


1Department of Dermatology, Xiangya Hospital, 2Key Laboratory of Organ Injury, Aging and Regenerative Medicine of Hunan Province, 3Department of Social Medicine and Health Management, Xiangya School of Public Health, 4Center for Molecular Medicine, Xiangya Hospital, and 5National Clinical Research Center for Geriatric Disorders, Xiangya Hospital, Central South University, Changsha, Hunan, China
#These authors contributed equally and should be considered as first authors.
The pathogenesis of rosacea remains unclear but has been reported to correlate with skin barrier function. The objective of this study was to elucidate the skincare habits of Chinese adolescents and determine the relationship between skincare habits and rosacea. A university-based cross-sectional investigation included 310 rosacea cases and 3,129 healthy controls who underwent health examinations and completed a questionnaire about daily skincare habits. Fitzpatrick skin phototype IV is a protective factor against rosacea (adjusted adds ratio (aOR) 0.40; 95% confidence interval (CI) 0.22–0.72). Long bath duration (≥ 11 min, aOR 2.60; 95% CI 1.01–6.72) and frequent use of facial cleansers (≥ 2 times/day, aOR 1.70; 95% CI 1.17–2.36) were positively associated with rosacea, but bath frequency (p = 0.22), water temperature (p = 0.53), and sun protection (p = 0.65) were not associated with rosacea. Inappropriate skincare habits, including extended bath durations and frequent use of facial cleansers, significantly increase the risk of rosacea in Chinese adolescents.
Key words: rosacea; skincare habits; skin barrier; adolescent; cross-sectional study.
Accepted Feb 19, 2020; Epub ahead of print Mar 4, 2020
Acta Derm Venereol 2020; 100: adv00081.
Corr: Yiya Zhang and Xiang Chen, Department of Dermatology, Xiangya Hospital, Central South University, Xiangya Road, Changsha, 410008, Hunan, China. E-mails: yiya0108@csu.edu.cn; chenxiangck@126.com.
The association between skincare habits and rosacea in adolescents who rarely use skincare is not clear. In this university-based cross-sectional study, including 310 cases of rosacea and 3,129 healthy controls, long bath durations (≥ 11 min) and frequent use of facial cleansers (≥ 2 times/day) are risk factors for rosacea. Bath frequency and water temperature, as well as sun protection use do not affect rosacea occurrence. Adolescents should try to avoid the overuse of facial cleansers and limit the duration of bathing to reduce the risk of rosacea.
Rosacea is a chronic inflammatory disorder of the facial skin, characterised by various signs and symptoms on the convexities of the central face, and consisting of cycles of remission and exacerbation (1). According to previous investigations, the prevalence of rosacea ranges from less than 1% to up to 22% (2, 3), depending on the population and diagnostic criteria. This disease can lead to significant problems for the patient, including an altered appearance, itchiness, burning, embarrassment (4), social anxiety (5), depression (6), and an overall decreased quality of life (7).
Unfortunately, the pathogenesis of rosacea remains unclear but has been reported to correlate with damaged skin barrier, uncontrolled skin inflammation, immune system anomalies, and neurovascular dysregulation (8). Disruption of the skin barrier function in rosacea patients causes alterations in skin parameters (9), such as dehydration level and trans-epidermal water loss (TEWL) (10, 11). Skin barrier damage, including lipid synthesis disruption and stratum corneum impairment, occurs concomitantly with the classic symptoms of rosacea (12). Some skincare habits disturb the skin barrier; for example, high temperature is reported to dilate facial blood vessels, thereby resulting in an increase in inflammatory factors and a disturbance of skin homeostasis (13, 14). Those who bathe for long durations are prone to suffer increased diuresis and natriuresis caused by increased hydrostatic pressure, and this can lead to dehydration of the skin (15, 16). Moreover, extended sun exposure can lead to excessive penetration of ultraviolet light through the skin barrier, consequently damaging the skin (17, 18).
