


1L?beck Institute of Experimental Dermatology, University of L?beck, L?beck, Germany, 2Ben-Gurion University of the Negev, 3Department of Medical Psychology and Psychotherapy, Medical University of Graz, Graz, Austria, 4Siaal Research Center for Family Medicine and Primary Care, Division of Community Health, Faculty of Health Sciences, Ben-Gurion University of the Negev, Beer-Sheva, Israel, 5Dermatology Clinic, Padua University Hospital, Padua, Italy, 6Faculty of Health Sciences, Ben-Gurion University of the Negev, Beer-Sheva, Israel, and 7Chief Physician’s Office, Clalit Health Services, Tel Aviv, Israel
#These authors contributed equally.
Data regarding the association between psoriasis and dementia are inconclusive. The aim of this study was to evaluate this association in the database of Clalit Health Services, Israel. A comparative analysis for the association between psoriasis, dementia and its risk factors was performed for the entire study population and in the subgroup of patients with moderate-to--severe psoriasis. The study included 121,801 patients with psoriasis, of whom 16,947 were diagnosed with moderate-to-severe psoriasis, and 121,802 controls. Psoriasis was associated with a lower prevalence of dementia relative to control subjects (1.6% vs 1.8%; odds ratio (OR) 0.85; 95% confidence interval (95% CI) 0.80–0.91; p < 0.001). Multivariate analysis adjusting for demographic variables, cardiovascular-related risk factors, and healthcare utilization demonstrated a significant inverse association between psoriasis and dementia in the entire study population (adjusted OR 0.86; 95% CI 0.76–0.96; p = 0.009), but not in the subgroup of patients with moderate-to-severe psoriasis (adjusted OR 0.91; 95% CI 0.81–1.02; p = 0.113). In conclusion, these data support the hypothesis that psoriasis is inversely associated with dementia.
Key words: psoriasis; dementia; obesity; hypertension; diabetes; hyperlipidaemia; depression.
Accepted Jul 7, 2020; Epub ahead of print Jul 29, 2020
Acta Derm Venereol 2020; 100: adv00250.
Corr: Dennis Linder, Department of Medical Psychology, Psychotherapy and Psychosomatics, Medical University of Graz, AT-8036 Graz, Austria. E-mail: michael.dennis.linder@gmail.com
Psoriasis, a chronic inflammatory skin disease, often presents with other diseases, such as cardiovascular disease, depression, etc. Little is known about the relationship between psoriasis and dementia, and the frequency of dementia in people with psoriasis compared with those without psoriasis. To evaluate the association between psoriasis, dementia and dementia-related risk factors, this study compared data from more than 120,000 patients with psoriasis with that from similar individuals without psoriasis. The results indicate that patients with psoriasis have a lower risk of developing dementia. The high number of patients studied implies that these results reflect the actual situation.
Dementia is one of the leading causes of premature death in the Western world. In recent years, it has been shown that dementia is associated not only with chronic inflammation, but also with an aberrant immune response (1).
In psoriasis, systemic inflammation, particularly cytokines including tumour necrosis factor (TNF)-α and interleukin (IL)-17, play an important role (2, 3). As dementia and psoriasis are both associated with chronic inflammation and an abnormal immune response, a poss-ible association between psoriasis and dementia might be suspected. However, conclusive data regarding this possible association are lacking. A further assessment of such association is highly warranted given the high burden of both conditions.
Numerous studies have shown an association between dementia and metabolic syndrome; however, it is difficult to establish the nature of a hypothetical causal relation-ship between dementia and metabolic syndrome. Also, assuming there is a linear causal relationship, it is not clear which is the cause and which the consequence (1, 4).
The aim of the current study was to evaluate the association between psoriasis, dementia and dementia-related risk factors (4–7): obesity, hypertension, diabetes, hyperlipidaemia, and depression, utilizing the large medical database of Clalit Health Services (CHS), Tel Aviv, Israel.
Settings and dataset
Data-mining techniques were used in the CHS database. CHS is the largest healthcare provider organization in Israel, serving a population of more than 4,400,000 enrolees (8). CHS has a comprehensive computerized database with continuous real-time input from pharmaceutical, medical, and administrative operating systems, which facilitates epidemiological studies, such as the current analysis.
