


1Division of Dermatology, 4Institute of Pathology, Rabin Medical Center, Beilinson Hospital, 2Laboratory for Molecular Dermatology, Felsenstein Medical Research Center-Tel Aviv University, Petach Tikva, 3Sackler School of Medicine, Tel Aviv University, Tel Aviv, 5Cancer Research Center, and 6Department of Dermatology, Sheba Medical Center, Tel Hashomer, Israel
Recent studies suggest that folliculotropic mycosis fungoides (FMF), the most common variant of mycosis fungoides (MF), presents with 2 distinct clinicopathological stages: early indolent stage and more aggressive advanced/tumour stage. To further characterize these stages, miR-155 expression was studied with qRT-PCR and found to be significantly higher in biopsies of tumour-stage FMF compared with early-stage FMF and inflammatory dermatoses. There was no statistically significant difference in miR-155 expression between early-stage FMF and early-stage MF, nor between tumour-stage FMF and tumour-stage MF. Immunohistochemical analysis revealed a significantly increased number of dermal Ki-67+ proliferating lymphocytes in tumour-stage FMF, together with an increased number of CD20+ B cells and CD68+ macrophages compared with early-stage FMF. Thus, similar to classic MF, miR-155, Ki-67 tumour cell immunoreactivity, and certain tumour-infiltrating inflammatory cells are differentially expressed in early- vs tumour-stage FMF. The results of this study corroborate the notion that FMF presents with 2 distinct stages.
Key words: folliculotropic mycosis fungoides; stage, microRNA-155; cutaneous T-cell lymphoma; Ki-67; microenvironment.
Accepted Jun 16, 2020; Epub ahead of print Jun 18, 2020
Acta Derm Venereol 2020; 100: adv00230.
Corr: Emmilia Hodak, Division of Dermatology, Rabin Medical Center – Beilinson Hospital, Petach Tikva 4941492, Israel. E-mail: hodake@post.tau.ac.il
Folliculotropic mycosis fungoides, the most common variant of mycosis fungoides, was recently suggested to present with 2 distinct stages: early-stage and advanced/tumour-stage, each with different prognostic implications. To gain further insight into the different presentations of folliculotropic mycosis fungoides, skin biopsies of folliculotropic mycosis fungoides were studied for miR-155 expression, a well-documented cancer promoter in classic mycosis fungoides, the proliferation marker Ki-67 expression, and the composition of the inflammatory infiltrate. This study shows that, similar to classic mycosis fungoides, expression of miR-155, dermal Ki-67 immunoreactivity, and the number of tumour-infiltrating B-cells and macrophages are also increased in a stage-dependent manner in folliculotropic mycosis fungoides.
Folliculotropic mycosis fungoides (FMF), the most common variant of mycosis fungoides (MF), is characterized by follicle-based lesions, with folliculotropism as the histopathological hallmark, as opposed to epidermortropism in classic MF. Since the course of FMF was found by several groups to be comparable with that of tumour-stage MF, researchers have proposed that FMF should be considered tumour-stage (1–6). However, we have shown recently that, in fact, FMF presents with 2 distinct clinicopathological features, representing an early stage and an advanced/tumour stage, each with different prognostic implications (7). These findings were further validated by the Dutch Cutaneous Lym-phoma Group (8). Early FMF is characterized by more superficial clinical features and less heavy perifollicular infiltrates than advanced/tumour-stage FMF. While the course of early FMF is indolent, similar to that of classic early-stage MF, and patients may respond to skin-targeted therapy, tumour-stage FMF has a more aggressive course similar to classic tumour-stage MF, and requires more aggressive treatments (7–10).