A previous retrospective case-controlled study by our group showed that skincare habits were significantly associated with rosacea development in Chinese outpatients and indicated that those who more frequently use facial cleansers are more likely to develop rosacea. However, among Chinese adolescents, a population that tends to use fewer skincare products or cosmetics, the link between skincare and rosacea development has not been studied. Furthermore, our previous investigation focused on the use of facial cleansers and sunscreens and did not include bathing habits, such as bath frequency, bath duration, and water temperature. Therefore, we also included these factors in our present study to investigate the association between skincare and rosacea development in adolescents. Since the skin barrier plays such an important role in rosacea, we hypothesised that skincare habits, such as the temperature of water used to wash the face, the use of facial cleansers, and the use of sun protection, may influence the occurrence and development of rosacea. The aims of our study were to summarise the daily skincare habits of Chinese university-based adolescents and to investigate whether these habits are associated with rosacea development.
Study design and participants
This was a cross-sectional study performed at two comprehensive universities (Central South University, Changsha, and Xiamen University, Xiamen) in China, with a geographically dispersed enrolment policy. All newly enrolled students who consented to participate underwent a health examination and responded to an online questionnaire between September and October 2018.
Data collected included demographic information, history of diseases, and living habits. The investigated living habits were those that had been performed for recent two years. The questionnaire survey was organised by the student affairs department of each university. Height and weight were measured by clinical research nurses using standardised methods. Skin phototype was determined, and skin diseases were face-to-face diagnosed by two certificated dermatologists during the physical examination. More details can be found in previous publications of the pilot study in 2017 (19, 20).
Participants diagnosed with rosacea were included in the study. Diagnostic criteria were mainly based on clinical manifestations defined by the National Rosacea Society Expert Committee, which were updated in 2017 (1). As acne is more prevalent in adolescents, investigators gave particular focus to the differences between the papules of rosacea and acne. Dome-shaped red papules with or without accompanying pustules, often in crops and dominant in the centrofacial area, are typical of rosacea. Comedones should be considered a feature of acne. Healthy controls were defined as participants who were free from apparent skin diseases and self-reported systemic diseases. Participants with systemic diseases or skin diseases other than rosacea (such as acne, atopic eczema, psoriasis) were excluded from the analysis. Participants were also excluded if other skin conditions occurred concurrently with rosacea.
Written informed consent was obtained from all participants. The investigation was completed in accordance with the ethical principles originating from the Declaration of Helsinki and was approved by the Medical Ethics Committee of Xiangya Hospital, Central South University.
Statistical analysis
Continuous data are presented as mean ± standard deviation, and between-group differences were tested using analysis of variance. Categorical data are presented as an absolute number (with the percentage (%)), and between-group differences were tested using the chi-square test. Risk factors for rosacea were analysed using two-level logistic models (student as level-1 unit and province as level-2 unit). Odds ratios (ORs) and 95% confidence intervals (CIs) were estimated from the model. Adjusted odds ratios (aORs) and adjusted 95% confidence intervals (aCIs) were further adjusted for all variables. Statistical analysis was performed using SAS 9.4 (SAS Inc., Cary, USA). p < 0.05 was considered statistically significant.
A total of 9,227 newly admitted college students consented to participate and underwent the dermatological examination. Among them, 5,788, who were diagnosed with skin diseases other than rosacea or who reported systematic diseases were excluded from the analysis, leaving 310 cases of rosacea and 3,129 healthy controls.
