


1Columbia University Vagelos College of Physicians and Surgeons, New York, USA, 2Department of Dermatology, 4Pathology Department and 5Hematological Oncology, APHP, Saint-Louis Hospital, and 3Université de Paris, INSERM U976, Paris, France. *E-mail: martine.bagot@aphp.fr
#These authors contributed equally.
Accepted Jun 16, 2020; Epub ahead of print Jun 18, 2020
Inflammatory skin conditions may present with patches, plaques, and nodules that mimic other skin diseases, including lymphomas (1). Cutaneous lymphomas, especially indolent cutaneous B-cell lymphomas, may present with similar clinicopathological features. Molecular studies may not be consistent with the aetiology of the conditions. It is important to distinguish these entities to provide optimal therapy.
Primary cutaneous marginal zone B-cell lymphoma (MZL) is a proliferation of cells ranging from plasma cells to marginal zone B cells (2). Affecting young adults, it presents as multiple red-violaceous plaques or nodules, preferentially on the trunk and arms (3). On biopsy, patchy, nodular, or diffuse infiltrates are seen with sparing of the epidermis, typically CD20+, CD79+ and bcl-2+ (4, 5). Light chain restriction (LCR) is found by immunohistochemistry and clonality by PCR. Lupus erythematosus tumidus (LET) is a form of cutaneous lupus that is characterized by non-scarring, erythematous, succulent, urticaria-like plaques without surface changes (6). Similar to MZL, biopsy classically shows perivascular and periadnexal lymphocytic infiltration.
Here we present 2 cases of young female patients with challenging diagnoses of LET initially diagnosed as MZL. Clinicopathological correlation led to diagnosis of LET and a change in treatment resulted in improvement. These cases highlight the importance of considering LET in cases of difficult to treat MZL.
Case 1. A 19-year-old female was referred to us in 2010 for evaluation of papulonodules on the right arm since 2006, concerning for MZL (Fig. 1). Diagnostic evaluation at an outside hospital was inconclusive. Biopsies in 2007 and 2009 were comparable in architecture without disturbance of the epidermis, moderately dense lymphocytic infiltrates of small-medium-sized cells present across the entire dermis and in the upper subcutis. The infiltrates were perivascular, occasionally periadnexal, without fat necrosis (panniculitis less likely). The majority of lymphocytes were CD3+ and some CD20+. Rare CD138+ plasma cells were dispersed, Ki67 was normal. There was no evidence of lymphocyte clonality, LCR, or lymphoid follicles. Biopsy was difficult to interpret, read as LET or pseudolymphoma.
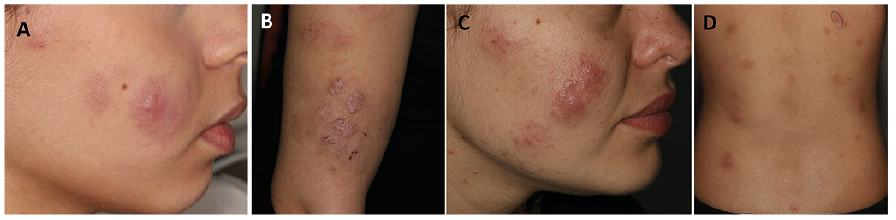
Fig. 1. Papulonodules and plaque in Patient 1 on the (A) right cheek and (B) arm and in Patient 2 on the (C) right cheek and (D) back. The clinical similarities can be seen between these 2 patients.
The patient was referred to the Saint-Louis Hospital in July 2010. A complete autoimmune work-up was negative (antinuclear antibody (ANA) 1:80, anti-extractable nuclear antigen (ENA) and dsDNA negative). Clinicopathological correlation favoured a diagnosis of LET, and empirical treatment with hydroxychloroquine (HCQ, 200 mg/day) was initiated in September 2010. HCQ was self-discontinued after one month, although it was well tolerated.
Repeat biopsy in December 2010 showed a normal epidermis with conserved papillary structures and some orthokeratosis. There were no vacuoles on the basal membrane or keratinocyte necrosis, but dermal oedema and a weak perivascular infiltrate. The infiltrate was composed of small lymphocytes at the dermal-subcutaneous junction and eosinophils. Immunofluorescence showed granular C3 deposits along the dermo-epidermal junction and no IgA or IgG deposits. Chloroquine (250 mg/day) was initiated in December 2010, but was discontinued after 7 days due to development of urticarial lesions. HCQ (200 mg/day) was initiated in January 2011 for 4 months without improvement. Another biopsy in June 2011 showed normal epidermis, conserved papillary structures, without vacuoles at the basal layer. In the dermis, there was moderately dense infiltration of small lymphocytes, histiocytes, and plasma cells at the dermal-subcutaneous junction, along the capillaries. The infiltrate was composed of 60% CD3+ T lymphocytes (70% CD4+, 30% CD8+), 40% CD20+ B lymphocytes, and CD68+ histiocytes. It was read as non-specific lymphohistiocytic infiltrate with an important B-cell component unusual for lupus (Fig. S1). Topical desonide (mild corticosteroid) treatment and doxycycline (100–200 mg/day) was initiated because of anti-inflammatory properties in October 2011 and continued for 2 months without disease progression. Thalidomide (50–100 mg/day) was started in April 2013 under strict contraception, was well tolerated and led to significant improvement. At the 2-year follow-up improvement persisted and the treatment was continued.