In the CHS, consultations with specialists (i.e. dermatologists) can be performed in 3 different settings: in-patient settings (i.e. with hospitalization or during an emergency-room visit without hospitalization); out-patient settings, in which the out-patient clinic is affiliated with a hospital; and primary-care settings, also referred to as a community setting, in which the consultation is performed outside the hospital setting by a board-certified specialist who has no affiliation with any hospital. To capture the real-life picture the current study approach was based on the community setting.
The diagnoses investigated in the present study were extracted from the CHS chronic diseases registry. The chronic diseases registry is subjected to a continuous validation process based on repeated appraisal of diagnoses made by CHS physicians in any setting, registered prescriptions, pharmacy claims, laboratory tests, and auxiliary tests for each patient. Comparisons between diagnoses, drug administration, laboratory, and auxiliary tests from various sources are performed repeatedly, and inconsistencies between records are resolved after authentication by the registry manager. In this registry, the diagnosis of dementia includes several disorders under the spectrum of the disease; all of which are continuously validated by a comparison between physicians, prescriptions, pharmacy claims, laboratory tests, and auxiliary tests, etc. for the same patient, and only when a diagnosis is fully validated according to all sources is it registered in the chronic disease register. The accuracy of the CHS chronic disease register has been documented in a previous publication (9). Data regarding outcomes, i.e. diagnoses of dementia, obesity, hypertension, diabetes, hyperlipidaemia, and depression, were extracted from the CHS Chronic Disease Register.
The study was approved by the institutional review board of Soroka University Medical Center, Beer Sheva, Israel. Publication of the data was approved by the institutional ethical committee of CHS general management (0212-17-COM).
Study population and covariates
The database has been used to study patients with psoriasis, and the methodology has been described previously (10, 11). In the current cross-sectional study patients were defined as having psoriasis when there was at least one documented diagnosis of psoriasis in the medical records registered by a CHS dermatologist in the primary-care setting or when psoriasis was listed in the diagnoses of discharge letters from a hospital affiliated with CHS between January 2002 and December 2016. The control group was frequency matched, with sex, age, and ethnicity matched to cases, and was randomly selected from the general population enrolees in the CHS, excluding patients with a diagnosis of psoriasis. The 2 groups were compared with regard to the lifetime prevalence of dementia.
Data regarding the severity of psoriasis were not available for this study and, therefore, disease severity was assessed based on healthcare utilization and pharmacy claims. Patients with psoriasis were considered to have moderate-severe disease if they had at least one hospitalization due to psoriasis exacerbation or at least one course of systemic psoriasis-related medications: acitretin, methotrexate, cyclosporine, etanercept, infliximab, adalimumab, ustekinumab, with more than 2 succeeding prescriptions over a period of more than 4 weeks, or phototherapy treatment or dead-sea climatotherapy prescribed in the indication of psoriasis.
Potential covariates included age, sex, smoking status (current smoking vs no current smoking), ethnicity (Arab, other), socioeconomic status (low, medium, high), and Charlson’s comorbidity score (score range 0–24). Outcomes measures were controlled for the following metabolic variables (hypertension, diabetes mellitus, hyperlipidaemia, and body mass index (BMI)) since these may impose a risk of the development of vascular dementia. We additionally adjusted for depression, since it may be the presenting symptom of dementia.
Outcome measures were also adjusted for overutilization of health services, to ensure that observed associations were not merely due to increased or decreased ascertainment. Healthcare utilization was determined by the number of total dermatological visits per individual in the year before the diagnosis of psoriasis in cases and the enrollment date in control subjects. The study outcomes were also adjusted for exposure to acitretin and methotrexate, as there are data suggesting a protective role of these drugs against the development of dementia (12).