Analysis of participant demographics and skincare habits
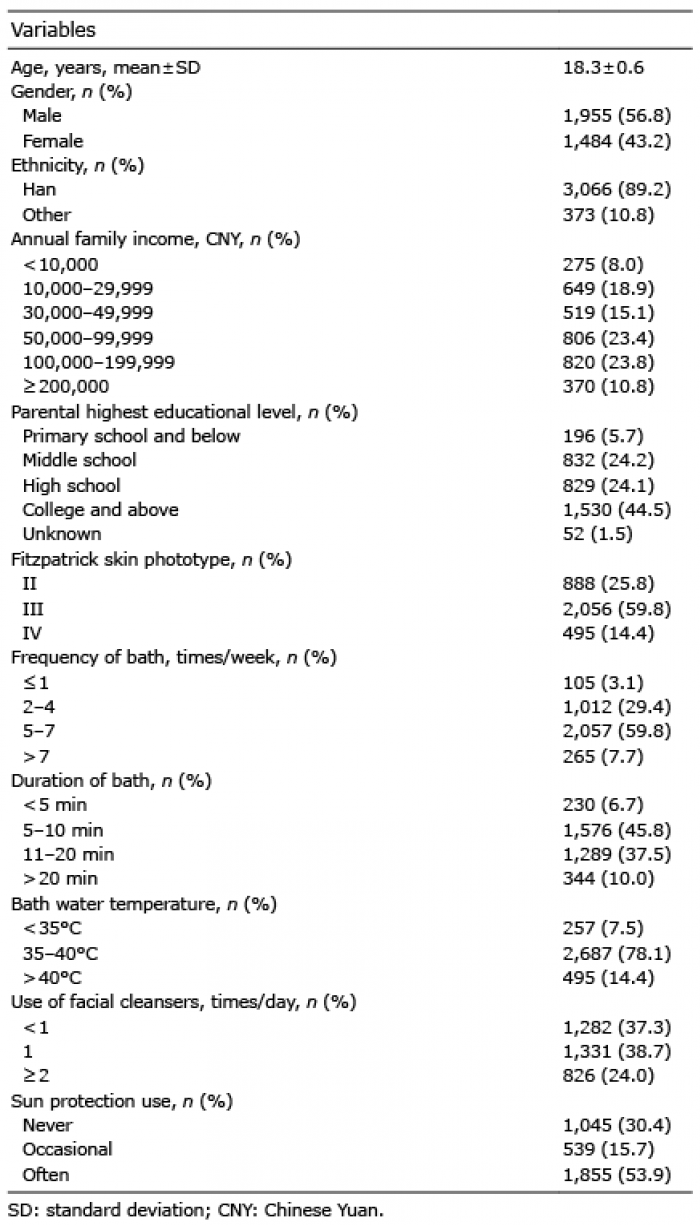
Age and sex were not significantly different between the 3,439 included and 5,788 excluded subjects. Of the 3,439 included participants, the mean age was 18.3 ± 0.6 years, and the male: female ratio was 1.32:1. In the rosacea group, the mean age was 18.2 ± 0.7 years and the male: female ratio was 1.35:1. The participants predominantly belonged to the Han Chinese ethnic group (89.2%). The distribution of skincare habits is listed in Table I.
Table I. Analysis of participant demographics and skincare habits
Associations between skincare habits and rosacea
Age, sex, ethnicity, family income, and parental education level were not significantly different between rosacea cases and healthy controls (Table II). Fitzpatrick skin phototype (Table III) was associated with rosacea (ptrend = 0.001), and phototype IV (Table IV) was a protective factor against rosacea (aOR 0.40, 95% CI 0.22–0.72). The associations between skincare-related habits were examined (Table III). Longer bath duration (p = 0.02) and frequent use of facial cleansers (p = 0.03) were associated with rosacea (p < 0.05), and the associations showed linear trends (ptrend < 0.05). The identified risk factors were further analysed in two-level logistic models (Table IV).
In model I, after adjusting for demographic variables (age, sex, and family income), longer bath duration (≥ 11 min) (aOR 2.60, 95% CI 1.01–6.72) and more frequent use of facial cleansers (≥ 2 times/day) (aOR 1.66, 95% CI 1.17–2.36) were risk factors for rosacea. When including all significant variables in addition to demographic factors (model II), the effect sizes increased slightly compared to those in model I. Bath frequency (p = 0.22), water temperature (p = 0.53), and the use of sun protection (p = 0.65) were not associated with rosacea prevalence.
Table II. Characteristics of the rosacea cases and healthy controls
Table III. Comparison of skincare habits and characteristics between case and control group
Table IV. Adjusted estimates of skincare habits and characteristics as risk factors for rosacea
To the best of our knowledge, this study is the first to report on the skincare habits among Chinese adolescents and to relate this to rosacea development. College adolescents are a highly heterogeneous population, with many potential confounding variables, including age, education level, and aesthetic standards. However, these variables can be more easily controlled in the population used in this study, since adolescents newly admitted to university are more homogenous with respect to age and education level and are less likely to have developed specific skincare routines. It is, therefore, much easier to exclude external variables. Nevertheless, from our review of the literature, the association between skincare habits and rosacea in adolescents has not been studied before. Such research would help dermatologists not only gain a general understanding of daily skincare habits among adolescents, but also understand the relationship between these habits and rosacea, which might better equip them to treat the earlier stages of rosacea.