Case 2. A 20-year-old female was referred to us in 2019 for evaluation and management of papulonodules on the trunk, thighs, and face since 2015. Three biopsies at an outside hospital between January and September 2018 showed a dermal infiltrate comprised of B- and T-cells read as MZL vs pseudolymphoma. Despite lack of clonality or LCR, diagnosis of MZL was validated by clinicopathological correlation and the strong B-cellular lymphocytic infiltrate as to the WHO – European Organization for Research and Treatment of Cancer (EORTC) classification in October 2018.
Treatment with rituximab was started in October 2018 (375 mg/m2 4×/week then maintenance therapy every 2 months). Symptoms persisted after 2 months, and the patient was referred to us. Complete work-up included an autoimmune panel (all negative) and a skin biopsy (April 2019), read as LET. Morphology showed preserved thickness of the epidermis and perivascular infiltrate across the entire dermis with small lymphocytes and some eosinophils. Immunohistochemistry showed CD3+ lympho-cytes with occasional B lymphocytes (CD79+, PAX5+). The B lymphocytes were CD20–, probably secondary to treatment with rituximab. A few follicular helper T cells (TFH) were observed (PD1+, ICOS+, BCL6+, focal CXCL13+) and a large population of CD123+ plasmocytoid dendritic cells clustered over the dermis. There was no LCR, clonality was negative. Given the diagnosis of LET, the patient began treatment with prednisolone (30 mg/day and tapered) and chloroquine (200 mg/day) for one month with symptom improvement, but due to side-effects it was discontinued. Because of the high response rate, our previous experience showing rapid response, and the cosmetically perturbing lesions, we initiated treatment with thalidomide under strict contraception. Lesions improved significantly after 6 weeks and the patient will continue follow-up.
These cases demonstrate the overlap in clinical presentation and histology of LET and MZL, highlighting the difficulty in distinguishing inflammatory skin conditions from cutaneous malignancies (Table SI). These cases demonstrate the importance of LCR and clonality in establishing a diagnosis of MZL (4). Although these features were absent on biopsy for both patients, a diagnosis of MZL was made clinically.
Clinical presentation was similar; neither patient had photosensitivity. Lymphoid infiltrate with B cells lead to initial diagnosis of MZL vs pseudolymphoma. This perivascular-periadnexal lymphocytic infiltration is also seen in LET, without epidermal involvement (6, 7).
Treatment for case 1 included HCQ, chloroquine, doxycycline, and fourth-line thalidomide. Anti-malarial agents are first-line treatments for LET (6). Case 1 did not progress after HCQ and chloroquine treatment, although both were stopped early. The patient responded to thalidomide, which is used for the treatment of cutaneous lupus refractory to conventional treatments (8). The second patient was treated with rituximab due to the given diagnosis of MZL, without efficacy. This was changed to prednisolone, chloroquine, and, subsequently, thalidomide, leading to improvement.
Histology highlights the difficulty in distinguishing these conditions. TFH and CD123+ cells, both of which are seen in B-cell lymphomas, were observed in the second case (9, 10). Features of the biopsies that may be more suggestive of LET include no LCR, polyclonal B and T-cell populations, and presence of eosinophils (11). Mucin deposition is typically seen in LET (7), but this was not reported in the biopsies. LET can occur with or without systemic involvement (12).
These cases highlight the difficulty of distinguishing MZL from LET and other inflammatory skin conditions, including Jessner’s lymphocytic infiltrate, both clinically and histopathologically, and suggest the importance of considering LET in cases of discrete dermal infiltrates. Distinguishing it from Jessner’s lymphocytic infiltrate is extremely challenging, although LET is characterized by abundant mucin deposition and immunofluorescence is positive for C3 in most cases, as described in case 1. Clinicopathological correlation is essential in difficult cases, and it is important to reconsider the diagnosis of MZL if refractory to standard therapies and of atypical evolution.
GD is a recipient of the EADV Young Researcher Fellowship (www.eadv.org).


 Click to show fullsize
Click to show fullsize