MicroRNAs (miRNAs) are evolutionarily conserved small single-stranded non-coding RNA molecules that regulate gene expression by either messenger RNA degradation or inhibition of translation (11). Oncogenic features of miR-155 have been documented in MF, and a significant upregulation of miR-155 was found, specifically in tumoural MF (11–17). Furthermore, our group and others showed that the progression of MF from early- to tumour-stage is associated with upregulation of miR-155 (15, 18), and it may also serve as a prognostic marker (17). The molecular background of FMF has hardly been investigated. In the only 2 published small series higher expression of miR-155 was found in FMF compared with inflammatory dermatoses (19, 20). While in one report the FMF cases studied were defined as advanced-stage (20), in the other report no further details were given (19). Whether miR-155 is associated with tumour progression of FMF is unknown. Studies have shown that the tumour progression of MF in general is associated with increased expression of proliferation markers (17, 21–24), and a change in the immunological milieu with an increase in the number of several non-malignant immune cells (25). Likewise, our previous histopathological study, based on haematoxylin and eosin (H&E) staining, has demonstrated that the presence of eosinophils and, less significantly, the presence of plasma cells and granulomatous reaction, are stage-dependent, and are more frequently found in tumour-stage FMF compared with early-stage FMF (7).
The aim of the present study was to gain further insight into the different stages of FMF, by: (i) exploring miR-155 expression in early- and tumour-stage FMF; (ii) studying whether the Ki-67 nuclear proliferation antigen is stage dependent; and (iii) extending the previous study by evaluating the composition of the infiltrates using several immunohistochemically markers for tumour and tumour-associated inflammatory cells.
Study population
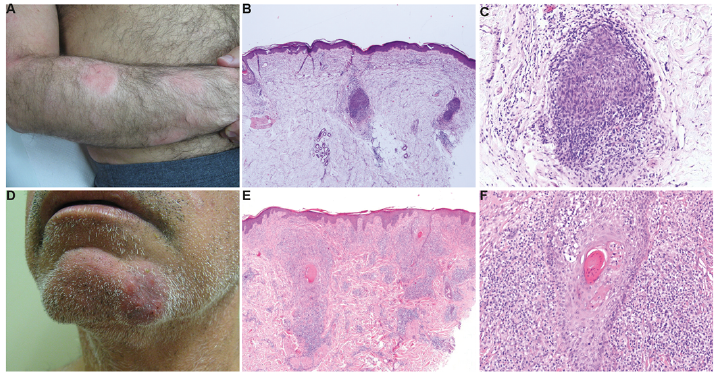
The study was approved by the Institutional Review Board and complied with the principles of the Declaration of Helsinki. Formalin-fixed paraffin-embedded (FFPE) skin biopsies from patients with FMF and classic MF and from inflammatory dermatoses diagnosed at the tertiary Cutaneous Lymphoma Clinic of Rabin Medical Center were used. MF and FMF were defined according to the World Health Organization-European Organization for Research and Treatment of Cancer (WHO-EORTC) classification for cutaneous lymphomas (1). FMF cases were classified into early-stage FMF and tumour-stage FMF according to newly defined clinicopathological criteria described in detail in our recent report (Table SI) (7). In brief, clinically, patients with early-stage FMF present with follicle-based patch/flat plaques, keratosis pilaris-like lesions, and/or acneiform lesions, often associated with alopecia, and are usually located in the trunk and/or limbs region. These clinical findings are combined histologically with intrafollicular and sparse or lichenoid perifollicular infiltrates of atypical lympho-cytes that are confined to the adventitial perifollicular dermis. Patients with tumour-stage FMF present with infiltrated plaques, nodules or tumours, often associated with alopecia, and are preferentially located on the head and/or neck area. These clinical lesions have, in general, heavier perifollicular infiltrates, that are at least lichenoid, but often with more nodular or diffuse pattern, extending to the reticular dermis. A proportion of the FMF cases characterized in our previous report served for the present study according to the availability of adequate residual FFPE tissue (7). All were non-transformed cases. Examples of clinicopathological features of early- and tumour-stage FMF are shown in Fig. 1.
Fig. 1. Clinicopathological presentations of folliculotropic mycosis fungoides (FMF). Early-stage FMF: (A) Hairless erythematous patches and flat plaques located on the outer aspect of the forearm. (B) Biopsy specimen shows 3 hair follicles surrounded by sparse to patchy lichenoid infiltrates (haematoxylin and eosin (H&E); original magnification ×20). (C) Magnification of the central hair follicle shows significant folliculotropism (H&E; original magnification ×100). Tumour-stage FMF: (D) Hairless infiltrated erythematous plaque located on the chin. (E) Biopsy specimen shows 2 hair follicles surrounded by heavy lichenoid infiltrates extending to the reticular dermis in a nodular pattern (H&E; original magnification ×20). (F) Magnification of E shows significant folliculotropism (H&E; original magnification ×100).
