


1Department of Dermatology and Allergy, 2Institute of Pathology, University Hospital of Munich (LMU), Frauenlobstrasse 9–11, DE-80337, Munich, and 3Institute of Human Genetics, Medical Center – University of Freiburg, Faculty of Medicine, University of Freiburg, Germany. E-mail: Kinan.hayani@med.uni-muenchen.de
Accepted Jul 7, 2020; Epub ahead of print Jul 29, 2020
Acta Derm Venereol 2020; 100: adv00241.
Phacomatosis pigmentokeratotica (PPK) is clinically defined by the co-occurrence of an organoid naevus of sebaceous differentiation and a speckled lentiginous naevus. Based on clinical associations and mutational analysis, PPK is currently considered a clinical variant of Schimmelpenning-Feuerstein-Mims syndrome (SFMS). Neoplasia arising in sebaceous naevi are not uncommon with age, but are rarely malignant.
Twenty years ago, a 23-year-old patient was referred to our department. He had 10 systematized linear lesions of sebaceous naevus (SN) on the scalp, face, neck and sternum, and 6 lesions of papular naevi spili on the torso (Fig. 1a–c) and no other cutaneous or extracutaneous manifestations. We had previously reported the case as phacomatosis pigmentokeratotica (1). In 2013, a mutation was found in the HRAS gene in the SN and several lesions of naevus spilus, and in a trichoblastoma detected at the time on a SN on his scalp (3). The patient was subsequently lost to follow-up, despite our recommendation. He returned 18 years later, aged 41 years, to our outpatient clinic for a recently developed tumour in one of his SN (Fig. 1d). Histopathological workup showed squamous cell carcinoma (SCC), partially with basal cell carcinoma differentiation. Computer tomography revealed metastases in several cervical lymph nodes and both lungs.
Fig. 1. (a–c) Representative lesions of sebaceous naevus and papular naevi spili in a 41-year-old patient with phacomatosis pigmentokeratotica. (d) Squamous cell carcinoma in the naevus sebaceous on the scalp with regional nodal metastasis.
Next generation sequencing (NGS) of 4 genes (HRAS, KRAS, NRAS and PIK3CA) in the SN tissue confirmed the previously reported mutation in the HRAS gene in the current patient (3) in a mosaic setting with a percentage of mosaic portion of 34%. No mutations in the KRAS or NRAS genes, but 2 additional sequence variants in the PIK3CA gene were detected in the SN. The first was a variant of unknown significance (VUS3), whereas the second was a known pathogenic somatic PIK3CA mutation. All mutations were present in a mosaic constellation, and no germline mutations were present in DNA from blood samples.
NGS analysis of the tumour and one lymph node metastasis confirmed the aforementioned HRAS mutation. No PIK3CA mutations, but 2 mutations in the PIK3R1 gene (encoding for the regulatory subunit of PI3K) were found. Furthermore, 2 inactivating mutations in the tumour suppressor genes CDKN2A and TP53 were reported in the tumour and lymph mode metastasis (Table I). The patient died within 2 months due to pulmonal complications of metastatic disease.
Table I. Sequencing results and detected variants. Naevus sebaceous tissue was analysed with an Illumina MiSeq (2×150 bp, paired-end)
Groesser et al. (2) showed, in 2012, that several types of naevi (organoid sebaceous naevi, non-organoid keratinocytic epidermal naevi, congenital melanocytic naevi, and papular speckled lentiginous naevi) share a postzygotic activating mutation in RAS pathway in a multipotent ectodermal progenitor cell. Depending on the developmental stage and fate potential of the mutated cells, different tissue compartments and cell types (sebaceous, keratinocytic and/or melanocytic) can be affected. Of note, these mutations were detected in a mosaic setting in the naevi, but not in blood, buccal mucosa, uroepithelial cells or unaffected skin of these patients (2). In 2013, Groesser and colleagues conducted a study on patients with PPK where they used a SNaPshot multiplex assay for the detection of hotspot mutations of 3 genes: HRAS, PIK3CA and FGFR3. Only a mosaic HRAS mutation was detected in the SN in our patient, not in PIK3CA or FGFR3 genes (3). HRAS is an oncogene and the mutation found in 2013 could serve as an initiating event in multistep carcinogenesis. PIK3CA mutations occurred later in 2018 in the naevus, may have played a role in initiating the malignant evolvement of SN through an uncontrolled activation of the AKT/PI3K pathway. Like-wise, PIK3R1 found in the tumour and the metastasis can serve as an alternative pathway to the activation of the latter pathway.
SCC is rarely detected in sebaceous naevi. In 2 large retrospective studies from France and USA involving 1,303 patients with SN, trichoblastomas (n = 80) and syringocystadenomata papelliferi (n = 63) were the most frequently developed tumours (4, 5). By contrast, cases of SCC (n = 8) were quite rare.
A number of clinically defined epidermal naevus syndromes are described in the literature. The advent of NGS has changed the field by favouring genetically defined disease entities, because remarkable genomic overlap exists between the clinically defined epidermal naevus syndromes. PPK and SFMS are probably better considered as one disorder within the wide spectrum of different diseases called RASopathies (6), rather than different disease entities. Close and vigilant follow up should be recommended for all RASopathy patients, but adherence issues should be considered.


 Click to show fullsize
Click to show fullsize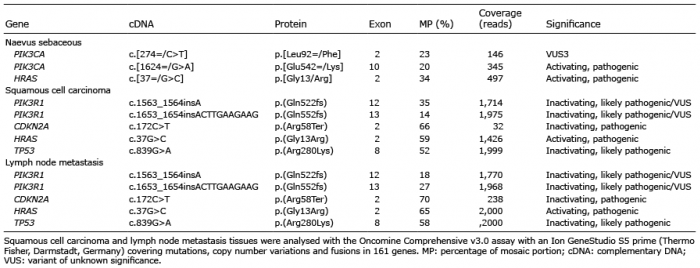 Click to show fullsize
Click to show fullsize