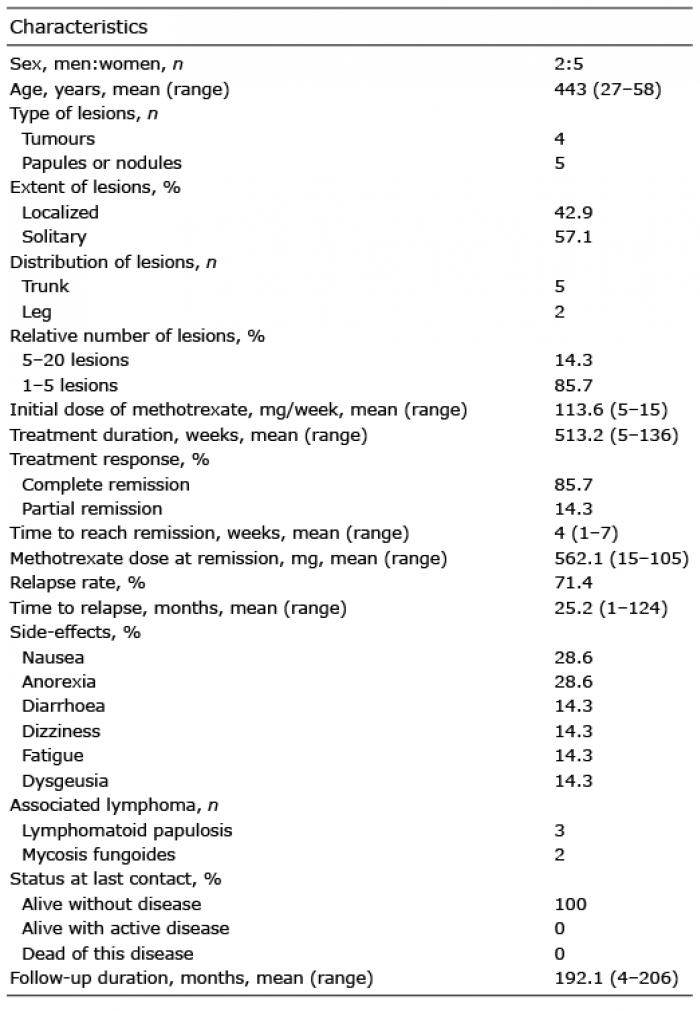 Click to show fullsize
Click to show fullsize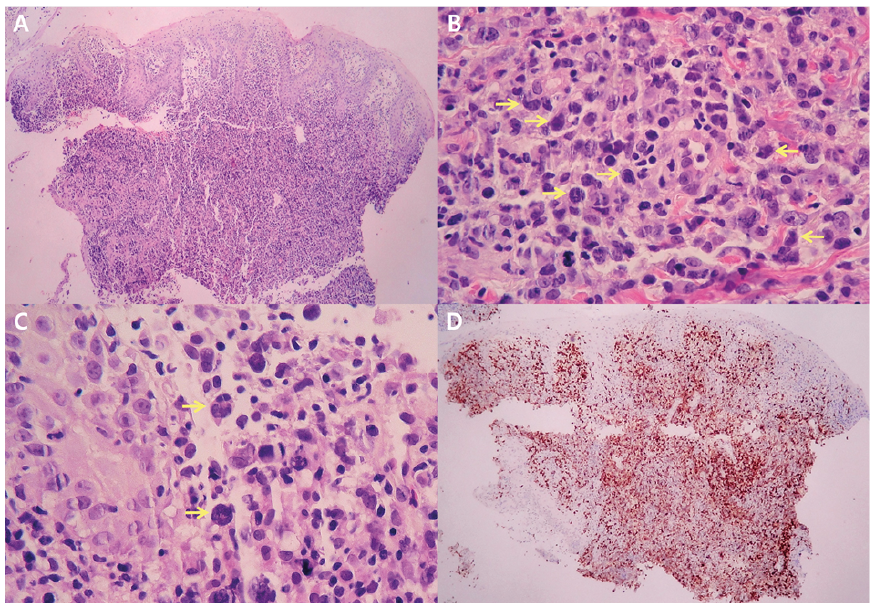 Click to show fullsize
Click to show fullsize