Our study primarily investigated the effect of bathing on rosacea in Chinese adolescents and confirmed that bathing for longer durations is a risk factor. Byun et al. (21) reported that bathing for an extended period is likely to wash away natural moisturising factors and intercellular lipids of the stratum corneum, which can cause disruption to the skin barrier. Skin barrier dysfunction may aggravate skin inflammation and lead to abnormal function of the skin’s immune system (22). Persistent skin inflammation further attenuates skin barrier function, thereby driving or aggravating rosacea (23). These findings are consistent with our results regarding bath duration, which suggest that bathing for ≥11 min increases the risk of developing rosacea. Another study found that high temperature can damage the skin barrier as well as increase the blood flow in facial blood vessels, thus increasing the skin’s susceptibility to rosacea development (24). However, we identified no association between water temperature and rosacea in our study; additionally, we speculate that this is because the range of temperatures in our study was narrow, and that the highest temperature in the study was not high enough to increase neurovascular sensitivity and trigger rosacea. The temperature threshold for inducing rosacea remains unknown (22) and requires further investigation. Moreover, bathing frequency had no effect on rosacea development in our study. Indeed, a clinical evaluation has previously shown that even daily bathing (7 times/week) did not increase skin eruptions or worsen symptoms (25), which is consistent with our results.
Many previous studies have primarily focused on evaluating the effect of facial washing products on acne, but little research has been conducted on whether they affect rosacea development. It has been reported that frequent use of facial cleansers damages the skin barrier by removing the lipids produced by sebaceous glands (14). Our research suggests that adolescents overusing facial cleansers (≥2 times/day) have a higher risk of developing rosacea, which is consistent with results from a previous study we conducted in a Chinese outpatient population. Therefore, doctors should advise adolescents not to overuse facial cleansers in order to decrease the risk of rosacea.
Additionally, sun avoidance and the regular use of sunscreen have been shown to reduce TEWL, minimise stinging and erythema, and decrease the risk of rosacea (26, 27). However, we observed that over 50% of the participants in this study often used sunscreen, but this did not act as a protective factor against rosacea. A possible reason for this is that some ingredients of sunscreens, for instance, para-aminobenzoic acid, could irritate the skin and lead to stinging and erythema (28, 29), which would likely aggravate skin inflammation, disturb the skin barrier, and contribute to rosacea development (30, 31). We should, therefore, conduct further investigations into the relationship between sunscreen ingredients and rosacea development.
Although our study preliminarily establishes links between skincare habits and rosacea in Chinese college adolescents, the pathophysiological connections are complex and require further investigations. The limitations of our study include the possible presence of recall bias in self-reported questionnaires, as well as potential bias among investigators. As such, the cause-effect relationship and their directionality may become obscured. Therefore, our results should be considered as hypothesis-generating and require further prospective studies to prove or disprove these hypotheses. Moreover, more detailed evaluations of skincare products should be conducted, by classifying types of facial cleansers and skin status, and investigations may need to be stratified accordingly.
In conclusion, our study presents, for the first time, the basic features of skincare habits in Chinese adolescents and provides evidence that supports the link between skincare habits and rosacea. Dermatologists should be aware of these associations and should provide adolescents with appropriate advice, such as avoiding the overuse of facial cleansers and limiting the duration of bathing, to reduce the prevalence of rosacea in this population.
We are grateful to all participants and staff of student affairs department in both universities for their effort in this study. We would like to thank Editage (www.editage.cn) for English language editing. We also thank all the investigators at the Department of Dermatology and Public Health who participated in the field survey.