RNA extraction
RNA was extracted from 20 10-µm-thick sections of each sample using the miRNeasy FFPE kit (Qiagen, Hilden, Germany).
MicroRNA quantitative polymerase chain reaction
Skin biopsies from untreated 14 patients with early-stage and 13 patients with tumour-stage FMF were studied for miR-155 expression and compared with biopsies from classic early-stage (n = 14) and tumour-stage (n = 19) MF. Biopsies from T-cell-rich inflammatory dermatoses (n = 29) served as controls and included lichen planus (LP, n = 8), discoid lupus erythematosus (DLE, n = 7), and the follicular-based disease lichen planopilaris (LPP, n = 14). Relative quantification of mature miR-155 expression was analysed using the individual TaqMan microRNA™ assay for hsa-miR-155 (Applied Biosystems, Foster City, CA, USA) on 100 ng total RNA, as described previously (15). Briefly, specific stem-loop reverse transcription primers were used to reverse-transcribe mature microRNA, followed by quantitative PCR, that was performed in triplicate on a StepOne platform (Applied Biosystems, Foster City, CA, USA). U6 was used as an expression normalizer. Data were interpreted with Sequence Detection Systems (SDS) software version 1.2.3. We used our mir-155 expression data in tumour-stage MF and in LP and DLE from our previous study (15).
Immunohistochemistry
Histopathological sections were stained with anti Ki-67 (RM9106, 1:200, Thermo Scientific, Fremont, CA, USA); anti CD20 (1:400, Agilent Dako, Santa Clara, CA, USA), anti CD68 (1:150, Agilent Dako), anti CD30 (1:30, Agilent Dako), and anti TOX (HPA018322, 1:100, Sigma-Aldrich, Zwijndrecht, The Netherlands). Slides were evaluated by a highly experienced dermatopathologist (M.F.). The dermal infiltrate was evaluated semi-quantitatively and scored for percentage of immunopositive cells from a minimum of 3 representative medium-power fields, as follows: For CD30, CD20, CD68 and Ki-67: ≤ 5%, 6–10%, 11–20%, ≥ 21%. For TOX: ≤5%, 6–33%, 34–66% and ≥ 67%. The number of cases stained with each antibody is shown in Table I.
Statistical analysis
SPSS v. 21 was used for analysis. A p-value < 0.05 was considered significant. Statistical differences between ΔCt values were calculated using unpaired Student’s t-test assuming normal distribution. In case of statistical significance, a post-hoc Mann–Whitney U test was performed. The fold change in miR-155 expression level (relative quantification; RQ) was calculated using the following equation: RQ=mean 2(–ΔCt tested group)/mean 2(–ΔCt reference group). For immunohistochemical studies the Mann–Whitney U test or Fisher’s exact test were used for comparison of 2 groups, as appropriate.
Expression of miR-155 is significantly higher in tumour-stage folliculotropic mycosis fungoides compared with early-stage folliculotropic mycosis fungoides
miR-155 expression in early-stage and tumour-stage FMF, early-stage and tumour-stage MF, and inflammatory dermatoses is presented in –ΔCt (Fig. 2A) and in fold change (RQ) (Fig. 2B). Since there was no difference in miR-155 expression between LP, DLE and LPP (Fig. S1), they were grouped together for further analysis.
The expression level of miR-155 was significantly higher in tumour-stage FMF compared with early-stage FMF (Fig. 2A), with a fold change of 10.75 (Fig. 2B). miR-155 expression in tumour-stage FMF was also significantly higher compared with early-stage MF (p = 0.01) and inflammatory dermatoses (p = 0.01, Fig. 2A). There was no significant difference in miR-155 expression between early-stage FMF and early-stage MF (Fig. 2A), nor between tumour-stage FMF and classic tumour-stage MF (p = 0.5, Fig. 2A). miR-155 expression was significantly higher in classic tumour-stage MF and T-cell-rich inflammatory dermatoses than in early-stage FMF (Fig. 2A) with fold changes of 26.96 and 4.53, respectively (Fig. 2B).