Statistical analysis
The study population was subdivided according to disease severity and was categorized into the entire group of patients with psoriasis and a group of patients with moderate-to-severe psoriasis and their matched comparison group. The distribution of patient’s characteristics was compared between patients with and without psoriasis using the χ2 test for sex and smoking status and the t-test for age. The proportions of patients with dementia were compared between the study groups in the entire study sample, as well as in a stratified analysis based on psoriasis severity using the χ2 test. The presence of effect modification was identified using Breslow–Day test. Odds ratios (OR) and 95% confidence intervals (95% CI) are also presented. A logistic regression model was used to measure the association between psoriasis and dementia in a multivariate analysis. Statistical analysis was performed using SPSS software, version 15 (SPSS, Armonk, NY: IBM Corp.).
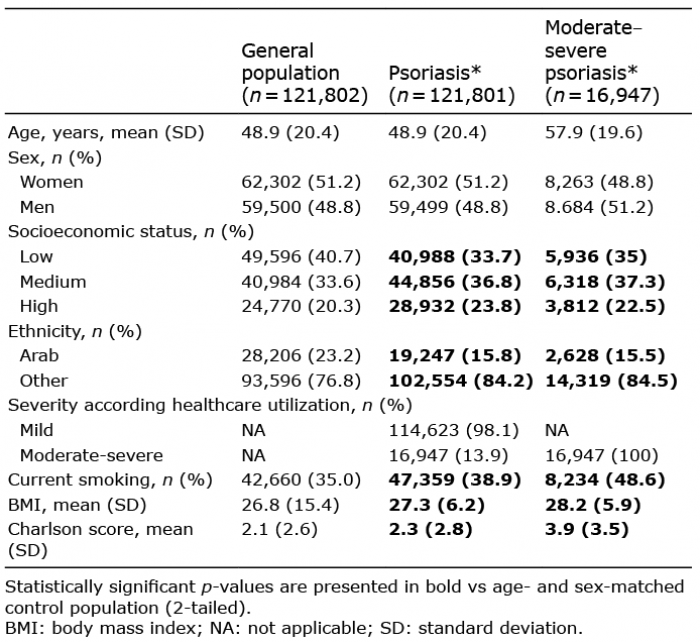
The study included 121,801 patients with psoriasis and 121,802 age- and sex-matched controls. Among cases, 16,947 (13.9%) patients had moderate-to-severe psoriasis. Descriptive analyses of the characteristics of case and control patients are shown in Table I. The mean age in the group of patients with psoriasis was 48.9 years, and in the group of patients with moderate-to-severe psoriasis 57.9 years. Compared with the control population, patients with psoriasis and moderate-to-severe psoriasis had higher rates of high and medium socioeconomic status, higher BMI and comorbidities (Charlson’s score), and were more likely to smoke. The psoriasis group had more patients of non-Arab origin (Table I).
Table I. Baseline characteristics of the study population
The prevalence of dementia in patients with psoriasis was significantly lower than in the control group (1.6% vs 1.8%, respectively; OR 0.85; 95% CI 0.80–0.91; p < 0.001). However, other comorbidities such as obesity, hypertension, diabetes, hyperlipidaemia, and depression were significantly more prevalent among patients with psoriasis (Table II).
Table II. Association between psoriasis, dementia and related risk factors and comorbidities by univariate analysis
Table III presents the association between psoriasis and dementia in the entire study population, as well as among patients with moderate-to-severe psoriasis following the adjustment for putative confounding factors. After controlling for demographic variables, psoriasis had an independent inverse association with dementia, both in the general population of patients with psoriasis (OR 0.83; 95% CI 0.77–0.88) and among those with moderate-to-severe disease (OR 0.80; 95% CI 0.71–0.89). After controlling for the demographic variables, metabolic variables (BMI, hypertension, hyper-lipidaemia, and diabetes), healthcare utilization, and exposure to acitretin and methotrexate, a significantly inverse association persisted in the general population of patients with psoriasis (OR 0.86; 95% CI 0.76–0.96), but not among patients with moderate-to-severe disease (OR 0.91; 95% CI 0.81–1.02).
Table III. Logistic regression results for the association between psoriasis and dementia
This large-scale cross-sectional study revealed an inverse association between psoriasis and dementia, with psoriasis patients being less likely to have dementia than age- and sex-matched controls without psoriasis. This association retained its statistical significance in a sensitivity analysis including moderate-to-severe patients as well as in a multivariate analysis adjusting for potential confounders, including age, depression and cardiovascular risk factors (13).