This work was supported by grants from the National Natural Science Foundation of China (81703149, 81602784, 81502709), Science and Technology Aid Program of Xinjiang Uygur Autonomous Region (2019E0289).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize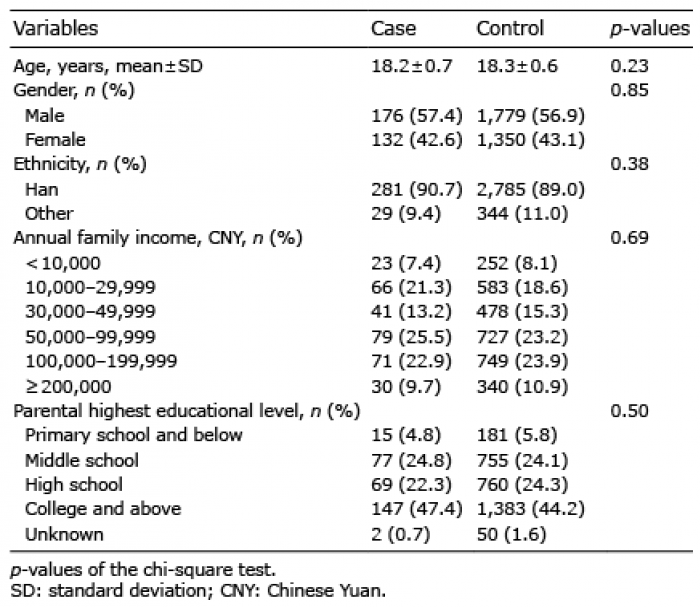 Click to show fullsize
Click to show fullsize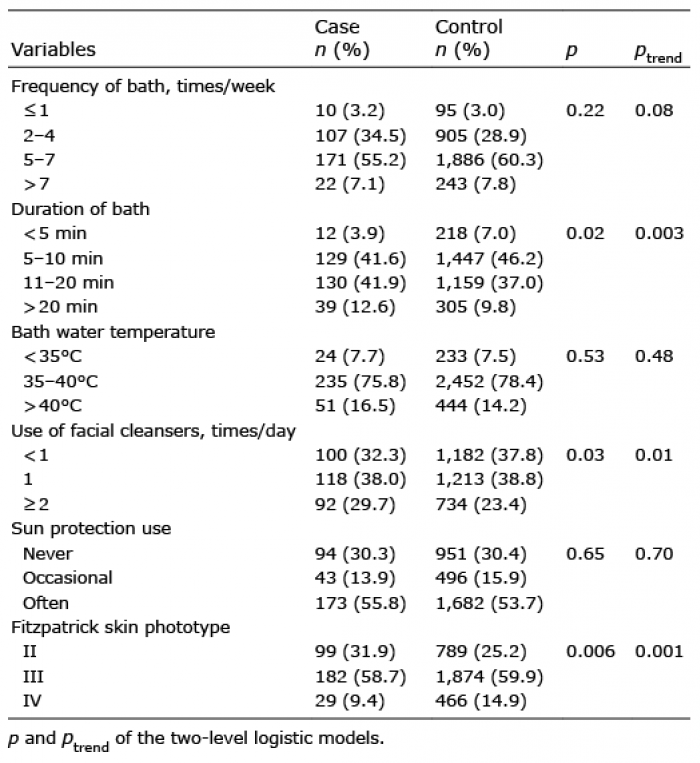 Click to show fullsize
Click to show fullsize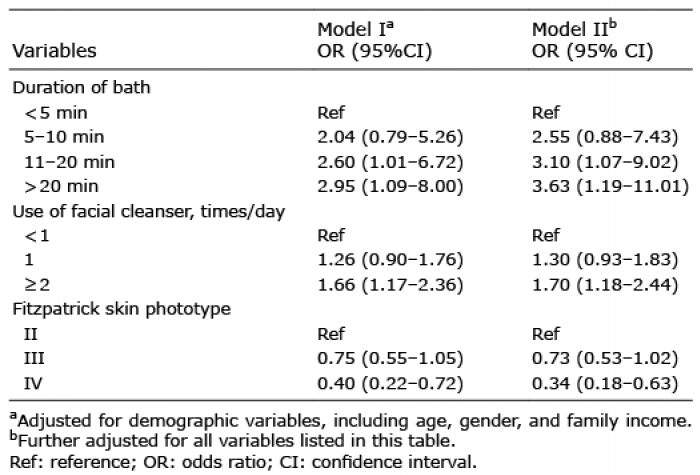 Click to show fullsize
Click to show fullsize