Fig. 2. miR-155 expression in folliculotropic mycosis fungoides (FMF), classical mycosis fungoides (MF) and T-cell-rich inflammatory dermatoses. (A) Expression level of miR-155 as measured by miRNA qPCR in early-stage FMF (n = 14), tumour-stage FMF (n = 13), early-classic MF (n=14), tumour-stage MF (n = 19) and inflammatory dermatoses (n = 29). Delta Ct for each group was calculated and represented by –ΔCt. Horizontal bars represent the –ΔCt mean for each patients group. ****Statistically significant difference in ΔCt compared with early-stage FMF with p < 0.0001. (B) The fold change of miR-155 expression using early-stage FMF as the reference group. Values above the bars represent the fold change. ns: non-significant; RQ: relative quantification.
Significantly greater number of dermal Ki-67, CD20 and CD68 positive cells are observed in tumour-stage folliculotropic mycosis fungoides compared with early-stage folliculotropic mycosis fungoides
Table I summarizes the immunophenotypical results. There was a significantly increased number of Ki-67-positive lymphocytes, presumably representing the proliferating lymphoma cells, in the dermis of tumour-stage FMF compared with early-stage FMF (Fig. 3A). While two- thirds of the early cases had less than 5% positivity, and only one- third had greater than 10% positivity, the distribution of the immunoreactivity in tumour-stage was less polarized, still more than half of the cases had at least 10% positivity.
Table I. Immunohistochemical characteristics of the dermal infiltrates in early- vs. tumour-stage folliculotropic mycosis fungoides (FMF)
Fig. 3. Immunohistochemistry for Ki-67, CD20 and CD68 in early- and tumour-stage folliculotropic mycosis fungoides (FMF). (A) Increased number of Ki-67 positive lymphocytes in the dermis of tumour-stage folliculotropic mycosis fungoides compared with early-stage FMF. (B) Increased number of CD20+ B cells (C) and CD68+ macrophages in tumour-stage FMF compared with early-stage FMF. Representative pictures from each group (original magnification ×100).
Positivity for CD20, a B-cell marker, was significantly higher in tumour-stage FMF compared with early-stage FMF (Fig. 3B). While 92% of early-stage FMF had up to 10% positivity, in tumour-stage FMF there was a relatively equal distribution between the different categories of staining intensity, thus 50% expressed up to 10% and 50% above this level.
Positivity for CD68, a marker for macrophages, was significantly higher in tumour-stage FMF compared with early-stage FMF (Fig. 3C). While all cases of early-stage FMF had up to 20% positivity of the dermal infiltrate, with most of the cases up to 10%, the infiltrate of the majority of tumour-stage FMF expresses strong immunoreactivity, i.e. more than 20% of the dermal cells had positivity.
For CD30 and TOX, no statistically significant difference was found between early- and tumour-stage FMF.
The present study was prompted by recent new insights regarding FMF, suggesting that it presents with 2 clinicopathological stages: the early indolent and the more aggressive advanced/tumour stage (7, 8). This study showed that, in analogy to classic MF, biopsies of early- and tumour-stage FMF exhibit distinct molecular features, with an increased expression of the miR-155 in tumour-stage compared with early-stage FMF, accompanied by an increased number of Ki-67+ proliferating dermal lymphocytes, and an increased number of the tumour-associated inflammatory cells.