While the cardiovascular and metabolic profile of patients with psoriasis has been well characterized, there is a shortage of knowledge regarding neurological comorbidities, particularly dementia, in psoriasis. These findings are in contrast with a recent UK population-based cohort study that examined the risk of developing different types of dementia subsequent to admission to hospital with a diagnosis of psoriasis, among other immune-related diseases (14). In that study, patients with psoriasis were shown to be at a 29% and 43% increased risk of developing any dementia and vascular dementia, respectively. A weaker association was observed with Alzheimer’s disease, with only 8% increased risk (14). An excessive mortality due to dementia (hazard ratio (HR) 3.64) was observed among 3,603 patients with psoriasis relative to matched controls in another UK population-based cohort study (15). A recent systematic review pooled data from 16,574 psoriasis cases across 11 observational studies (6 of which were deemed methodologically weak). This narrative synthesis found that 9 of the 11 eligible studies found a significant positive association between the psoriasis and dementia, one study a null association, and one study an inverse association (16).
In a recent hospital-based case-control study of 41 Italian patients with psoriasis, greater prevalence of mild cognitive impairment (MCI) was observed among cases compared with among control subjects (17). MCI includes disturbances in episodic memory, and is considered an intermediate stage between normal cognitive function-ing and dementia (17). Seven of these patients were submitted to cortical thickness analysis by high-field magnetic resonance imaging, and exhibited reduction in brain thickness in parahippocampal, superior temporal and frontal gyri of the left hemisphere (17). Correspondingly, another case-control study of 97 Polish patients with psoriasis revealed that these patients scored lower than controls in cognitive neuropsychological tests assessing memory and executive functions (18).
The association between Alzheimer’s disease and psoriasis has been investigated on the genetic level. In a genetic epidemiology study, a single-nucleotide polymorphisms was associated with both Alzheimer’s disease and psoriasis (19). In addition, the Apo e4 allele, which is considered as the main genetic risk factor for the sporadic form of Alzheimer’s disease, has also been associated with chronic plaque psoriasis (20).
The increased prevalence of mental impairment among patients with psoriasis has been ascribed to the increased risk of cerebrovascular events rendering patients susceptible to vascular dementia (21). It is well-established that cardiovascular risk factors, which were found to associate prominently with psoriasis (22), increase the risk of dementia in a dose-dependent fashion, suggesting a cumulative effect of these factors on neuronal stress (17, 23). In addition, a chronic inflammatory state characterized by increased levels of C-reactive protein and pro-inflammatory cytokines, as in psoriasis, has been linked with cognitive impairment and the development of dementia (24, 25). The increased prevalence of depression in patients with psoriasis may pose another putative risk factor for dementia (26, 27).
The findings of this population-based study are, on the other hand, in agreement with 2 recent reports (27, 29). In a recent Italian study of 318 psoriatic participants, Pezzolo et al. (28) found that the cognitive test scores and volumetric, microstructural, focal measures on brain magnetic resonance imaging (MRI) did not differ between psoriasis and non-psoriasis participants, and that psoriasis was not significantly associated with MCI (adjusted OR 0.87; 95% CI 0.53–1.43). The same study found that patients with psoriasis were at a reduced risk of developing dementia (HR 0.50; 95% CI 0.28–0.91).
Recent evidence accumulated to suggest a negative association between Alzheimer’s disease and retinoids, vitamin A derivatives utilized widely as a systemic treatment for psoriasis (12). Vitamin A and other retinoids were proved to directly inhibit the formation of amyloid fibrils in vivo (12). An increasing body of evidence indicates the presence of retinoid signalling in diverse brain areas, including the amygdala, cortex, hypothalamus, hippocampus, suggesting its involvement in adult brain functions. Impaired retinoid signalling has been evidenced in the pathology of Alzheimer’s disease. Vitamin A-deprived mice present with severe deficiencies in spatial learning and memory, signifying the profound role of vitamin A in preserving memory functions (30, 31). Given that the negative association of psoriasis with dementia was robust in a sensitivity analysis including patients with moderate-to-severe psoriasis receiving systemic therapies (including acitretin, with 1,920 patients exposed to acitretin in the current study), as well as to a multivariate analysis adjusting for acitretin, the current study does not imply that retinoids may account for the observed negative association. Further longitudinal studies are required to explore the effect of these agents in the neurological comorbidities of patients with psoriasis.
