


1Department of Dermatology, Venereology and Allergology, and 2Department of Pathomorphology, Division of Pathomorphology, Wroclaw Medical University, ul. Cha?ubi?skiego 1, PL-50-368 Wroc?aw, Poland. *E-mail: jacek.szepietowski@umed.wroc.pl
Accepted Feb 10, 2020; Epub ahead of print Feb 14, 2020
Acta Derm Venereol 2020; 100: adv00074
Keratoacanthoma (KA) is a common skin tumour in humans. The most common variant of KA is a sporadic and solitary tumour, usually up to 20 mm in diameter; however, the KA centrifugum variant can vary from a few millimetres up to more than 20 cm in diameter (1). Diagnosis of KA is based mostly on the typical clinical presentation of the tumour and rapid growth (weeks to months), with a triphasic course with self-healing. Mature KA is a dome- or bud-shaped well-demarcated, symmetrical nodule with a keratin plug in the centre. KA is typically localized on sun-exposed areas of light-skinned people and shows a tendency to spontaneous resolution (2). Despite the very characteristic clinical picture of KA, careful differential diagnosis is essential, as other malignancies, even highly malignant skin cancers, can mimic the presentation of KA. We report here 2 cases that were initially suspected to be KA, in which histopathology and immunopathology resulted in a final diagnosis of malignant tumours after surgical removal in our dermatosurgery unit in 2019. In both patients differential diagnosis included the possibility of squamous cell carcinoma (SCC) and basal cell carcinoma (BCC).
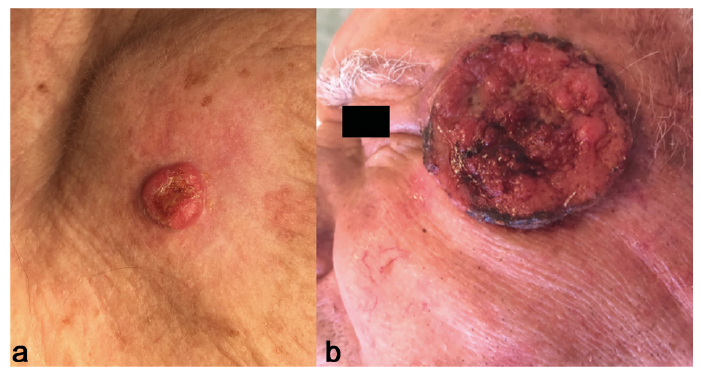
An 89-year-old woman presented with a single, well-demarcated, red nodule, approximately 20 mm diameter, on her left cheek. The central part of the tumour comprised a crater cavity filled with horny masses on a ground-glass milky background (Fig. 1a). The patient reported that the painless, rapidly growing tumour had appeared 5 months previously. There was no trauma, previous birthmark in this area, or accompanying itching in the patient’s history. Apart from the current lesion the patient was healthy, with no history of internal malignancy or family history of skin tumours.
Fig. 1. (a) Case one: Amelanotic melanoma approximately 20 mm diameter on the cheek, presenting as a dome-shaped nodule with a central crater, mimicking a keratoacanthoma (KA). (b) Case two: Squamous cell carcinoma, 60×80 mm, on the temple, presenting as exophytic, well-demarcated, red tumour with coral-reef appearance, mimicking a KA.
Differential diagnosis. The rapidly growing, dome-shaped, centrally ulcerated nodule indicated an initial diagnosis of KA. However, the whitish halo area in the background of the nodule (Fig. 1a) brought this opinion into question. Total excision, with a security margin of 3–5 mm healthy tissue, was performed. Three-dimensional histopathology showed that all surgical margins were free. The excisional defect was repaired with primary closure of the wound. Histopathology revealed an invasive malignant melanoma of a nodular subtype. The Breslow thickness was 5.5 mm, with a Clark level of IV. The histopathological margins were clear. Histologically, the entire lesion was melanoma with ulceration on the surface. Mitotic figures were conspicuous, with a mitotic rate of 8/mm2. Brisk-like lymphocytic infiltration was present. Immunohistochemical studies revealed that the tumour cells were positive for Melan A, HBM-45 and S-100. Ki67 expression in “hot spots” was up to 80%. There was no infiltration of the blood vessels and nerves, and no satellite lesion. The clinical absence of pigmentation led to a diagnosis of amelanotic melanoma (Fig. 2a). The patient was referred to the oncology department for further diagnostics and treatment.