An earlier study by our group demonstrated that miR-155 is selectively overexpressed by malignant lymphoma cells in biopsy samples from tumour-stage MF compared with early-stage MF, suggesting its role in tumour progression (15). This in vivo observation is in line with the findings suggesting that miR-155 contributes to the proliferation of MF cells in vitro (24), and with our more recent in vitro and ex vivo findings that miR-155 expression is functionally important in the development of MF tumours through contributing to increased tumour growth (26). In addition, miR-155 was found to have a poor prognostic implication in cutaneous T-cell lymphoma, including MF (17). These findings provided support to the development of an anti-miR-155 treatment for MF (27, 28). Little is known about the role of microRNAs in general and miR-155 in particular in FMF. In 2 previous reports of overall 16 cases of FMF as a group, miR-155 expression was found to be overexpressed compared with inflammatory dermatoses (19, 20). The current study is the first to distinguish between miR-155 expression in early-stage and tumour-stage FMF. The increased miR-155 expression in tumour-stage FMF compared with early-stage FMF and inflammatory dermatoses, as observed in the present study, together with the results of the 2 previous reports (19, 20), provide a rationale to evaluate anti-miR-155 treatment in FMF and, specifically, in the tumour-stage. No significant difference was found in miR-155 expression between tumour-stage FMF and classic tumour-stage MF. Likewise, a previous comparison between 9 cases of FMF and 7 cases of classic tumour MF failed to detect a difference (19). Thus, it is most likely that the cases studied in that study, although not specified in the manuscript, included only tumour-stage cases of FMF. In contrast, in another study on FMF, increased miR-155 expression was found in 7 cases, defined as advanced cases, compared with 29 cases of tumour-stage MF (20). The discordant results may be explained by difference in clinicopathological patient selection and the small size of the cohorts.
Interestingly, higher levels of miR-155 were found in T-cell-rich inflammatory dermatoses compared with early-stage FMF. This might be attributable to the relatively sparse lymphocytic infiltrate surrounding the involved hair follicles in early-stage FMF (6, 8), and the dilution of the miR-155 signal due to cell admixture.
The proliferative status, as evidenced by the immunoreactivity of the proliferation marker Ki-67, has been reported to be increased in advanced-stages of MF (21–24) and was also found to serve as a marker of poor prognosis (17). Similar to classic MF, significantly higher numbers of Ki-67 dermal lymphocytes were found in tumour-stage FMF compared with early-stage FMF. Importantly, a new prognostic model in CTCL including MF, combining the expression of both miR-155 and Ki-67, was suggested recently (17). Moreover, the presence of more than 10% Ki-67 positive cells was found to be a prognostic factor in plaque-stage FMF (29).
In addition to tumour cells, the inflammatory microenvironment plays an important role in cancer biology, including MF. Here, by applying immuno-histochemistry, we showed that the number of infiltrating B cells and macrophages in FMF are stage-dependent, thus extending our previous observation demonstrating increased presence of plasma cell and granulomatous reaction in tumour-stage compared with early-stage FMF (7).
While the presence of B cells in MF has been noted in early reports (30, 31), it was only in a recent analysis of 33 cases of MF that a positive correlation was demonstrated with its advanced stages. Moreover, there was a significant correlation of B-cell infiltrates and shortened progression-free survival (32). Remarkably, all the 5 cases of FMF included in that study had increased median B-cell numbers compared with classic MF, suggesting that those cases, in fact, would be classified as tumour-stage FMF (32). Preclinical data indicate that B cells may exert a pro-tumourigenic effect by their ability to promote an immunosuppressive milieu through releasing factors that promote tumour growth (33). Notably, 2 patients with FMF showing significant B-cell infiltrates were treated with either intralesional or systemic rituximab and experienced a sustained remission, suggesting that local depletion of B cells can re-establish immunological tumour control (32, 34).
Macrophages are a major component of the infiltrates in the tumour microenvironment and play a role in tumour development and progression in several cancers (35, 36). In line with our present study, Sugaya et al. detected more dermal CD68+ macrophages as MF progressed through patch, plaque- and tumour-stages (36). The so-called tumour-associated macrophages (TAMs) possess many, although not necessarily all, of the features of macrophages cultured in vitro in the presence of Th2 cytokines and express CD163 (M2 macrophages). Sugaya et al. demonstrated that the number of CD68+ cells overlapped the number of CD163+, not only in MF specimens but also in other inflammatory dermatoses, such as atopic dermatitis and psoriasis, and suggested that CD163 might be a marker of macrophages in the skin rather than a marker of M2 macrophages. Thus, although we have not stained FMF specimens with CD163, it is possible that the results would not differ from their observation.
There was no significant difference in CD30 immunoreactivity between the FMF stages. This is in contrast with at least one study of MF in which CD30-positivity in non-transformed MF was found to be significantly associated with a higher clinical stage (24). The lack of difference in our cohort could be attributed to the small number of cases that were included in the analysis. Finally, the current study did not demonstrate significant differences in TOX (thymocyte selection associated high-mobility group box protein expression, a nuclear CD4+ factor, which is essential for the development of T cells in the thymus) between early- and tumour-stage FMF. Immunohistochemical studies, assessing the correlation between TOX and tumour progression in MF in general, yielded contradictory results, some suggesting that overexpression is correlated with thicker lesions (37, 38), while others did not (39).
In conclusion, the results of this study support the recent notion that FMF presents with 2 distinct clinicopathological stages. For the first time it was shown that, similar to classic MF expression of miR-155, Ki-67 immunoreactivity and the number of tumour-infiltrating B cells and macrophages are also increased in a stage-dependent manner in FMF. Whether any of these markers can serve as an independent prognostic indicator in FMF is a subject for further research.
This study was supported by Katzenelnbogen Foundation, the Sackler Faculty of Medicine, Tel Aviv University.
The study was presented in part at the EORTC Cutaneous Lym-phoma Task Force meeting in London, October, 2017.


 Click to show fullsize
Click to show fullsize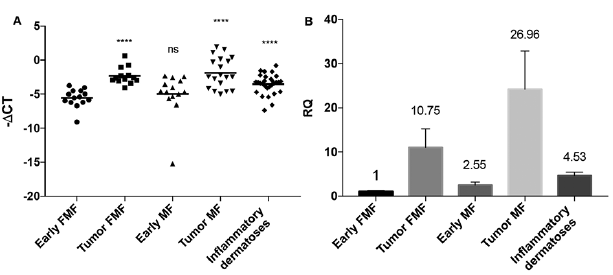 Click to show fullsize
Click to show fullsize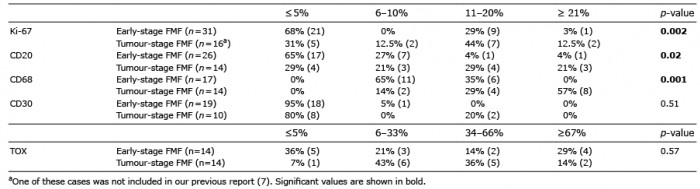 Click to show fullsize
Click to show fullsize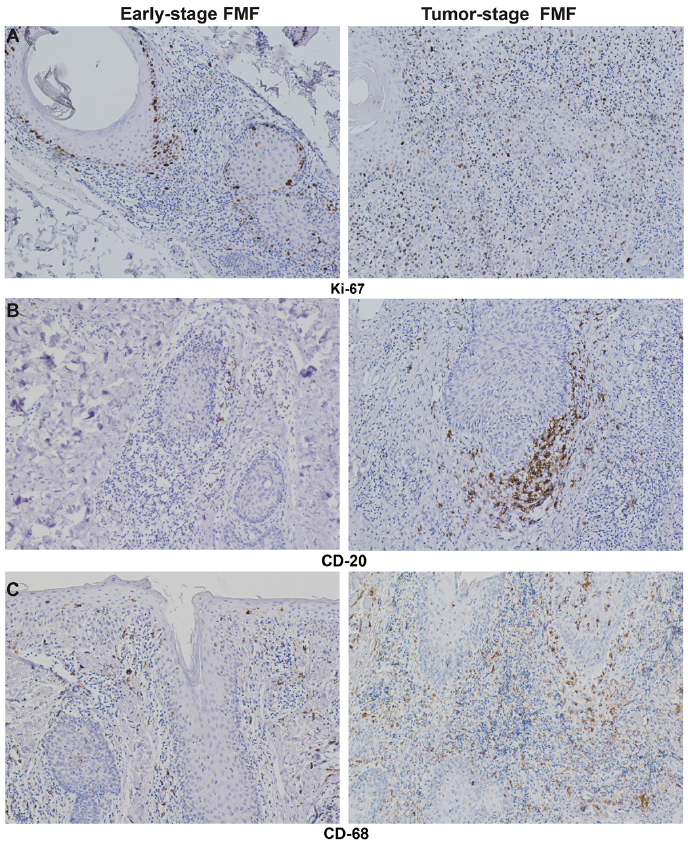 Click to show fullsize
Click to show fullsize