Pezzolo et al. (28) have also suggested that disease-modifying antirheumatic drugs, especially methotrexate, may also exert a protective role against the development of dementia, as was previously proven among patients with rheumatoid arthritis. This possibility is yet to be determined in patients with psoriasis (32). Similarly, the current study does not imply a meaningful protective role of methotrexate, since the inverse association persisted following adjustment for this variable in multivariable logistic regression analysis. Under-diagnosis of dementia among patients with psoriasis, due to limited access to healthcare facilities, was ruled-out when the negative association remained significant following the adjustment for healthcare utilization.
The large sample size provides a high level of precision for an exact estimate of the association between relatively uncommon conditions, that are otherwise difficult to compare. The population-based setting reduced the likelihood of selection bias, which can be encountered in hospital-based studies. The study limitations include the lack of data concerning the clinical features and severity of both diseases and the specific type of dementia. The utilization of routinely collected data does not enable a direct validation of diagnoses. However, it is unlikely that a significant differential misclassification would have interfered meaningfully with the findings. The diagnosis of psoriasis is of high validity, since it was grounded on the registration of trained dermatologists. Previous studies based on the CHS database have shown high reliability of data (8, 33). The cross-sectional design interfered with drawing a conclusion regarding the existence of a causal relationship, since the current study compared the lifetime prevalence of dementia among psoriatic patients and controls without addressing the temporal sequence in which these conditions appeared. Absence of information regarding psoriasis subtype and morphological features embodies an additional drawback of the current study.
In conclusion, this study of population-based large-scale data demonstrates that psoriasis is inversely associated with dementia. Further observational studies are necessary to confirm these findings and replicate them in longitudinal cohorts in different study populations. This inverse relation is thought-provoking and will contribute to our understanding of the pathogenesis of both conditions.
The authors would like to thank Katie Palmers for her valuable comments.
Conflicts of interest: ADC received research grants from Novartis. In the last 3 years, he served as a consultant, advisor, or speaker to Abbvie, Dexcel Pharma, Janssen, Novartis, Perrigo, Pfizer, and Rafa. All other authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize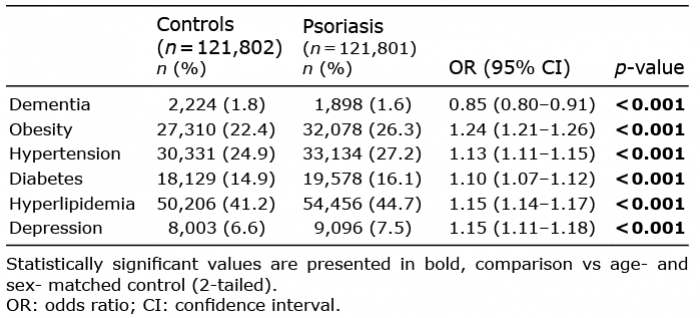 Click to show fullsize
Click to show fullsize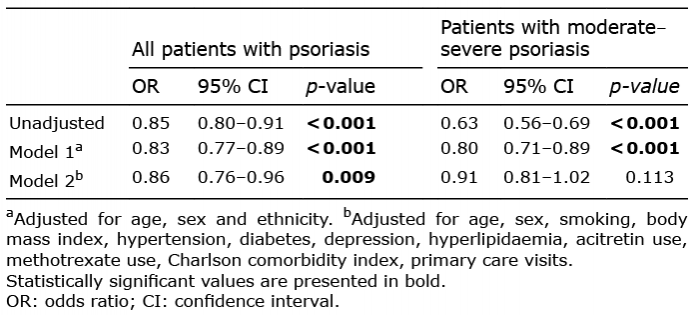 Click to show fullsize
Click to show fullsize