Fig. 2. (a) Case one: Histological features of melanoma (haematoxylin and eosin; H&E×40) formed by atypical pleomorphic melanocytes showing a positive staining reaction for (I) S-100, (II) Melan-A and (III) HBM-45. (b) Case two: Histological features of squamous cell carcinoma (SCC) (H&E×100).
Case two
A 93-year-old man presented with a single, exophytic, well-demarcated, red tumour, 60×80 mm, on his left temple. The entire surface of the tumour was ulcerated, with a bleeding crater in the middle, developing “coral-reef appearance” (Fig. 1b). The patient reported that the itchy, rapidly growing tumour had appeared only 3 months previously. He reported no trauma or previous birthmark in this area. The patient was otherwise healthy, with no history of internal malignancy or family history of skin tumours.
Differential diagnosis. The unusual size of the tumour brought into question the initial diagnosis of KA. However, based on literature, even larger KA had been found, although mostly on lower extremities (1, 3–5). The very rapid growth of the tumour (over the course of 3 months the plaque enlarged to measure up to 80 mm), lead us to a prompt and complete excision of the lesion. The excisional defect was repaired with a full-thickness graft from the right supraclavicular region, with good functional and aesthetic result.
Histological examination (Fig. 2b) revealed moderately differentiated SCC. The tumour was characterized by the presence of malignant cells with large abundant eosinophilic cytoplasm and often vesicular nucleus. Focally, nuclear and cytoplasmic pleomorphism was pronounced and mitotic figures (including abnormal forms) were seen. “Keratin pearls” and scattered individually keratinized cells were also seen. Breslow thickness was 12 mm. Mitotic figures were conspicuous, with a mitotic rate of 4/mm2. The patient was referred to the oncology department for further diagnostics and treatment.
A variety of tumours that can mimic KA have been described; hence careful differential diagnosis, taking into consideration the following tumours, is essential. Nodular melanoma is a relatively uncommon subtype of malignant melanoma (10–15% of all cases), mostly described as a rapidly growing, aggressive tumour with blue or black pigmentation (6). Melanoma with little or no pigmentation represents clinically amelanotic melanoma, which is a very rare subtype of the disease (7). SCC or BCC may be clinically confused with nodular melanoma; however, to date, only 3 cases of melanoma mimicking KA have been described (Table I). Reed et al. (8) described the metastases of malignant melanoma mimicking KA, while the other authors (9, 10) have described primary tumours. Cavicchini et al.(9), in their dermoscopic findings, also described a milky/pinkish background in their patient. Other findings that distinguish clinically amelanotic melanoma are dotted, linear irregular, or polymorphous vessels and milky red globules (11).
Clinical and morphological distinction between KA and SCC may cause difficulties in certain cases. Cutaneous SCC usually present as enlarging scaly or crusted lumps. In dermoscopy, invasive SCC present white nonstructural masses, a central keratotic plug with ulceration, hair-pin and polymorphic vessels (12). Similar attributes are also found in KA, except for irregular linear vessels, which are more commonly encountered in the presentation of SCC.
If there is any clinical doubt in cases of KA, we recommend that the treatment of choice should be surgical removal with histological examination, especially in elderly patients with rapidly growing tumours.
Table I. Cases of malignant melanoma mimicking keratoacanthoma (KA) described in the literature


 Click to show fullsize
Click to show fullsize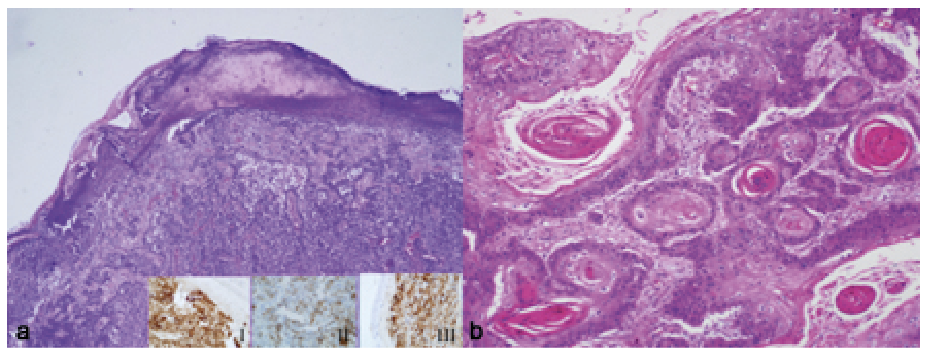 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize